Herb-drug interactions [ edit ] Herb-drug interactions are drug interactions that occur between herbal medicines and conventional drugs. [24] These types of interactions may be more common than drug-drug interactions because herbal medicines often contain multiple pharmacologically active ingredients, while conventional drugs typically contain only one. [24] Some such interactions are clinically significant , [25] although most herbal remedies are not associated with drug interactions causing serious consequences. [26] Most herb-drug interactions are moderate in severity. [27] The most commonly implicated conventional drugs in herb-drug interactions are warfarin , insulin , aspirin , digoxin , and ticlopidine , due to their narrow therapeutic indices . [27] [28] The most commonly implicated herbs involved in such interactions are those containing St. ... Revista Mexicana de Anestesiología . 28 (1): 32–42. Archived from the original on 2012-06-29. ^ J.
Relapsing polychondritis (RP) is characterized by recurrent swelling and inflammation of cartilage and other tissues throughout the body. Cartilage is a tough but flexible tissue that covers the ends of bones at a joint and gives shape and support to other parts of the body. Symptoms of RP include swelling of the cartilage of the ear, nose, and joints. Other parts of the body that may be involved are the airways (trachea), costal (rib) cartilage, eyes, heart, vascular (veins) system, skin, kidney, and nervous system. The signs and symptoms vary from person to person depending on which parts of the body are affected.
A rare, clinically heterogeneous, multisystemic inflammatory disease characterized by inflammation of the cartilage and proteoglycan rich structures leading to cartilage damage along with joint, ocular and cardiovascular involvement. Epidemiology The prevalence and annual incidence of Relapsing polychondritis (RP) are not known. The estimated incidence is 1/285,000. The sex ratio appears to be equal and all ethnic groups seem to be affected (with more cases reported among Caucasians). Clinical description Onset is generally sudden and most commonly occurs in the 5th decade of life (age 40 to 55). Cases with early and late onset do occur. RP follows a flaring and remitting course.
Without an agreed-on definition, different researchers may report different numbers of cases and characteristics of the disease. [27] Some morbidity databases are compiled with data supplied by states and territories health authorities, at national levels [28] [29] or larger scale (such as European Hospital Morbidity Database (HMDB)) [30] which may contain hospital discharge data by detailed diagnosis, age and sex. ... Disease category Percent of all YPLLs lost, worldwide [31] Percent of all DALYs lost, worldwide [31] Percent of all YPLLs lost, Europe [31] Percent of all DALYs lost, Europe [31] Percent of all YPLLs lost, US and Canada [31] Percent of all DALYs lost, US and Canada [31] Infectious and parasitic diseases, especially lower respiratory tract infections , diarrhea , AIDS , tuberculosis , and malaria 37% 26% 9% 6% 5% 3% Neuropsychiatric conditions , e.g. depression 2% 13% 3% 19% 5% 28% Injuries , especially motor vehicle accidents 14% 12% 18% 13% 18% 10% Cardiovascular diseases , principally heart attacks and stroke 14% 10% 35% 23% 26% 14% Premature birth and other perinatal deaths 11% 8% 4% 2% 3% 2% Cancer 8% 5% 19% 11% 25% 13% Society and culture [ edit ] Obesity was a status symbol in Renaissance culture: "The Tuscan General Alessandro del Borro ", attributed to Andrea Sacchi , 1645. [32] It is now generally regarded as a disease. ... US National Institute of Mental Health . Archived from the original on 28 May 2010 . Retrieved 18 April 2010 . ^ "Regents Prep: Living Environment: Homeostasis" .
According to Dietitians Australia 25-50% of overweight or obese children with turn out to be obese as adults. [28] Long-term effects of obesity, therefore, include cardiovascular disease ( hypertension and high blood pressure ) and particular types of cancers in particular colon , kidney and breast cancer . [4] [10] Non-alcoholic fatty liver disease (NAFLD) is one of the most common risk factors associated with obesity being characterised as a buildup of fat within the liver cells. [29] Musculoskeletal defects such as osteoarthritis are also said to have a strong link with obesity due to excessive amounts of weight being exerted on the joints. [4] Individuals who have a Body Mass Index (BMI) that is equal to or greater than 25 kg/m2 [3] are also said to have an increased chance of premature morality . [10] Economic costs and consequences [ edit ] As a result of the alarming statistics involving the number of obese children in Australia the consequences have also been extensive to the economy.
