Uterine Fibroid

Uterine fibroids, also known as uterine leiomyomas or fibroids, are benign smooth muscle tumors of the uterus. Most women have no symptoms while others may have painful or heavy periods. If large enough, they may push on the bladder causing a frequent need to urinate. They may also cause pain during sex or lower back pain. A woman can have one uterine fibroid or many. Occasionally, fibroids may make it difficult to become pregnant, although this is uncommon.
The exact cause of uterine fibroids is unclear. However, fibroids run in families and appear to be partly determined by hormone levels. Risk factors include obesity and eating red meat. Diagnosis can be performed by pelvic examination or medical imaging.
Treatment is typically not needed if there are no symptoms. NSAIDs, such as ibuprofen, may help with pain and bleeding while paracetamol (acetaminophen) may help with pain. Iron supplements may be needed in those with heavy periods. Medications of the gonadotropin-releasing hormone agonist class may decrease the size of the fibroids but are expensive and associated with side effects. If greater symptoms are present, surgery to remove the fibroid or uterus may help. Uterine artery embolization may also help. Cancerous versions of fibroids are very rare and are known as leiomyosarcomas. They do not appear to develop from benign fibroids.
About 20% to 80% of women develop fibroids by the age of 50. In 2013, it was estimated that 171 million women were affected worldwide. They are typically found during the middle and later reproductive years. After menopause, they usually decrease in size. In the United States, uterine fibroids are a common reason for surgical removal of the uterus.
Signs and symptoms
Some women with uterine fibroids do not have symptoms. Abdominal pain, anemia and increased bleeding can indicate the presence of fibroids. There may also be pain during intercourse, depending on the location of the fibroid. During pregnancy, they may also be the cause of miscarriage, bleeding, premature labor, or interference with the position of the fetus. A uterine fibroid can cause rectal pressure. The abdomen can grow larger mimicking the appearance of pregnancy. Some large fibroids can extend out through the cervix and vagina.
While fibroids are common, they are not a typical cause for infertility, accounting for about 3% of reasons why a woman may not be able to have a child. The majority of women with uterine fibroids will have normal pregnancy outcomes. In cases of intercurrent uterine fibroids in infertility, a fibroid is typically located in a submucosal position and it is thought that this location may interfere with the function of the lining and the ability of the embryo to implant.
Risk factors
Some risk factors associated with the development of uterine fibroids are modifiable. Fibroids are more common in obese women. Fibroids are dependent on estrogen and progesterone to grow and therefore relevant only during the reproductive years.
Diet
Diets high in fruits and vegetables tend to lower the risk of developing fibroids. Fibers, vitamin A, C and E, phytoestrogens, carotenoids, meat, fish, and dairy products are of unclear effect. Normal dietary levels of vitamin D may reduce the risk of developing fibroids.
Genetics
Fifty percent of uterine fibroids demonstrate a genetic abnormality. Often a translocation is found on some chromosomes. Fibroids are partly genetic. If a mother had fibroids, risk in the daughter is about three times higher than average. Black women have a 3-9 times increased chance of developing uterine fibroids than white women. Only a few specific genes or cytogenetic deviations are associated with fibroids. 80-85% of fibroids have a mutation in the mediator complex subunit 12 (MED12) gene.
Familial leiomyomata
A syndrome (Reed's syndrome) that causes uterine leiomyomata along with cutaneous leiomyomata and renal cell cancer has been reported. This is associated with a mutation in the gene that produces the enzyme fumarate hydratase, located on the long arm of chromosome 1 (1q42.3-43). Inheritance is autosomal dominant.
Pathophysiology

Fibroids are a type of uterine leiomyoma. Fibroids grossly appear as round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and show whorled appearance on histological section. The size varies, from microscopic to lesions of considerable size. Typically lesions the size of a grapefruit or bigger are felt by the patient herself through the abdominal wall.

