-
Rohhad
Wikipedia
Patients present with both alveolar hypoventilation along with hypothalamic dysfunction, which distinguishes ROHHAD from congenital central hypoventilation syndrome (CCHS). [2] ROHHAD is a rare disease, with only 100 reported cases worldwide thus far. [3] The first sign of ROHHAD is a rapid weight gain between 1.5 and 11 years of age. [4] Typically, hypoventilation, or abnormally slow breathing, presents after the rapid onset obesity. [4] Symptoms of hypothalamic dysfunction and autonomic dysfunction present in a variety of ways, but in order for a diagnosis of ROHHAD they must be present in some form. [3] Approximately 40% of patients will develop neuroendocrine tumors. [1] There is also a possibility of behavioral disorders, but some children with ROHHAD have normal cognitive development and intelligence. [3] Treatment plans for ROHHAD vary depending on each patient's symptoms. ... The later ROHHAD is diagnosed, the greater the risk for behavioral problems due to hypoxia from hypoventilation or during cardiopulmonary arrest. [3] Cause [ edit ] The etiology of ROHHAD is currently unknown, and the condition is diagnosed based on a set of clinical criteria. [1] It is believed that there may be a genetic component to ROHHAD, however there is no widely accepted gene linked to the disease. [3] There has been one ROHHAD patient identified to have a mutation in the retinoic acid-induced 1(RAI1) gene through Whole Exome Sequencing, but there has been no otherwise proven link between the RAI1 gene and ROHHAD. [17] It is believed that ROHHAD originates from a combination of genetic and environmental or immunological factors. [1] As of yet, evidence of its etiology has not been discovered and is not well understood. [1] In 2011, a case of monozygotic twins with divergent ROHHAD phenotypes was reported. ... This report questioned the theory that ROHHAD is genetically inherited, and the authors suggest that the disease may have an autoimmune or epigenetic etiology. [18] Pathophysiology [ edit ] The pathophysiology of ROHHAD is not currently known or understood. [1] Diagnosis [ edit ] Rapid obesity is the first symptom to arise between the ages of 1.5 and 11. ... Lurie Children's Hospital of Chicago has an international repository for patients with ROHHAD, which is available to researchers who are interested in the disease. [25] As of June 2018, there are 3 clinical trials currently recruiting patients with ROHHAD being performed respectively at Lurie Children's Hospital, Sidney Kimmel Cancer Center , and Boston Children's Hospital . [26] Epidemiology [ edit ] There have been at least 158 documented cases of ROHHAD worldwide. [27] History [ edit ] ROHHAD was first described in 1965, and this was believed to be the first reported instance of hypoventilation presenting alongside hypothalamic dysfunction. [2] ROHHAD had often been mistaken for congenital central hypoventilation syndrome, until the distinction was made by Ize-Ludlow et al. in 2007. ... Retrieved 2018-06-03 . ^ Thaker, Vidhu V.; Esteves, Kristyn M.; Towne, Meghan C.; Brownstein, Catherine A.; James, Philip M.; Crowley, Laura; Hirschhorn, Joel N.; Elsea, Sarah H.; Beggs, Alan H. (May 2015). "Whole exome sequencing identifies RAI1 mutation in a morbidly obese child diagnosed with ROHHAD syndrome" .