Having established the existence of asbestosis on a medical and judicial basis, the report resulted in the first Asbestos Industry Regulations being published in 1931, which came into effect on 1 March 1932. [27] [28] The first lawsuits against asbestos manufacturers occurred in 1929.
A rare pneumoconiosis caused by exposure to asbestos particles. Symptoms may appear many years after exposure and include progressive dyspnea on exertion, dry cough, chest pain, tightness, inspiratory crackles, clubbing of the fingers. Later complications include mesothelioma and lung cancers.
Overview Asbestosis (as-bes-TOE-sis) is a chronic lung disease caused by inhaling asbestos fibers. Prolonged exposure to these fibers can cause lung tissue scarring and shortness of breath. Asbestosis symptoms can range from mild to severe, and usually don't appear until many years after initial exposure. Bronchioles and alveoli in the lungs In your lungs, the main airways, called bronchi, branch off into smaller and smaller passageways. The smallest airways, called bronchioles, lead to tiny air sacs called alveoli.
., extremes of temperature, changes in osmotic or barometric pressure). [26] Vasomotor rhinitis appears to be significantly more common in women than men, leading some researchers to believe that hormone imbalance plays a role. [27] [28] In general, age of onset occurs after 20 years of age, in contrast to allergic rhinitis which can be developed at any age.
Balantidiasis is the only ciliate known to be capable of infecting humans, and swine are the primary reservoir host. [27] Balantidiasis is opportunistic and rare in Western countries. [28] Apicomplexans are parasites of animals and contain an arrangement of organelles called the apical complex.
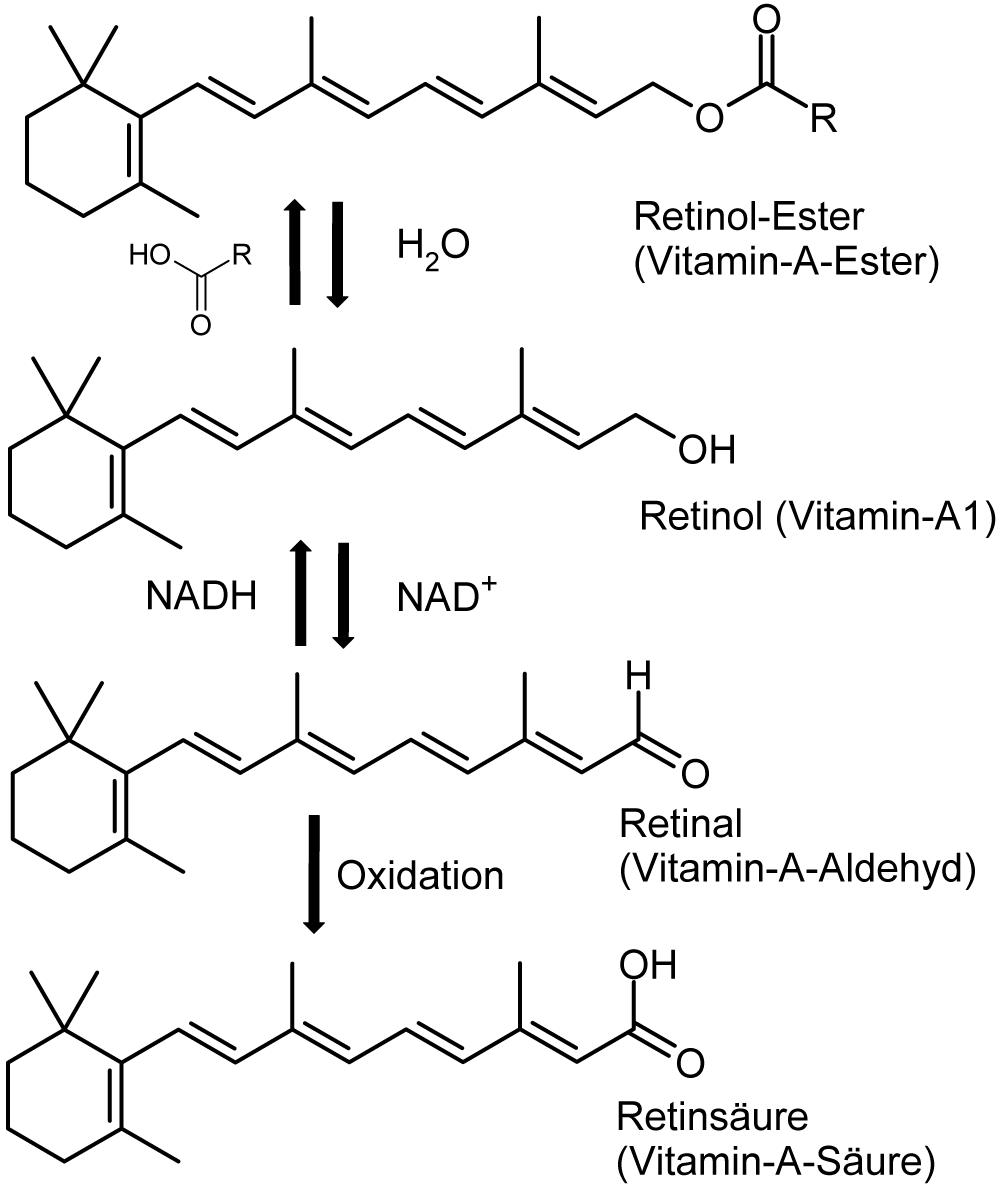
Medications – Many drugs are used on a long-term basis in numerous preventive and therapeutic medical applications, which may lead to hypervitaminosis A. [28] Types of toxicity [ edit ] Acute toxicity occurs over a period of hours or a few days, and is less of a problem than chronic toxicity.
One is removal by injecting compounds that trigger lipolysis , such as steroids or phosphatidylcholine . [24] [27] Other potential methods based on tissue-targeted heating include cauterization , electrosurgery , and harmonic scalpel . [28] Resection of an intermuscular lipoma in the elbow region Intraoperative photo.