Microscopically, tumor cells resemble normal cells (elongated, spindle-shaped, with a cigar-shaped nucleus) and form bundles with different directions (whorled). These cells are uniform in size and shape, with scarce mitoses. There are three benign variants: bizarre (atypical); cellular; and mitotically active.
The appearance of prominent nucleoli with perinucleolar halos should alert the pathologist to investigate the possibility of the extremely rare hereditary leiomyomatosis and renal cell cancer (Reed) syndrome.
Location and classification

Growth and location are the main factors that determine if a fibroid leads to symptoms and problems. A small lesion can be symptomatic if located within the uterine cavity while a large lesion on the outside of the uterus may go unnoticed. Different locations are classified as follows:
- Intramural fibroids are located within the muscular wall of the uterus. Unless they are large, they may be asymptomatic. Intramural fibroids begin as small nodules in the muscular wall of the uterus. With time, intramural fibroids may expand inwards, causing distortion and elongation of the uterine cavity.
- Subserosal fibroids are located on the surface of the uterus. They can also grow outward from the surface and remain attached by a small piece of tissue and then are called pedunculated fibroids.
- Submucosal fibroids are most common type, located in the muscle beneath the endometrium of the uterus and distort the uterine cavity; even small lesions in this location may lead to bleeding and infertility. A pedunculated lesion within the cavity is termed an intracavitary fibroid and can be passed through the cervix.
- Cervical fibroids are located in the wall of the cervix (neck of the uterus). Rarely, fibroids are found in the supporting structures (round ligament, broad ligament, or uterosacral ligament) of the uterus that also contain smooth muscle tissue.
Fibroids may be single or multiple. Most fibroids start in the muscular wall of the uterus. With further growth, some lesions may develop towards the outside of the uterus or towards the internal cavity. Secondary changes that may develop within fibroids are hemorrhage, necrosis, calcification, and cystic changes. They tend to calcify after menopause.
If the uterus contains too many to count, it is referred to as diffuse uterine leiomyomatosis.
Extrauterine fibroids of uterine origin, metastatic fibroids
Fibroids of uterine origin located in other parts of the body, sometimes also called parasitic myomas have been historically extremely rare, but are now diagnosed with increasing frequency. They may be related or identical to metastasizing leiomyoma.
They are in most cases still hormone dependent but may cause life-threatening complications when they appear in distant organs. Some sources suggest that a substantial share of the cases may be late complications of surgeries such as myomectomy or hysterectomy. Particularly laparoscopic myomectomy using a morcellator has been associated with an increased risk of this complication.
There are a number of rare conditions in which fibroids metastasize. They still grow in a benign fashion, but can be dangerous depending on their location.
- In leiomyoma with vascular invasion, an ordinary-appearing fibroid invades into a vessel but there is no risk of recurrence.
- In intravenous leiomyomatosis, leiomyomata grow in veins with uterine fibroids as their source. Involvement of the heart can be fatal.
- In benign metastasizing leiomyoma, leiomyomata grow in more distant sites such as the lungs and lymph nodes. The source is not entirely clear. Pulmonary involvement can be fatal.
- In disseminated intraperitoneal leiomyomatosis, leiomyomata grow diffusely on the peritoneal and omental surfaces, with uterine fibroids as their source. This can simulate a malignant tumor but behaves benignly.
Pathogenesis