-
Intellectual Developmental Disorder 59
Omim
A number sign (#) is used with this entry because of evidence that autosomal dominant intellectual developmental disorder-59 (MRD59) is caused by heterozygous mutation in the CAMK2G gene (602123) on chromosome 10q22. ... Detailed in vitro and in vivo functional studies in mouse primary hippocampal cells and in mouse embryos showed that the mutant protein caused decreased neurite length and arborization, as well as impaired neuronal migration from the subventricular zone during development. A dominant effect was observed. Further studies showed that the mutant protein had constitutively increased phosphotransferase activity with increased autophosphorylation at Thr287 compared to controls, consistent with a gain of function. ... The authors concluded that CAMK2G has an indispensable function in neurodevelopment and that the R292P protein gains constitutive activity toward cytosolic targets, rather than impaired targeting to the nucleus. INHERITANCE - Autosomal dominant GROWTH Height - Short stature, mild HEAD & NECK Head - Large head circumference Face - Dysmorphic facial features, mild, variable - Tall forehead - Narrow forehead - Flat forehead - Flat face - Round cheeks - Long philtrum - Facial hypotonia Ears - Prominent ears - Low-set ears Eyes - Myopia - Long palpebral fissures - Arched eyebrows - Glaucoma, juvenile Nose - Tubular nose - Full nasal tip SKELETAL Hands - Short hands - Brachydactyly Feet - Short feet - Large first toes SKIN, NAILS, & HAIR Skin - Vascular malformations (1 patient) Nails - Brittle nails (1 patient) MUSCLE, SOFT TISSUES - Hypotonia NEUROLOGIC Central Nervous System - Global developmental delay - Impaired intellectual development - Impaired language development - No seizures Behavioral Psychiatric Manifestations - Autistic features MISCELLANEOUS - Two unrelated patients have been reported (last curated July 2019) - Non-neurologic features are variable - De novo mutation MOLECULAR BASIS - Caused by mutation in the calcium/calmodulin-dependent protein kinase II-gamma gene (CAMK2G, 602123.0001 ) ▲ Close
-
Spondyloepimetaphyseal Dysplasia, Strudwick Type
Wikipedia
Find sources: "Spondyloepimetaphyseal dysplasia, Strudwick type" – news · newspapers · books · scholar · JSTOR ( June 2020 ) ( Learn how and when to remove this template message ) Spondyloepimetaphyseal dysplasia, Strudwick type Other names Lower extremity-predominant autosomal dominant proximal spinal muscular atrophy Spondyloepimetaphyseal dysplasia, Strudwick type is inherited in an autosomal dominant pattern. ... The name of the condition indicates that it affects the bones of the spine (spondylo-) and two regions near the ends of bones ( epiphyses and metaphyses ). This type was named after the first reported patient with the disorder. ... This condition is inherited in an autosomal dominant pattern, which means one copy of the altered gene is sufficient to cause the disorder.COL2A1, FN1, PCYT1A, ACP5, CFAP410, TRPV4, PAM16, TRIP11, EFL1, GPX4, COL10A1, LBR, TONSL, MAPT, TARDBP, ABCB10P1, MMP13

-
Rapp–hodgkin Syndrome
Wikipedia
Rapp–Hodgkin syndrome Other names Ectodermal dysplasia, anhidrotic, with cleft lip/palate [1] Rapp–Hodgkin syndrome was formerly thought to be a unique autosomal dominant disorder due to a P63 gene mutation. However, it was recently shown to the same disease as Hay–Wells syndrome . [2] It was first characterized in 1968. [3] Contents 1 See also 2 References 3 Further reading 4 External links See also [ edit ] Punctate porokeratosis List of cutaneous conditions References [ edit ] ^ "Rapp–Hodgkin syndrome" . ... "Anhidrotic ectodermal dysplasia: autosomal dominant inheritance with palate and lip anomalies" . ... Includes: Rapp–Hodgkin Syndrome External links [ edit ] Classification D OMIM : 129400 MeSH : C535289 External resources Orphanet : 3022 OMIM entries on AEC v t e Genetic