This device must be placed using endoscopy, however. [19] [20] [21] Findings on gastroscopy may include edematous gastric mucosa, [22] and hyperperistalsis. [23] Finding on colonoscopy may include: fragile mucosa, [24] segmental erythema, [25] longitudinal ulcer, [26] and loss of haustrations [27] Plain X-ray [ edit ] Plain X-rays are often normal or show non-specific findings. [28] Computed tomography [ edit ] Computed tomography (CT scan) is often used. [29] [30] The accuracy of the CT scan depends on whether a small bowel obstruction (SBO) is present. [31] SBO absent prevalence of mesenteric ischemia 23% sensitivity 64% specificity 92% positive predictive value (at prevalence of 23%) 79% negative predictive value (at prevalence of 23%) 95% SBO present prevalence of mesenteric ischemia 62% sensitivity 83% specificity 93% positive predictive value (at prevalence of 62%) 93% negative predictive value (at prevalence of 62%) 61% Early findings on CT scan include: Mesenteric edema [29] Bowel dilatation [29] Bowel wall thickening [29] Mesenteric stranding [32] Evidence of adjacent solid organ infarctions to the kidney or spleen, consistent with a cardiac embolic shower phenomenon In embolic acute mesenteric ischemia, CT-Angiography can be of great value for diagnosis and treatment.
Case histories often reveal a positive family history of communication disorders . Between 28% and 60% of children with a speech and language deficit have a sibling and/or parent who is also affected. [13] Down syndrome is another example of a genetic causal factor that may result in speech and/or language impairments.
Workers who are not acclimatized or who are wearing impermeable equipment or clothing should be monitored every 15 minutes. [25] NIOSH and OSHA have also created a Heat Index App for mobile devices that provides information on temperature, humidity, risk of heat illness, as well as hourly forecasts of temperature and information on how to prevent and treat heat illnesses. [26] Prevention [ edit ] Working in hot conditions can make the body lose fluids through sweating, so workers must drink extra water in these conditions to replenish those fluids and prevent dehydration . [27] Employers can establish prevention programs, which focus on having protocols to gradually increases workloads and concede on allowing on more breaks for new hired workers. [28] Employers can control heat stress through engineering controls, work practices, providing training, implementing an acclimatization schedule, providing water and encouraging workers to drink often, and ensuring workers take appropriate rest breaks to cool down. [29] Engineering controls [ edit ] Employers can provide air conditioners for indoor work spaces and for indoor break areas.
