Vaping-Associated Pulmonary Injury
Vaping-associated pulmonary injury (VAPI) also known as vaping-associated lung injury (VALI) or e-cigarette, or vaping, product use associated lung injury (E/VALI), is a lung disease associated with the use of vaping products that can be severe and life-threatening. Symptoms can initially mimic common pulmonary diagnoses like pneumonia, but individuals typically do not respond to antibiotic therapy. Individuals usually present for care within a few days to weeks of symptom onset.
Starting, in September 2019, the US Centers for Disease Control and Prevention (CDC) has been reporting on a nation-wide outbreak of severe lung disease linked to vaping, or the process of inhaling aerosolized substances with battery-operated electronic cigarettes (e-cigarettes), ciga-likes, or vape mods. The cases of lung injury date back to at least April 2019. As of February 4, 2020[update], 2,758 cases of VAPI have been reported to the CDC, with 64 confirmed deaths.
All CDC-reported cases of VAPI involve a history of using e-cigarette, or vaping, products, with most samples testing positive for tetrahydrocannabinol (THC) by the US FDA to date and most patients reporting a history of using a THC-containing product. Recent CDC data shows that the outbreak peaked in September 2019, and has declined steadily to a low level through January 2020. In late February 2020, a CDC publication in the NEJM stated that the VAPI outbreak was "driven by the use of THC-containing products from informal and illicit sources."
The CDC says that the THC cutting agent vitamin E acetate is very strongly implicated in VAPI, but evidence is not yet sufficient to rule out contribution of other chemicals of concern to VAPI as of January 2020.
Signs and symptoms
Commonly reported symptoms include shortness of breath, cough, fatigue, body aches, fever, nausea, vomiting, and diarrhea. Additional symptoms may include chest pain, abdominal pain, chills, or weight loss. Symptoms can initially mimic common pulmonary diagnoses like pneumonia, but individuals typically do not respond to antibiotic therapy. In some patients, gastrointestinal symptoms can precede respiratory symptoms. Individuals typically present for care within a few days to weeks of symptom onset. At the time of hospital presentation, the individual is often hypoxic and meets systemic inflammatory response syndrome (SIRS) criteria, including fever. Physical exam can reveal rapid heart rate or rapid breathing. Auscultation of the lungs tends to be unremarkable, even in patients with severe lung disease. In some cases, the affected individuals have progressive respiratory failure, leading to intubation. Several affected individuals have needed to be placed in the intensive care unit (ICU) and on mechanical ventilation. Time to recovery for hospital discharge has ranged from days to weeks.
Mechanism
Vaping refers to the practice of inhaling an aerosol from an electronic cigarette device, which works by heating a liquid that can contain various substances, including nicotine, tetrahydrocannabinol (THC), flavoring, and additives (e.g. glycerin (sold as vegetable glycerine (VG)), propylene glycol (PG)). The long-term health impacts of vaping are unknown. Glycerin was long thought to be a safe option. However, the carcinogen formaldehyde is known as a product of propylene glycol and glycerol vapor degradation, these ingredients may also cause lung inflammation.
Most individuals treated for VAPI report vaping the cannabis compounds THC and/or cannabidiol (CBD), and some also report vaping nicotine products. In addition to vaping, some individuals have also experienced VAPI through "dabbing." Dabbing uses a different type of device to heat and extract cannabinoids for inhalation. It is a process that entails superheating and inhaling particles into the lungs that contain THC and other types of cannabidiol plant materials.
VAPI appears to be a type of acute lung injury, similar to acute fibrinous pneumonitis, organizing pneumonia, or diffuse alveolar damage. VAPI appears to be a general term for various causes of acute lung damage due to vaping. There is no evidence of an infectious etiology causing VAPI.
No single compound or ingredient has emerged as the cause of these illnesses as of November 2019[update]. Many different substances and product sources are still under investigation. The CDC stated that the latest national and state findings suggest products containing THC, particularly from informal sources like friends, family, or in-person or online dealers, are linked to most of the cases and play a major role in the outbreak. The CDC states that vitamin E acetate is a very strong culprit of concern in VAPI, having been found in 29 out of 29 lung biopsies tested from ten different states, but evidence is not yet sufficient to rule out contribution of other chemicals of concern to VAPI. The CDC states that previous research suggests inhaled vitamin E acetate may interfere with normal lung functioning. A 2020 study found that vaped vitamin E acetate produced exceptionally toxic ketene gas, and carcinogic alkenes and benzene.
