Alcoholic Hepatitis

Alcoholic hepatitis is hepatitis (inflammation of the liver) due to excessive intake of alcohol. Patients typically have a history of decades of heavy alcohol intake, typically 8-10 drinks per day. It is usually found in association with fatty liver, an early stage of alcoholic liver disease, and may contribute to the progression of fibrosis, leading to cirrhosis. Symptoms may present acutely after a large amount of alcoholic intake in a short time period, or after years of excess alcohol intake. Signs and symptoms of alcoholic hepatitis include jaundice (yellowing of the skin and eyes), ascites (fluid accumulation in the abdominal cavity), fatigue and hepatic encephalopathy (brain dysfunction due to liver failure). Mild cases are self-limiting, but severe cases have a high risk of death. Severe cases may be treated with glucocorticoids.
Signs and symptoms
Alcoholic hepatitis is characterized by a number of symptoms, which may include feeling unwell, enlargement of the liver, development of fluid in the abdomen (ascites), and modest elevation of liver enzyme levels (as determined by liver function tests). May also present with Hepatic encephalopathy (brain dysfunction due to liver failure causing symptoms such as confusion, decreased levels of consciousness, or asterixis, (a characteristic jerking of the limbs). Severe cases are characterized by profound jaundice, obtundation (ranging from drowsiness to unconsciousness), and progressive critical illness; the mortality rate is 50% within 30 days of onset despite best care.
Alcoholic hepatitis is distinct from cirrhosis caused by long-term alcohol consumption. Alcoholic hepatitis can occur in patients with chronic alcoholic liver disease and alcoholic cirrhosis. Alcoholic hepatitis by itself does not lead to cirrhosis, but cirrhosis is more common in patients with long term alcohol consumption. Some alcoholics develop acute hepatitis as an inflammatory reaction to the cells affected by fatty change. This is not directly related to the dose of alcohol. Some people seem more prone to this reaction than others. This inflammatory reaction to the fatty change is called alcoholic steatonecrosis and the inflammation probably predisposes to liver fibrosis.

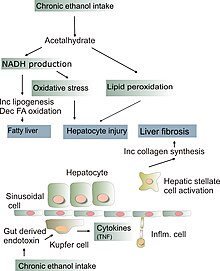
Pathophysiology
Some signs and pathological changes in liver histology include:
- Mallory's hyaline body – a condition where pre-keratin filaments accumulate in hepatocytes. This sign is not limited to alcoholic liver disease, but is often characteristic.
- Ballooning degeneration – hepatocytes in the setting of alcoholic change often swell up with excess fat, water and protein; normally these proteins are exported into the bloodstream. Accompanied with ballooning, there is necrotic damage. The swelling is capable of blocking nearby biliary ducts, leading to diffuse cholestasis.
- Inflammation – neutrophilic invasion is triggered by the necrotic changes and presence of cellular debris within the lobules. Ordinarily the amount of debris is removed by Kupffer cells, although in the setting of inflammation they become overloaded, allowing other white cells to spill into the parenchyma. These cells are particularly attracted to hepatocytes with Mallory bodies.
If chronic liver disease is also present:
- Fibrosis
- Cirrhosis – a progressive and permanent type of fibrotic degeneration of liver tissue.
 Play media
Play mediaEpidemiology
- Alcoholic hepatitis occurs in approximately 1/3 of chronic alcohol drinkers.
- 10-20% of patients with alcoholic hepatitis progress to alcoholic liver cirrhosis every year.
- Patients with liver cirrhosis develop liver cancer at a rate of 1.5% per year.
- In total, 70% of those with alcoholic hepatitis will go on to develop alcoholic liver cirrhosis in their lifetimes.
- Infection risk is elevated in patients with alcoholic hepatitis (12-26%). It increases even higher with use of corticosteroids (50%). When compared with the general population.
- Untreated alcoholic hepatitis mortality in one month of presentation may be as high as 40-50%.
Diagnosis
The diagnosis is made in a patient with history of significant alcohol intake who develops worsening liver function tests, including elevated bilirubin (typically greater than 3.0) and aminotransferases, and onset of jaundice within the last 8 weeks. The ratio of aspartate aminotransferase to alanine aminotransferase is usually 2 or more. In most cases, the liver enzymes do not exceed 500. Liver biopsy confirms the diagnosis.
Management
Clinical practice guidelines have recommended corticosteroids. People should be risk stratified using a MELD Score or Child-Pugh score. These scores are used to evaluate the severity of the liver disease based on several lab values. The greater the score, the more severe the disease.
- Abstinence: Stopping further alcohol consumption is the number one factor for recovery in patients with alcoholic hepatitis.
- Nutrition Supplementation: Protein and calorie deficiencies are seen frequently in patients suffering from alcoholic hepatitis, and it negatively affects their outcomes. Improved nutrition has been shown to improve liver function and reduce incidences encephalopathy and infections.
- Corticosteroids: These guidelines suggest that patients with a modified Maddrey's discriminant function score > 32 or hepatic encephalopathy should be considered for treatment with prednisolone 40 mg daily for four weeks followed by a taper. Models such as the Lille Model can be used to monitor for improvement or to consider alternative treatment.
- Pentoxifylline: Systematic reviews comparing the treatment of pentoxifylline with corticosteroids show there is no benefit to treatment with pentoxifylline
- Potential for combined therapy: A large prospective study of over 1000 patients investigated whether prednisolone and pentoxifylline produced benefits when used alone or in combination. Pentoxifylline did not improve survival alone or in combination. Prednisolone gave a small reduction in mortality at 28 days but this did not reach significance, and there were no improvements in outcomes at 90 days or 1 year.
- IV N-acetylcysteine: When used in conjunction with corticosteroids, improves survival at 28 days by decreasing rates of infection and hepatorenal syndrome.
- Liver Transplantation: Early liver transplantation is ideal and helps to save lives. However, patients must remain abstinent from alcohol for 6 months prior to transplantation, but the ethics and science behind this are controversial.
See also
- AST/ALT ratio
- Lille Model
- Steatohepatitis