Stage [23] Histopathology [23] 4 Year relapse-free survival (RFS) or event-free survival (EFS) [23] 4 Year overall survival (OS) [23] Treatment [23] Stage I [23] Favorable histology in children younger than 24 months or tumor weight less than 550g 85% 98% Surgery only (should be done only within the context of a clinical trial) Favorable histology in children older than 24 months or tumor weight more than 550g 94% RFS 98% Nephrectomy + lymph node sampling followed by regimen EE-4A Diffuse anaplastic 68% EFS 80% Nephrectomy + lymph node sampling followed by regimen EE-4A and radiotherapy Stage II [23] Favorable histology 86% RFS 98% Nephrectomy + lymph node sampling followed by regimen EE-4A Focal anaplastic 80% EFS 80% Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen DD-4A Diffuse anaplastic 83% EFS 82% Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen I Stage III [23] Favorable histology 87% RFS 94% Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen DD-4A Focal anaplastic 88% RFS 100% (8 people in study) Nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen DD-4A Focal anaplastic (preoperative treatment) 71% RFS 71% Preoperative treatment with regimen DD-4A followed by nephrectomy + lymph node sampling and abdominal radiotherapy Diffuse anaplastic 46% EFS 53% Preoperative treatment with regimen I followed by nephrectomy + lymph node sampling and abdominal radiotherapy Diffuse anaplastic 65% EFS 67% Immediate nephrectomy + lymph node sampling followed by abdominal radiotherapy and regimen I Stage IV [23] Favorable histology 76% RFS 86% Nephrectomy + lymph node sampling, followed by abdominal radiotherapy, bilateral pulmonary radiotherapy, and regimen DD-4A Focal anaplastic 61% EFS 72% Nephrectomy + lymph node sampling, followed by abdominal radiotherapy, bilateral pulmonary radiotherapy, and regimen DD-4A Diffuse anaplastic 33% EFS 33% Immediate nephrectomy + lymph node sampling followed by abdominal radiotherapy, whole-lung radiotherapy, and regimen I Diffuse anaplastic (preoperative treatment) 31% EFS 44% Preoperative treatment with regimen I followed by nephrectomy + lymph node sampling followed by abdominal radiotherapy, whole-lung radiotherapy Stage V [23] Overall 61% EFS 80% Favorable histology 65% 87% Preoperative treatment with regimen DD-4A , followed by nephron sparing surgery or nephrecomy, staging of tumors, and chemotherapy and/or radiotherapy based on pathology and staging Focal anaplastic 76% 88% Preoperative treatment with regimen DD-4A , followed by nephron sparing surgery or nephrecomy, staging of tumors, and chemotherapy and/or radiotherapy based on pathology and staging Diffuse anaplastic 25% 42% Preoperative treatment with regimen DD-4A , followed by nephron sparing surgery or nephrecomy, staging of tumors, and chemotherapy and/or radiotherapy based on pathology and staging In case of relapse of Wilms' tumor, the 4-year survival rate for children with a standard-risk has been estimated to be 80%. [24] Epidemiology [ edit ] Wilms tumor is the most common malignant renal tumor in children. [25] There are a number of rare genetic syndromes that have been linked to an increased risk of developing Wilms Tumor. [26] Screening guidelines vary between countries; however health care professionals are recommending regular ultrasound screening for people with associated genetic syndromes. [26] Wilms' tumor affects approximately one person per 10,000 worldwide before the age of 15 years. [27] People of African descent may have slightly higher rates of Wilms' tumor. [27] The peak age of Wilms' tumor is 3 to 4 years and most cases occur before the age of 10 years. [28] A genetic predisposition to Wilms' tumor in individuals with aniridia has been established, due to deletions in the p13 band on chromosome 11. [29] History [ edit ] Dr.