Diagnosis
High clinical suspicion is necessary to make the diagnosis of VAPI. As of October 2019, VAPI is considered a diagnosis of exclusion because no specific tests or markers exist for its diagnosis, as of October 2019. Healthcare providers should evaluate for alternative diagnoses (e.g., cardiac, gastrointestinal, rheumatologic, neoplastic, environmental, or occupational exposures, or causes of acute respiratory distress syndrome) as suggested by clinical presentation and medical history, while also considering multiple etiologies, including the possibility of VAPI occurring with a concomitant infection.
All healthcare providers evaluating patients for VAPI should consider obtaining a thorough patient history, including symptoms and recent use of e-cigarette, or vaping, products, along with substances used, duration and frequency of use, and method of use. Additionally a detailed physical examination should be performed, specifically including vital signs and pulse-oximetry. Laboratory testing guided by clinical findings, which may include a respiratory virus panel to rule out infectious diseases, complete blood count with differential, serum inflammatory markers (C-reactive protein [CRP], erythrocyte sedimentation rate [ESR]), liver transaminases, and urine toxicology testing, including testing for THC should be acquired. Imaging, typically a chest X-ray, with consideration for a chest CT if chest X-ray results do not correlate with the clinical picture or to evaluate severe or worsening disease should be obtained. Consulting with specialists (e.g. critical care, pulmonology, medical toxicology, or infectious disease) can help guide further evaluation. The diagnosis is commonly suspected when the person does not respond to antibiotic therapy, and testing does not reveal an alternative diagnosis. Many of the reported cases involved worsening respiratory failure within 48 hours of admission after the administration of empiric antibiotic therapy. Lung biopsies are not necessary for the diagnosis but are performed as clinically indicated to rule out the likelihood of infection.
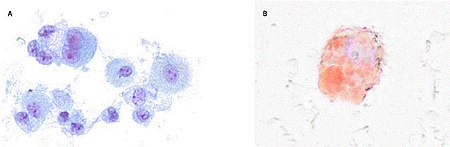
There are non-specific laboratory abnormalities that have been reported in association with the disease, including elevations in white blood cell count (with neutrophilic predominance and absence of eosinophilia), transaminases, procalcitonin, and inflammatory markers. Infectious disease testing, including blood and sputum cultures and tests for influenza, Mycoplasma, and Legionella were all found to be negative in the majority of reported cases. Imaging abnormalities are typically bilateral and are usually described as "pulmonary infiltrates or opacities" on chest X-ray and "ground-glass opacities" on chest CT. Bronchoalveolar lavage specimens may exhibit an increased level of neutrophils in combination with lymphocytes and vacuole-laden macrophages. Lavage cytology with oil red O staining demonstrated extensive lipid-laden alveolar macrophages. In the few cases in which lung biopsies were performed, the results were consistent with acute lung injury and included a broad range of features, such as acute fibrinous pneumonitis, diffuse alveolar damage, lipid-laden macrophages, and organizing pneumonia. Lung biopsies often showed neutrophil predominance as well, with rare eosinophils.
Case definitions
Based on the clinical characteristics of VAPI cases from ongoing federal and state investigations, interim surveillance case definitions for confirmed and probable cases have been developed.
The CDC surveillance case definition for confirmed cases of severe pulmonary disease associated with e-cigarette use:
- Using an e-cigarette ("vaping") or dabbing during the 90 days before symptom onset AND
- Pulmonary infiltrate, such as opacities on plain film chest radiograph or ground-glass opacities on chest computed tomography AND
- Absence of pulmonary infection on initial work-up. Minimum criteria include:
- A negative respiratory viral panel
- A negative influenza polymerase chain reaction or rapid test if local epidemiology supports testing.
- All other clinically indicated respiratory infectious disease testing (e.g., urine antigen for Streptococcus pneumoniae and Legionella, sputum culture if productive cough, bronchoalveolar lavage culture if done, blood culture, human immunodeficiency virus–related opportunistic respiratory infections if appropriate) must be negative and
- No evidence in medical record of alternative plausible diagnoses (e.g., cardiac, rheumatologic, or neoplastic process).