Fibroids are monoclonal tumors and approximately 40 to 50% show karyotypically detectable chromosomal abnormalities.When multiple fibroids are present they frequently have unrelated genetic defects. Specific mutations of the MED12 protein have been noted in 70 percent of fibroids.
The exact cause of fibroids is not clearly understood, but the current working hypothesis is that genetic predispositions, prenatal hormone exposure and the effects of hormones, growth factors and xenoestrogens cause fibroid growth. Known risk factors are African descent, obesity, polycystic ovary syndrome, diabetes, hypertension, and never having given birth.
It is believed that estrogen and progesterone have a mitogenic effect on leiomyoma cells and also act by influencing (directly and indirectly) a large number of growth factors, cytokines and apoptotic factors as well as other hormones. Furthermore, the actions of estrogen and progesterone are modulated by the cross-talk between estrogen, progesterone and prolactin signaling which controls the expression of the respective nuclear receptors. It is believed that estrogen promotes growth by up-regulating IGF-1, EGFR, TGF-beta1, TGF-beta3 and PDGF, and promotes aberrant survival of leiomyoma cells by down-regulating p53, increasing expression of the anti-apoptotic factor PCP4 and antagonizing PPAR-gamma signaling. Progesterone is thought to promote the growth of leiomyoma through up-regulating EGF, TGF-beta1 and TGF-beta3, and promotes survival through up-regulating Bcl-2 expression and down-regulating TNF-alpha. Progesterone is believed to counteract growth by downregulating IGF-1. Expression of transforming growth interacting factor (TGIF) is increased in leiomyoma compared with myometrium. TGIF is a potential repressor of TGF-β pathways in myometrial cells.
Aromatase and 17beta-hydroxysteroid dehydrogenase are aberrantly expressed in fibroids, indicating that fibroids can convert circulating androstenedione into estradiol. Similar mechanism of action has been elucidated in endometriosis and other endometrial diseases. Aromatase inhibitors are currently considered for treatment, at certain doses they would completely inhibit estrogen production in the fibroid while not largely affecting ovarian production of estrogen (and thus systemic levels of it). Aromatase overexpression is particularly pronounced in African-American women.
Genetic and hereditary causes are being considered and several epidemiologic findings indicate considerable genetic influence especially for early onset cases. First degree relatives have a 2.5-fold risk, and nearly 6-fold risk when considering early onset cases. Monozygotic twins have double concordance rate for hysterectomy compared to dizygotic twins.
Expansion of uterine fibroids occurs by a slow rate of cell proliferation combined with the production of copious amounts of extracellular matrix.
A small population of the cells in a uterine fibroid have properties of stem cells or progenitor cells, and contribute significantly to ovarian steroid-dependent growth of fibroids. These stem-progenitor cells are deficient in estrogen receptor α and progesterone receptor and instead rely on substantially higher levels of these receptors in surrounding differentiated cells to mediate estrogen and progesterone actions via paracrine signaling.
Diagnosis
The presence of a uterine fibroid versus an adnexal tumor is made. Fibroids can be mistaken for ovarian neoplasms. An uncommon tumor which may be mistaken for a fibroid is Sarcoma botryoides. It is more common in children and adolescents. Like a fibroid, it can also protrude from the vagina and is distinguished from fibroids. While palpation used in a pelvic examination can typically identify the presence of larger fibroids, gynecologic ultrasonography (ultrasound) has evolved as the standard tool to evaluate the uterus for fibroids. Sonography will depict the fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam. The location can be determined and dimensions of the lesion measured. Also, magnetic resonance imaging (MRI) can be used to define the depiction of the size and location of the fibroids within the uterus.
Imaging modalities cannot clearly distinguish between the benign uterine leiomyoma and the malignant uterine leiomyosarcoma, however, the latter is quite rare. Fast growth or unexpected growth, such as enlargement of a lesion after menopause, raise the level of suspicion that the lesion might be a sarcoma. Also, with advanced malignant lesions, there may be evidence of local invasion. A biopsy is rarely performed and if performed, is rarely diagnostic. Should there be an uncertain diagnosis after ultrasounds and MRI imaging, surgery is generally indicated.
Other imaging techniques that may be helpful specifically in the evaluation of lesions that affect the uterine cavity are hysterosalpingography or sonohysterography.

A very large (9 cm) fibroid of the uterus which is causing pelvic congestion syndrome as seen on CT
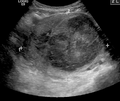
A very large (9 cm) fibroid of the uterus which is causing pelvic congestion syndrome as seen on ultrasound

A relatively large submucosal leiomyoma; it fills out the major part of the endometrial cavity

A small uterine fibroid seen within the wall of the myometrium on a cross-sectional ultrasound view

Two calcified fibroids (in the uterus)

A subserosal uterine fibroid with a diameter of 5 centimeters.

MRI image with multiple uterine leiomiyomas

Giant leiomiyomas almost filling the abdomen.

Histopathology of uterine fibroids typically show smooth muscle in a whorled (fascicular) pattern.

This variant of Van Gieson's stain distinguishes muscle (yellow) from connective tissue (red)