disorders relating to deficiencies of transcription factor or coregulators (1) Basic domains 1.2 Feingold syndrome Saethre–Chotzen syndrome 1.3 Tietz syndrome (2) Zinc finger DNA-binding domains 2.1 ( Intracellular receptor ): Thyroid hormone resistance Androgen insensitivity syndrome PAIS MAIS CAIS Kennedy's disease PHA1AD pseudohypoaldosteronism Estrogen insensitivity syndrome X-linked adrenal hypoplasia congenita MODY 1 Familial partial lipodystrophy 3 SF1 XY gonadal dysgenesis 2.2 Barakat syndrome Tricho–rhino–phalangeal syndrome 2.3 Greig cephalopolysyndactyly syndrome / Pallister–Hall syndrome Denys–Drash syndrome Duane-radial ray syndrome MODY 7 MRX 89 Townes–Brocks syndrome Acrocallosal syndrome Myotonic dystrophy 2 2.5 Autoimmune polyendocrine syndrome type 1 (3) Helix-turn-helix domains 3.1 ARX Ohtahara syndrome Lissencephaly X2 MNX1 Currarino syndrome HOXD13 SPD1 synpolydactyly PDX1 MODY 4 LMX1B Nail–patella syndrome MSX1 Tooth and nail syndrome OFC5 PITX2 Axenfeld syndrome 1 POU4F3 DFNA15 POU3F4 DFNX2 ZEB1 Posterior polymorphous corneal dystrophy Fuchs' dystrophy 3 ZEB2 Mowat–Wilson syndrome 3.2 PAX2 Papillorenal syndrome PAX3 Waardenburg syndrome 1&3 PAX4 MODY 9 PAX6 Gillespie syndrome Coloboma of optic nerve PAX8 Congenital hypothyroidism 2 PAX9 STHAG3 3.3 FOXC1 Axenfeld syndrome 3 Iridogoniodysgenesis, dominant type FOXC2 Lymphedema–distichiasis syndrome FOXE1 Bamforth–Lazarus syndrome FOXE3 Anterior segment mesenchymal dysgenesis FOXF1 ACD/MPV FOXI1 Enlarged vestibular aqueduct FOXL2 Premature ovarian failure 3 FOXP3 IPEX 3.5 IRF6 Van der Woude syndrome Popliteal pterygium syndrome (4) β-Scaffold factors with minor groove contacts 4.2 Hyperimmunoglobulin E syndrome 4.3 Holt–Oram syndrome Li–Fraumeni syndrome Ulnar–mammary syndrome 4.7 Campomelic dysplasia MODY 3 MODY 5 SF1 SRY XY gonadal dysgenesis Premature ovarian failure 7 SOX10 Waardenburg syndrome 4c Yemenite deaf-blind hypopigmentation syndrome 4.11 Cleidocranial dysostosis (0) Other transcription factors 0.6 Kabuki syndrome Ungrouped TCF4 Pitt–Hopkins syndrome ZFP57 TNDM1 TP63 Rapp–Hodgkin syndrome / Hay–Wells syndrome / Ectrodactyly–ectodermal dysplasia–cleft syndrome 3 / Limb–mammary syndrome / OFC8 Transcription coregulators Coactivator: CREBBP Rubinstein–Taybi syndrome Corepressor: HR ( Atrichia with papular lesions ) This Genodermatoses article is a stub .
-
Juvenile Amyotrophic Lateral Sclerosis
Gard
Mutations may be inherited from a parent or may occur for the first time in a person with the disease. Inheritance may be autosomal recessive or autosomal dominant depending on the gene involved.
-
Cafe-Au-Lait Spots, Multiple
Omim
Charrow et al. (1993) reported a family with multiple cafe-au-lait spots with no other features of NF1 in 4 generations, with male-to-male transmission in the first 2 generations. Mapping Charrow et al. (1993) excluded linkage to NF1 on chromosome 17 in a family with multiple cafe-au-lait spots. ... Eyes - No Lisch nodules of the iris Inheritance - Autosomal dominant Skin - Multiple cafe-au-lait spots - No neurofibromas ▲ CloseMAP2K2, AKT1, MAN1B1, TSC1, TSC2, XRCC2, KDM5C, TP63, BUB3, TRIP13, CEP57, ABCB6, MAD2L2, SEC23B, CIB1, TMC6, SDHC, PLXND1, UBE2T, SMARCAL1, FANCL, RFWD3, FANCI, FANCM, PALB2, BRIP1, SLX4, TWIST2, TMC8, ARL6IP6, SDHD, SDHB, ATM, FANCG, BRCA1, BRAF, BRCA2, BUB1, BUB1B, ERCC4, FANCA, FANCC, FANCD2, FANCE, FANCB, FANCF, GNAS, REV3L, IL7, KRAS, NF1, NF2, PCNT, PIK3CA, MAP2K1, PTEN, RAD51, RAD51C, KLLN, MRC1, MSH2
-
Arrhythmogenic Right Ventricular Dysplasia, Familial, 6
Omim
The family spanned 5 generations, having 10 living and 2 dead affected individuals, with ARVD segregating as an autosomal dominant. Mapping By linkage analysis in a North American family with early-onset arrhythmogenic right ventricular dysplasia, Li et al. (2000) first excluded the 5 previously known ARVD loci, and a novel locus was identified on 10p14-p12.