The CDC surveillance case definition for probable cases of severe pulmonary disease associated with e-cigarette use:
- Using an e-cigarette ("vaping") or dabbing in 90 days before symptom onset AND
- Pulmonary infiltrate, such as opacities on plain film chest radiograph or ground-glass opacities on chest computed tomography AND
- Infection identified via culture or polymerase chain reaction, but clinical team believes this is not the sole cause of the underlying respiratory disease process OR minimum criteria to rule out pulmonary infection not met (testing not performed) and clinical team believes this is not the sole cause of the underlying respiratory disease process and
- No evidence in medical record of alternative plausible diagnoses (e.g., cardiac, rheumatologic, or neoplastic process).
These surveillance case definitions are meant for public health data collection purposes and are not intended to be used as a clinical diagnostic tool or to guide clinical care; they are subject to change and will be updated as additional information becomes available.
Differential diagnosis
As VAPI is, as of October 2019, a diagnosis of exclusion, a variety of respiratory diseases must be ruled out before a diagnosis of VAPI can be made. The differential diagnosis should include more common diagnostic possibilities, such as community-acquired pneumonia, as well as do-not-miss diagnoses, such as pulmonary embolism. Other commonly documented hospital diagnoses for cases of severe pulmonary disease associated with e-cigarette use have included acute respiratory distress syndrome (ARDS), sepsis, acute hypoxic respiratory failure, and pneumonitis. As of September 2019, distinctions are still being made between processes occurring in association with vaping or the use of nicotine-containing liquids and those considered as alternative diagnoses to VAPI. These processes include the following:
- Acute eosinophilic pneumonia
- Hypersensitivity pneumonitis
- Respiratory bronchiolitis interstitial lung disease
- Organizing pneumonia
- Lipoid pneumonia
- Diffuse alveolar hemorrhage
- Giant cell pneumonitis
The use of imaging and other diagnostic modalities, including chest CT, bronchoscopy with bronchoalveolar lavage, and lung biopsy, may provide additional information to determine the presence of these processes and potentially establish a definitive diagnosis, but are generally not performed unless clinically indicated.
Treatment
CDC recommendations for primary care
As of October 18, 2019[update], the CDC has published updated interim guidance based on the most current data to provide a framework for healthcare providers in their management and follow-up of persons with symptoms of VAPI. Initial management involves deciding whether to admit a patient with possible VAPI to the hospital. Currently, the CDC recommends that patients with suspected VAPI should be admitted if they have decreased O2 saturation (<95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. Once admitted, initiation of corticosteroids should be considered, which have been found to be helpful in treating this injury. Several case reports describe improvement with corticosteroids, likely because of a blunting of the inflammatory response. In a group of patients in Illinois and Wisconsin, 92% of 50 patients received corticosteroids, and those that began glucocorticoid therapy continued on it for at least 7 days. The medical team documented in 65% of 46 patient notes that "respiratory improvement was due to the use of glucocorticoids". Among 140 cases reported nationally to the CDC that received corticosteroids, 82% of patients improved. In patients with more severe illness, a more aggressive empiric therapy with corticosteroids as well as antimicrobial and antiviral therapy may be warranted.
As a large proportion of patients were admitted to an intensive care unit based on data submitted to the CDC, many patients require supplemental oxygen via nasal cannula, high-flow oxygen, bilevel positive airway pressure (BiPAP), or mechanical ventilation.
During influenza season, health care providers should consider influenza in all patients with suspected VAPI. Decisions on initiation or discontinuation of treatment should be based on specific clinical features and, when appropriate, in consultation with specialists.
Special consideration should be given to high-risk patients such as the elderly, those with a history of cardiac or lung disease, or pregnant individuals. Patients over 50 years old have an increased risk of intubation and might need longer hospitalizations. CDC says patients should be advised to discontinue the use of vaping products upon hospital admission and during outpatient follow-up, to speed recovery and avoid potential recurrence of symptoms or lung injury. Evidence-based tobacco product quitting strategies include behavioral counseling and U.S. Food and Drug Administration (US FDA)-approved cessation medications.
Follow-up care
Due to reports of relapse during corticosteroid tapers after hospitalization, the CDC recommends scheduling a follow-up visit no later than one to two weeks after discharge from inpatient hospital treatment from VAPI, with considerations for performing pulse-oximetry testing and repeat CXR. In one to two months, healthcare providers should consider additional follow-up testing, including spirometry, diffusion capacity testing, and another repeat CXR. In patients with persistent hypoxemia (O2 saturation <95%) requiring home oxygen at discharge, consider ongoing pulmonary follow-up. In patients treated with high-dose corticosteroids, consider endocrinology follow-up to monitor adrenal function.