Coexisting disorders
Fibroids that lead to heavy vaginal bleeding lead to anemia and iron deficiency. Due to pressure effects gastrointestinal problems such as constipation and bloatedness are possible. Compression of the ureter may lead to hydronephrosis. Fibroids may also present alongside endometriosis, which itself may cause infertility. Adenomyosis may be mistaken for or coexist with fibroids.
In very rare cases, malignant (cancerous) growths, leiomyosarcoma, of the myometrium can develop. In extremely rare cases uterine fibroids may present as part or early symptom of the hereditary leiomyomatosis and renal cell cancer syndrome.
Treatment
Most fibroids do not require treatment unless they are causing symptoms. After menopause, fibroids shrink, and it is unusual for them to cause problems.
Symptomatic uterine fibroids can be treated by:
- medication to control symptoms (i.e., symptomatic management)
- medication aimed at shrinking tumors
- ultrasound fibroid destruction
- myomectomy or radiofrequency ablation
- hysterectomy
- uterine artery embolization
In those who have symptoms, uterine artery embolization and surgical options have similar outcomes with respect to satisfaction.
Medication
A number of medications may be used to control symptoms. NSAIDs can be used to reduce painful menstrual periods. Oral contraceptive pills may be prescribed to reduce uterine bleeding and cramps. Anemia may be treated with iron supplementation.
Levonorgestrel intrauterine devices are effective in limiting menstrual blood flow and improving other symptoms. Side effects are typically few as the levonorgestrel (a progestin) is released in low concentration locally. While most levongestrel-IUD studies concentrated on treatment of women without fibroids a few reported good results specifically for women with fibroids including a substantial regression of fibroids.
Cabergoline in a moderate and well-tolerated dose has been shown in two studies to shrink fibroids effectively. The mechanism of action responsible for how cabergoline shrinks fibroids is unclear.
Ulipristal acetate is a synthetic selective progesterone receptor modulator (SPRM) that has tentative evidence to support its use for presurgical treatment of fibroids with low side-effects. Long-term UPA-treated fibroids have shown volume reduction of about 70%. In some cases UPA alone is used to relieve symptoms without surgery.
Danazol is an effective treatment to shrink fibroids and control symptoms. Its use is limited by unpleasant side effects. Mechanism of action is thought to be antiestrogenic effects. Recent experience indicates that safety and side effect profile can be improved by more cautious dosing.
Gonadotropin-releasing hormone analogs cause temporary regression of fibroids by decreasing estrogen levels. Because of the limitations and side effects of this medication, it is rarely recommended other than for preoperative use to shrink the size of the fibroids and uterus before surgery. It is typically used for a maximum of 6 months or less because after longer use they could cause osteoporosis and other typically postmenopausal complications. The main side effects are transient postmenopausal symptoms. In many cases the fibroids will regrow after cessation of treatment, however, significant benefits may persist for much longer in some cases. Several variations are possible, such as GnRH agonists with add-back regimens intended to decrease the adverse effects of estrogen deficiency. Several add-back regimes are possible, tibolone, raloxifene, progestogens alone, estrogen alone, and combined estrogens and progestogens.
Progesterone antagonists such as mifepristone have been tested, there is evidence that it relieves some symptoms and improves quality of life but because of adverse histological changes that have been observed in several trials it can not be currently recommended outside of research setting. Fibroid growth has recurred after antiprogestin treatment was stopped.
Aromatase inhibitors have been used experimentally to reduce fibroids. The effect is believed to be due partially by lowering systemic estrogen levels and partially by inhibiting locally overexpressed aromatase in fibroids. However, fibroid growth has recurred after treatment was stopped. Experience from experimental aromatase inhibitor treatment of endometriosis indicates that aromatase inhibitors might be particularly useful in combination with a progestogenic ovulation inhibitor.
Uterine artery
Uterine artery embolization (UAE) is a noninvasive procedure that blocks blood flow to fibroids, causing them to shrink. Long-term outcomes with respect to how happy people are with the procedure are similar to that of surgery. There is tentative evidence that traditional surgery may result in better fertility. One review found that UAE doubles the future risk of miscarriage. UAE also appears to require more repeat procedures than if surgery was done initially. A person will usually recover from the procedure within a few days.
Uterine artery ligation, sometimes also laparoscopic occlusion of uterine arteries are minimally invasive methods to limit blood supply of the uterus by a small surgery that can be performed transvaginally or laparoscopically. The principal mechanism of action may be similar like in UAE but is easier to perform and fewer side effects are expected.
The 2016 NICE (National Institute of Clinical Excellence – the non governmental public body that publishes guidelines in the use of health technologies and good clinical practice in the United Kingdom) guidelines state UAE/UFE can be offered to women with symptomatic fibroids (fibroids being usually >30mm in size). Women should be informed that UAE and myomectomy (the surgical removal of fibroids) may potentially allow them to retain their fertility.
Myomectomy