A number sign (#) is used with this entry because of evidence that susceptibility to Wilms tumor can be caused by mutation in the REST (600571) gene on 4q12. For a general phenotypic description and discussion of genetic heterogeneity of Wilms tumor, see WT1 (194070). Molecular Genetics To identify predisposition genes for Wilms tumor, Mahamdallie et al. (2015) performed exome sequencing in 24 individuals with Wilms tumor from 12 families and identified 2 different frameshift mutations (600571.0001, 600571.0002) that segregated with the disease in 2 unrelated families. Neither was present in the ICR1000 and ExAC browsers. The mutations were confirmed by Sanger sequencing. Subsequently, Mahamdallie et al. (2015) performed Sanger sequencing of the full coding sequence and intron-exon boundaries of the REST gene in 38 individuals with familial Wilms tumor from 27 families.
A number sign (#) is used with this entry because of evidence that susceptibility to Wilms tumor can be caused by mutation in the POU6F2 gene (609062) on chromosome 7p14. For a general phenotypic description and a discussion of genetic heterogeneity of Wilms tumor, see WT1 (194070). Cytogenetics Wilmore et al. (1994) observed a Wilms tumor patient who had a constitutional balanced translocation between chromosomes 1 and 7, t(1;7)(q42;p15), and suggested that the breakpoints might represent a Wilms tumor predisposition gene. Cytogenetic analysis of the tumor from this patient revealed an acquired abnormality of the other chromosome 7, resulting in an isochromosome of the long arm. This confirmed the monosomy of 7p and trisomy of 7q in the tumor of the translocation patient, and in addition a loss of 7p alleles was identified in a WT from a bilaterally affected patient.
A number sign (#) is used with this entry because of evidence that Wilms tumor-2 (WT2) is caused by mutation of the H19/IGF2-imprinting control region (ICR1; 616186) on chromosome 11p15. ICR1 controls imprinted expression of H19 (103280) and IGF2 (147470). ICR1 and a neighboring imprinted gene cluster are implicated in Beckwith-Wiedemann syndrome (BWS; 130650), of which Wilms tumor is a common feature. For a general phenotypic description and discussion of genetic heterogeneity of Wilms tumor, see WT1 (194070). Mapping Using a range of probes for chromosome 11, Mannens et al. (1988) demonstrated that loss of heterozygosity in Wilms tumors may involve chromosome 11p15.5 in addition to 11p13.
A number sign (#) is used with this entry because Wilms tumor-1 (WT1) is caused by heterozygous mutation in the WT1 gene (607102) on chromosome 11p13. Description Wilms tumor is the most common renal tumor of childhood, occurring with an incidence of 1 in 10,000 and with a median age of diagnosis between 3 and 4 years of age. Wilms tumours are thought to develop from abnormally persistent embryonal cells within nephrogenic rests. Histologically, Wilms tumor mirrors the development of the normal kidney and classically consists of 3 cell types: blastema, epithelia, and stroma (summary by Slade et al., 2010). Genetic Heterogeneity of Wilms Tumor Susceptibility to Wilms tumor is genetically heterogeneous.
For a general phenotypic description and a discussion of genetic heterogeneity of Wilms tumor, see WT1 (194070). Mapping With loss of heterozygosity studies, Maw et al. (1992) concluded that a third Wilms tumor locus (WT3) is on 16q. In addition to loss on chromosome 11p (11 of 25 informative Wilms tumors), there was significant loss on 16q (9 of 45 informative tumors), while the total frequency of allele loss excluding these loci was low (9 of 426 total informative loci). They screened loci on 33 autosomal arms. The parental origin of the lost chromosome 16q allele was paternal in 4 and maternal in 4 sporadic tumors tested. Thus, unlike chromosome 11p, alleles of either parental origin are lost on 16q.
A rare malignant renal tumor, typically affecting the pediatric population, characterized by an abnormal proliferation of cells that resemble the kidney cells of an embryo (metanephroma), leading to the term embryonal tumor. Epidemiology The annual incidence is estimated at about 1/10,000 births and it affects boys as well as girls. Clinical description Nephroblastoma mainly affects young children, between the ages 1 and 5 years, but 15% of nephroblastomas occur before the age of 1 year and 2% after the age of 8 years. Adult forms are very rare. An abdominal mass (unilateral in most cases) is frequently present. Patients sometimes experience abdominal pain (around 10% of cases), hypertension, fever (20% of cases), hematuria and anemia.