-
Neutrophil Migration
Omim
Jacobs and Norman (1977) found a cellular chemotactic defect in the neutrophils of both parents and 3 of 4 children who suffered from unusually severe bacterial eczema, asthma and recurrent bacterial skin infections, all starting in the first month of life. All affected members had HLA-B12; the normal child did not. ... Immune - Immunodeficiency Inheritance - Autosomal dominant Skin - Congenital ichthyosis ▲ Close
-
Edema, Familial Idiopathic, Prepubertal
Omim
Intermittent swelling of the face and abdomen was noted as early as the first year of life. Children with later onset often had swelling beginning after a period of weight gain. GU - Frequent micturition - Poor bladder control Neuro - Affective disturbance - Irritability - Lability of mood - Lassitude - Functional autonomic symptoms Inheritance - Autosomal dominant Endocrine - Diabetes mellitus Misc - Onset neonatal to age 12 years Skin - Idiopathic edema GI - Vomiting, often projectile ▲ Close
-
Congenital Hereditary Endothelial Dystrophy Type I
Orphanet
Clinical description Lesions become manifest in the first two years of life with photophobia and tearing. ... Genetic counseling Transmission appears to be autosomal dominant. Management and treatment Patients with CHED I usually require a penetrating keratoplasty, because procedures for repairing the posterior surface of the cornea, such as a deep lamellar endothelial keratoplasty (DLEK), Descemet stripping endothelial keratoplasty (DSEK), or Descemet stripping automated endothelial keratoplasty (DSAEK) and technically difficult in young children.
-
Lachiewicz–sibley Syndrome
Wikipedia
Lachiewicz–Sibley syndrome is a rare autosomal dominant disorder characterized by preauricular pits and renal disease. Persons with this disease may have hypoplasic kidneys or proteinuria . This disease was first described in a Caucasian family of British and Irish descent that emigrated to Ohio in the 19th century before settling in Nebraska.
-
Dentinogenesis Imperfecta
Gard
Dentinogenesis imperfecta is caused by mutations in the DSPP gene and is inherited in an autosomal dominant manner. According to the original classification, there are three types of dentinogenesis imperfecta: Type I: occurs in people who have osteogenesis imperfecta , a genetic condition in which bones are brittle, causing them to break easily. ... Type III: usually occurs in people without another inherited disorder. Type III was first identified in a group of families in southern Maryland and has also been seen in individuals of Ashkenazi Jewish descent.
-
Thiel-Behnke Corneal Dystrophy
Orphanet
Clinical description Corneal erosions develop in the first and second decade of life and cause ocular discomfort and pain. ... Genetic counseling This entity has an autosomal dominant mode of inheritance. Management and treatment The pathologic corneal tissue can be excised surgically or with an eximer laser.
-
Wilson-Turner Syndrome
Orphanet
The syndrome has been described in two families to date: 14 males in the 3 most recent generations of the first family, and 7 males and 7 females in a 5-generation Dutch family. ... Genetic counseling X-linked recessive transmission and X-linked dominant inheritance with absence of male-to-male transmission have been reported.
-
Metachromatic Leukodystrophy, Adult-Onset, With Normal Arylsulfatase A
Omim