As it is unknown whether patients with a history of VAPI are at increased risk for severe complications with influenza or other respiratory infections, follow-up care should also include annual vaccination against influenza for all persons over 6 months of age, including patients with a history of EVALI, as well as administration of the pneumococcal vaccine according to current guidelines.
An important part of both inpatient and follow-up care for VAPI involves advising patients to discontinue use of e-cigarette or vaping products.
Public health recommendations
The CDC and the FDA recommend that people not use e-cigarettes or other vaping products that contain THC, particularly products purchased off the street or obtained from informal sources like friends, family, or online sellers. In addition, CDC recommends that individuals not modify or add any substances to e-cigarettes or other vaping products that are not intended by the manufacturer.
Avoiding e-cigarettes entirely avoids the risk of VAPI as well as other negative health consequences of vaping, but some health advocates promote e-cigarettes for certain populations as a means to help smokers of conventional cigarettes to quit. Research into the effectiveness of this approach is still incomplete.
Epidemiology
An outbreak of vaping-related lung injuries in 2019 and 2020 has mainly affected young people, primarily in the United States. As of February 4, 2020[update], there have been 2,758 cases of VAPI reported from all 50 states, the District of Columbia, Puerto Rico, and the US Virgin Islands. The CDC has received complete gender and age data on these cases with 70% of cases being male. The median age of cases is 24 years and ranges from 13 to 85 years. 79% of cases are under 35 years old. There have been 64 confirmed deaths in 28 states and the District of Columbia from this outbreak ranging from ages 15–75 years old.
Of the 2,051 cases reported to the CDC, information on substance use is known for 867 cases in the three months prior to symptom onset as of October 15, 2019. About 86% reported using THC-containing products; 34% reported exclusive use of THC-containing products. About 64% reported using nicotine-containing products; 11% reported exclusive use of nicotine-containing products.
On September 28, 2019, the first case of vaping-associated pulmonary injury was identified in Canada. A number of other probable cases have been reported in British Columbia and New Brunswick as of October 2019.
In September 2019, a US Insurance Journal article stated that at least 15 incidents of vaping related illnesses have been reported worldwide prior to 2019, occurring from Guam to Japan to the UK to the US. 12 cases of health problems with nicotine-containing e-cigarettes were reported to the UK's Medicines and Healthcare products Regulatory Agency (MHRA), with at least one case bearing high similarities to the lipid pneumonia cases reported in the US. One lipoid pneumonia-related death in the UK was associated with e-cigarettes in 2010.
Medical officials in continental Europe have not reported any serious medical problems related to vaping products except one early case related to e-cigarettes documented in Northern Spain in 2015. Since many of the cases in North America were traced to THC-cartridges as well as the use of e-cigarette vape products, but THC remains illegal in European countries, the disease burden related to vaping has been significantly lower in Europe despite the prevalence of e-cigarette use.
Before the outbreak, one lipoid pneumonia-related death in the UK was associated with e-cigarettes in 2010.
18 year-old Raphaël Pauwaert from Brussels died on November 6, 2019, after developing pneumonia and being placed in a medically induced coma because he was unable to breathe on his own. He received an e-cigarette as a gift for his 18th birthday. His doctor stated Pauwaert's fatal lung infection probably resulted from the CBD vapor. This was considered the first death tied to vaping in Belgium. Pauwaert's CBD oils he also used were tested for vitamin E at the Saint-Luc Hospital in November 2019. The death is under investigation by the Brussels Public Prosecutor's Office. A friend of Pauwaert's was also hospitalized with the identical symptoms after using the same type of e-cigarette, but he survived.
The first case of a vaping-related lung illness in the Philippines was reported in November 2019. A 16-year-old girl from central Philippines was vaping e-cigarettes for half a year. She had difficulty breathing and was admitted to the hospital in October 2019. She was discharged after she received treatment from a pediatric pulmonologist.
Footnotes
- ^ a b c d e f
Vaping-associated pulmonary injury (VAPI) is also variously known as
- e-cigarette, or vaping, product use associated lung injury (E/VALI),
- vaping-associated lung injury,
- vaping-associated lung disease,
- vaping-induced lung injury,
- vaping-induced pulmonary disease,
- vaping associated respiratory syndrome,
- vape-related lung disease,
- vape-related lung illness,
- vape-related pulmonary illness,
- vaporizer-linked respiratory failure,
- vaping-linked lung illness,
- vape lung