For a general phenotypic description and discussion of genetic heterogeneity of Wilms tumor, see WT1 (194070). Clinical Features Rahman et al. (1996) described a large Canadian family with 7 confirmed cases of Wilms tumor in 3 generations. No congenital abnormalities or other cancers had been observed in the family. The average age of presentation was 5 years (age range of 2 to 12 years), which is older than the average age of diagnosis of sporadic WT (3 to 4 years). Typical triphasic histology with stromal, blastemal, and epithelial elements was found in 5 tumors, while the sixth tumor was predominantly myogenic.
Overview Wilms tumor is a rare kidney cancer that mainly affects children. Also known as nephroblastoma, it's the most common cancer of the kidneys in children. Wilms tumor most often affects children ages 3 to 4. It becomes much less common after age 5, but it can affect older children and even adults. Wilms tumor mostly occurs in just one kidney. But it can sometimes be in both kidneys at the same time. Over the years, progress in the diagnosis and treatment of Wilms tumor has greatly improved the prognosis for children with this disease.
Wilms tumor is a form of kidney cancer that primarily develops in children. Nearly all cases of Wilms tumor are diagnosed before the age of 10, with two-thirds being found before age 5. Wilms tumor is often first noticed because of abdominal swelling or a mass in the kidney that can be felt upon physical examination. Some affected children have abdominal pain, fever, a low number of red blood cells (anemia ), blood in the urine (hematuria), or high blood pressure (hypertension). Additional signs of Wilms tumor can include loss of appetite, weight loss, nausea, vomiting, and tiredness (lethargy).
Within that subset, African & Asian women were more likely to have a tumor, but this was not relevant to the prevalence of the disease within those racial groups. [9] Society and culture [ edit ] Anti-NMDA receptor encephalitis is suspected of being an underlying cause of historical accounts of demonic possession . [27] [28] [29] [30] New York Post reporter Susannah Cahalan wrote a book titled Brain on Fire: My Month of Madness about her experience with the disease. [31] This has subsequently been turned into a film of the same name . [32] Dallas Cowboys defensive lineman Amobi Okoye spent 17 months battling anti-NMDA receptor encephalitis.
Passive smoking [ edit ] Main article: Risk to children of passive smoking Passive smoking is associated with many risks to children, including, sudden infant death syndrome (SIDS), [23] [24] asthma , [25] [26] lung infections, [27] [28] [29] [30] impaired respiratory function and slowed lung growth, [8] Crohn's disease , [31] learning difficulties and neurobehavioral effects, [32] [33] an increase in tooth decay , [34] and an increased risk of middle ear infections. [35] [36] Multigenerational effect [ edit ] Main article: Epigenetic effects of smoking A grandmother who smokes during her daughter's pregnancy transmits an increased risk of asthma to her grandchildren, even if the second-generation mother does not smoke. [37] The multigenerational epigenetic effect of nicotine on lung function has already been demonstrated. [37] See also [ edit ] Medicine portal Health effects of tobacco Alcohol and pregnancy References [ edit ] ^ Ness, Roberta B.; Grisso, Jeane Ann; Hirschinger, Nancy; Markovic, Nina; Shaw, Leslie M.; Day, Nancy L.; Kline, Jennie (1999).
Any discoveries on approaches with dry eye will help further the oculoplastic surgeries. [28] Etymology [ edit ] Ptosis is derived from the Greek word πτῶσις ("fall"), and is defined as the "abnormal lowering or prolapse of an organ or body part".
Viewing videotapes of self-modeling should be shown over a spaced out period of time of approximately 6 weeks. [24] [25] [26] Drug treatments [ edit ] Some practitioners believe there would be evidence indicating anxiolytics to be helpful in treating children and adults with selective mutism, [28] to decrease anxiety levels and thereby speed the process of therapy.