Myomectomy is a surgery to remove one or more fibroids. It is usually recommended when more conservative treatment options fail for women who want fertility preserving surgery or who want to retain the uterus.
There are three types of myomectomy:
- In a hysteroscopic myomectomy (also called transcervical resection), the fibroid can be removed by either the use of a resectoscope, an endoscopic instrument inserted through the vagina and cervix that can use high-frequency electrical energy to cut tissue, or a similar device.
- A laparoscopic myomectomy is done through a small incision near the navel. The physician uses a laparoscope and surgical instruments to remove the fibroids. Studies have suggested that laparoscopic myomectomy leads to lower morbidity rates and faster recovery than does laparotomic myomectomy.
- A laparotomic myomectomy (also known as an open or abdominal myomectomy) is the most invasive surgical procedure to remove fibroids. The physician makes an incision in the abdominal wall and removes the fibroids from the uterus.
Laparoscopic myomectomy has less pain and shorter time in hospital than open surgery.
Hysterectomy
Hysterectomy was the classical method of treating fibroids. Although it is now recommended only as last option, fibroids are still the leading cause of hysterectomies in the US.
Endometrial ablation
Endometrial ablation can be used if the fibroids are only within the uterus and not intramural and relatively small. High failure and recurrence rates are expected in the presence of larger or intramural fibroids.
Other procedures
Radiofrequency ablation is a minimally invasive treatments for fibroids. In this technique the fibroid is shrunk by inserting a needle-like device into the fibroid through the abdomen and heating it with radio-frequency (RF) electrical energy to cause necrosis of cells. The treatment is a potential option for women who have fibroids, have completed child-bearing and want to avoid a hysterectomy.
Magnetic resonance guided focused ultrasound, is a non-invasive intervention (requiring no incision) that uses high intensity focused ultrasound waves to destroy tissue in combination with magnetic resonance imaging (MRI), which guides and monitors the treatment. During the procedure, delivery of focused ultrasound energy is guided and controlled using MR thermal imaging. Patients who have symptomatic fibroids, who desire a non-invasive treatment option and who do not have contraindications for MRI are candidates for MRgFUS. About 60% of patients qualify. It is an outpatient procedure and takes one to three hours depending on the size of the fibroids. It is safe and about 75% effective. Symptomatic improvement is sustained for two plus years. Need for additional treatment varies from 16-20% and is largely dependent on the amount of fibroid that can be safely ablated; the higher the ablated volume, the lower the re-treatment rate. There are currently no randomized trial between MRgFUS and UAE. A multi-center trial is underway to investigate the efficacy of MRgFUS vs. UAE.
Prognosis
About 1 out of 1000 lesions are or become malignant, typically as a leiomyosarcoma on histology. A sign that a lesion may be malignant is growth after menopause. There is no consensus among pathologists regarding the transformation of leiomyoma into a sarcoma.
Metastasis
There are a number of rare conditions in which fibroids metastasize. They still grow in a benign fashion, but can be dangerous depending on their location.
See extrauterine fibroids.
Epidemiology
About 20% to 80% of women develop fibroids by the age of 50. Globally in 2013 it was estimated that 171 million women were affected. They are typically found during the middle and later reproductive years. After menopause they usually decrease in size. Surgery to remove uterine fibroids occurs more frequently in women in "higher social classes". Adolescents develop uterine fibroids much less frequently than older women. Up to 50% of women with uterine fibroids have no symptoms. The prevalence of uterine fibroids among teenagers is 0.4%.
Europe
The incidence of uterine fibroids in Europe is thought to be lower than the incidence in the US.
United States
Eighty percent of African-American women will develop benign uterine fibroid tumors by their late 40s, according to the National Institute of Environmental Health Sciences. African-American women are two to three times more likely to get fibroids than Caucasian women. In African-American women fibroids seem to occur at a younger age, grow more quickly, and are more likely to cause symptoms. This leads to higher rates of surgery for African Americans, both myomectomy, and hysterectomy. Increased risk of fibroids in African- Americans causes them to fare worse in in-vitro fertility treatments and raises their risk of premature births and delivery by Cesarean section.
It is unclear why fibroids are more common in African American women. Some studies suggest that black women who are obese and who have high blood pressure are more likely to have fibroids. Other suggested causes include the tendency of African American women to consume food with less than the daily requirements for vitamin D.
Related legislation
United States
The 2005 S.1289 bill was read twice and referred to the committee on Health, Labor, and Pensions but never passed for a Senate or House vote; the proposed Uterine Fibroid Research and Education Act of 2005 mentioned that $5 billion is spent annually on hysterectomy surgeries each year, which affect 22% of African Americans and 7% of Caucasian women. The bill also called for more funding for research and educational purposes. It also states that of the $28 billion issued to NIH, $5 million was allocated for uterine fibroids in 2004.
Other animals
Uterine fibroids are rare in other mammals, although they have been observed in certain dogs and Baltic grey seals.
Research
Selective progesterone receptor modulators, such as progenta, have been under investigation. Another selective progesterone receptor modulator asoprisnil is being tested with promising results as a possible use as a treatment for fibroids, intended to provide the advantages of progesterone antagonists without their adverse effects. Low dietary intake of vitamin D is associated with the development of uterine fibroids.