All affected individuals had an affected parent except for the affected male in the first generation, and information concerning his parents is lacking. Endocrine - Disabling hypotension GU - Urinary urgency - Incontinence Neuro - Adult-onset metachromatic leukodystrophy variant - Autonomic neuropathy Lab - Normal arylsulfatase A levels - Excess sulfatides in brain white matter - Normal adrenals Inheritance - Autosomal dominant ▲ Close
-
Meningococcal Disease
Wikipedia
Meningococcemia [ edit ] Symptoms of meningococcemia are, at least initially, similar to those of influenza . Typically, the first symptoms include fever, nausea , myalgia, headache, arthralgia , chills , diarrhea, stiff neck, and malaise. ... Vaccines are currently available against all six strains, including the newest vaccine against serogroup B. The first vaccine to prevent meningococcal serogroup B (meningitis B) disease was approved by the European Commission on 22 January 2013. ... IRIN Africa news has been providing the number of deaths for each country since 1995, [43] [44] [45] [46] and a mass vaccination campaign following a community outbreak of meningococcal disease in Florida was done by the CDC . [47] History and etymology [ edit ] From the Greek meninx (membrane) + kokkos (berry), meningococcal disease was first described by Gaspard Vieusseux during an outbreak in Geneva in 1805. ... "Novartis receives EU approval for Bexsero, first vaccine to prevent the leading cause of life-threatening meningitis across Europe" . ... I61 ^ Tasker SA, Treanor J, Rossetti R et al. Whole virion influenza vaccine has protective efficacy in the setting of HIV infection.CFHR3, CFH, ACE, CFD, ADAM32, FBXO15, CNTNAP5, ZMIZ1, GRM5, PRDM11, OLA1, ALCAM, NUP62, MYO16, TMPRSS15, IL4I1, CES1, SERPINE1, MBL2, TLR4, TNF, IL10, ST11, IL1A, C7, IL1RN, TLR2, IL1B, CD46, FCGR2C, CFP, ABO, SFTPA2, IL4, FCGR2A, FCGR2B, CPB2, DHPS, DEFA4, C5AR2, BPIFA1, TLR9, ENAH, AP2M1, CD14, SERPING1, C11orf40, CEACAM1, CFB, ADRB1, SFTPA1, DEFB1, CXCL10, EGFR, F3, GAPDH, SLC11A1, SFTPD, CXCL11, RELA, CFHR1, PLG, IGHA1, PC, IL1R1, NMB, MIF, ADD1, ALKBH1

-
Optic Neuritis
Wikipedia
Please help improve it or discuss these issues on the talk page . ( Learn how and when to remove these template messages ) This article may need to be rewritten to comply with Wikipedia's quality standards . You can help . The talk page may contain suggestions. ( March 2016 ) This article needs additional citations for verification . ... Unique characteristics of optical coherence tomography (OCT) results and visual acuity testing in myelin oligodendrocyte glycoprotein (MOG) antibody positive pediatric patients, Nov. 2018, MS and related disorders, Volume 28, February 2019, Pages 86-90, doi: https://doi.org/10.1016/j.msard.2018.11.026 ^ Beck RW, Cleary PA, Trobe JD, Kaufman DI, Kupersmith MJ, Paty DW, Brown CH (1993).MOG, CAPN1, AQP4, TK2, POLG, PLXNA2, TNF, CSF2, LAMC2, HLA-DRB1, ASCC2, PMEL, MBP, SART3, IL10, IL4, IFNG, HLA-DRB5, CD19, HLA-DQB1, CAT, TPX2, HCRT, SND1, NFKB2, OAS3, CUX1, HT, SDC1, REN, STAT1, OPN1LW, TG, IL27, PRKCD, CXCL13, TPO, PHLDA2, PLA2G6, RBM45, RTN4R, MLC1, POU2F3, RASL12, RASD1, IL17D, LINGO1, DPYSL5, APOE, MS, PLA2G2A, HLA-A, AVPR2, BDNF, CD14, CD27, CISH, CCR5, CNR1, EDN1, GABPA, GFAP, GSTM1, GSTT1, HLA-DQA1, PLA2G1B, IL17A, ITGB3, MAG, MAP3K5, MIF, MMP2, MMP9, FAS, NEFH, NEFL, NFE2L2, CLDN11, MARCHF11
-
Emotional Dysregulation
Wikipedia
Affect dysregulation and disorders of the self . New York: Norton. [ page needed ] ^ Bjorkquist, Olivia (2010). ... Practitioner's Guide to Emotion regulation in School – Aged Children. NY: Springer. [ page needed ] ^ Waller E, Scheidt CE (February 2006). ... Self-regulation in early childhood. New York: Guilford Press. [ page needed ] ^ Vilhena-Churchill N, Goldstein AL (May 2014).