It also requires observations of the child's behavior with unfamiliar adults and a comprehensive history of the child's early caregiving environment including, for example, pediatricians, teachers, or caseworkers. [4] In the US, initial evaluations may be conducted by psychologists, psychiatrists, Licensed Marriage and Family Therapists, Licensed Professional Counselors, specialist Licensed Clinical Social Workers or psychiatric nurses. [28] In the UK, the British Association for Adoption and Fostering (BAAF) advise that only a psychiatrist can diagnose an attachment disorder and that any assessment must include a comprehensive evaluation of the child's individual and family history. [29] According to the AACAP Practice Parameter (2005) the question of whether attachment disorders can reliably be diagnosed in older children and adults has not been resolved. ... "Relationship between behavioral reactivity at 4 months and attachment classification at 14 months in a selected sample". Infant Behavior and Development . 28 (4): 492–502. doi : 10.1016/j.infbeh.2005.06.002 . ^ a b Prior & Glaser (2006), p. 219. ^ Zeanah CH, Fox NA (2004). ... Retrieved on 13 February 2008. ^ For examples see Reactive Attachment Disorder Archived 28 December 2007 at the Wayback Machine , DCFS, State of Illinois and DBHS Practice Protocol: Disturbances and Disorders of Attachment (PDF), Arizona Department of Health Services, 2 October 2006.
Overview Reactive attachment disorder is a rare but serious condition in which an infant or young child doesn't establish healthy attachments with parents or caregivers. Reactive attachment disorder may develop if the child's basic needs for comfort, affection and nurturing aren't met and loving, caring, stable attachments with others are not established. With appropriate treatment, children who have reactive attachment disorder may develop more stable and healthy relationships with caregivers and others. Treatments for reactive attachment disorder include learning how to create a stable, nurturing environment and providing positive child and caregiver interactions. Parent or caregiver counseling and education can help. Symptoms Reactive attachment disorder usually starts in infancy.
These symptoms accord with the DSM criteria for reactive attachment disorder. [25] Either of these behavior patterns may create a developmental trajectory leading ever farther from typical attachment processes such as the development of an internal working model of social relationships that facilitates both the giving and the receiving of care from others. [26] [27] Atypical development of fearfulness, with a constitutional tendency either to excessive or inadequate fear reactions, might be necessary before an infant is vulnerable to the effects of poor attachment experiences. [28] Alternatively, the two variations of RAD may develop from the same inability to develop "stranger-wariness" due to inadequate care. ... "Relationship between behavioral reactivity at 4 months and attachment classification at 14 months in a selected sample". Infant Behavior and Development . 28 (4): 492–502. doi : 10.1016/j.infbeh.2005.06.002 . ^ a b Prior and Glaser p. ^ Mercer (2006) p. ^ Fonagy P, Gergely G, Jurist EL, Target M (2006). ... Archived from the original (PDF) on 2007-09-28 . Retrieved 2008-03-16 . References [ edit ] Ainsworth.
. ^ Oaklander AL, Long DM, Larvie M, Davidson CJ (February 28, 2013). "Case 7-2013: A 77-year-old woman with long-standing unilateral thoracic pain and incontinence".
A disorder that is characterized by the presence of cerebrospinal fluid-filled nerve root cysts most commonly found at the sacral level of the spine, although they can be found in any section of the spine, which can cause progressively painful radiculopathy. Epidemiology The annual incidence of perineural cysts is estimated at approximately 5%, although large cysts that cause symptoms are relatively rare with annual incidence estimated at less than 1/2,000. Women are affected more frequently than men. Clinical description Patients with perineural cysts present with pain in the area of the nerves affected by the cyst, muscle weakness, difficulty sitting for prolonged periods, loss of sensation, loss of reflexes, pain when sneezing or coughing, swelling over the sacral area, parasthesias, headaches, sciatica, and bowel, bladder and sexual dysfunction. The cysts typically occur along the posterior nerve roots and can be valved or nonvalved. The main feature that distinguishes perineural cysts from other spinal lesions is the presence of spinal nerve root fibres within the cyst wall or in the cyst cavity.
Tarlov cysts are fluid-filled sacs that are usually found at the bottom of the spine (the sacrum). They grow in the roots of the nerves that grow out of the spinal cord. Most of the time, Tarlov cysts don't cause symptoms. When symptoms occur, they may include pain in the lower back, buttocks, or stomach. Other symptoms may include muscle weakness, numbness, loss of bladder or bowel control, or sexual dysfunction. Without treatment, Tarlov cysts may cause permanent nerve damage. The cause of Tarlov cysts is unknown.