-
Conduction Aphasia
Wikipedia
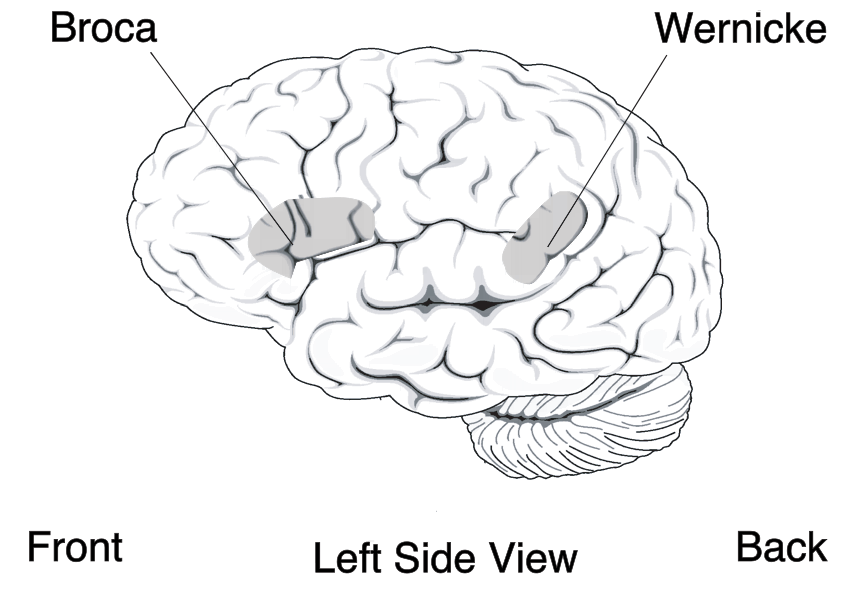
Causes [ edit ] Conduction aphasia is caused by damage to the parietal lobe of the brain, especially in regards to the area associated with the left-hemisphere dominant dorsal stream network. [17] [10] The arcuate fasciculus, which connects Broca's area and Wernicke's area (important for speech and language production and comprehension, respectively), is affected. [17] These two areas control speech and language in the brain. ... This can be done through a CT or MRI or the brain; these are the first imaging modality of choice. [16] Treatment [ edit ] Speech and language therapy are typically used as a treatment. ... Wernicke predicted the existence of conduction aphasia in his landmark 1874 monograph, Der Aphasische Symptomenkompleks: Eine Psychologische Studie auf Anatomischer Basis . [3] [19] [22] He was the first to distinguish the various aphasias in an anatomical framework, and proposed that a disconnection between the two speech systems (motor and sensory) would lead to a unique condition, distinct from both expressive and receptive aphasias, which he termed Leitungsaphasie . ... Introduction to Neurogenic Communication Disorders . Jones & Bartlett Learning. [ page needed ] ^ Ardila, Alfredo (2010). ... "The rate and extent of improvement with therapy from the different types of aphasia in the first year after stroke". Clinical Rehabilitation . 21 (10): 941–9. doi : 10.1177/0269215507078452 .
-
Supracondylar Humerus Fracture
Wikipedia
The capitulum of the humerus is the first to ossify at the age of one year. Head of radius and medial epicondyle of the humerus starts to ossify at 4 to 5 years of age, followed by trochlea of humerus and olecranon of the ulna at 8 to 9 years of age, and lateral epicondyle of the humerus to ossify at 10 years of age. [2] Anterior X-ray [ edit ] Baumann's Angle Carrying angle can be evaluated through AP view of the elbow by looking at the Baumann’s angle. [2] There are two definitions of Bowmann's angle: The first definition of Baumann's angle is an angle between a line parallel to the longitudinal axis of the humeral shaft and a line drawn along the lateral epicondyle. ... Open/closed reduction with percutaneous pinning would the first line of management. However, if there is no improvement of pulse after the reduction, surgical exploration of brachial artery and nerves is indicated, especially when there is persistent pain at the fracture site (indicating limb ischaemia), neurological deficits ( paresthesia , tingling, numbness), and additional signs of poor perfusion (prolonged capillary refilling time, and bluish discolouration of the fingers). [2] Meanwhile, for pink, pulseless hand (absent radial pulse but with good perfusion at extremities) after successful reduction and percutaneous pinning, the patient could still be observed until additional signs of ischaemia develops which warrants a surgical exploration. [9] Isolated neurological deficits occurred in 10 to 20% of the cases and can reach as high as 49% in Type III Gartland fractures. ... The mechanism of injury is most commonly due to fall on an outstretch hand. [2] Extension type of injury (70% of all elbow fractures) is more common than the flexion type of injury (1% to 11% of all elbow injuries). [3] Injury often occurs on the non-dominant part of the limb. Flexion type of injury is more commonly found in older children. ... Al Ameen Journal of Medical Sciences . 10 (1): 64–70 . Retrieved 15 April 2018 . ^ a b Page 1405 in: S. Terry Canale, James H.





