-
Enteropathy-Associated T-Cell Lymphoma
Wikipedia
One of these diseases, Extranodal NK/T cell lymphoma, nasal type may develop primarily in the small intestine but unlike EATL often involves lesions in the nasal cavity, pharynx , lung, skin, or other tissues. [28] Furthermore, the malignant T cells in this disease express readily detectable products encoded by the Epstein-Barr virus's genes [29] whereas those of EATL are not infected with this virus and therefore do not express these viral products. [8] Indolent T cell lymphoproliferative disorder of the gastrointestinal tract (ITCLD-GT)) is a rare, slowly progressive, and potentially premalignant disorder of the GI tract that may be mistaken of EATL, [4] particularly with respect to the severity of its symptoms, the gross pathology of its intestinal lesions, [8] and the presence in its intestinal lesions of T cells that have monoclonal rearrangements of their TCR as well as genetic abnormalities in the JAK/STAT signaling pathway. [30] Unlike EATL, ITCLD-GT is not associated with coeliac disease; often involves symptomatic lesions of the upper GI tract (i.e. stomach, esophagus, and pharynx ); [30] and has GI tract lesions populated by T cells that express CD3 (rather than iCD3), do not express CD56, and, in many cases, express an abnormal STAT3 - JAK2 fusion gene . [31] Prevention [ edit ] Strict adherence to a gluten-free diet has been shown in some but not all studies to prevent in a significant number of cases the progression of coeliac disease to Type I RCD, Type II RCD, and EATL. [9] For example, an Italian study of 1757 patients found that the morbidity of EATL over 3 years fell from 6.42 to 0.22 in coeliac disease patients kept on a strict gluten-free diet.STAT5B, TRBV20OR9-2, NCAM1, ITGAE, SOAT1, TP53, MYC, GUCY2D, CDR3, TIA1, ZAP70, ABL1, SSTR4, NCR1, CLEC10A, CXCR6, ISCU, SETD2, RTEL1, TET2, ACKR3, LPAR2, NOS2, NOTCH1, ADRA1A, NOS1, MYO9B, MATK, HLA-DRB1, HLA-DQB1, GZMB, GPR42, EDNRA, CDKN2A, TNFRSF8, CD19, BRS3, ADRA2B, H3P10

-
Snakebite
Wikipedia
However, subduing and killing prey became more difficult for the smaller snakes, leading to the evolution of snake venom. [27] Other research on Toxicofera , a hypothetical clade thought to be ancestral to most living reptiles, suggests an earlier time frame for the evolution of snake venom, possibly to the order of tens of millions of years, during the Late Cretaceous . [28] Snake venom is produced in modified parotid glands normally responsible for secreting saliva. ... Current Pharmaceutical Design . 13 (28): 2935–50. doi : 10.2174/138161207782023784 . ... Archived (PDF) from the original on 28 April 2011 . Retrieved 24 July 2009 . ^ Bhaumik, Soumyadeep; Kallakuri, Sudha; Kaur, Amanpreet; Devarapalli, Siddhardha; Daniel, Mercian (November 2020).

-
Sexually Transmitted Infection
Wikipedia
Depending on the disease, some untreated STIs can lead to infertility , chronic pain or death. [14] The presence of an STI in prepubescent children may indicate sexual abuse . [15] Cause Transmission A sexually transmitted infection present in a pregnant woman may be passed on to the infant before or after birth. [16] Risk of transmission per unprotected sexual act with an infected person [17] [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] [29] Known risks Possible Performing oral sex on a man Throat chlamydia [17] Throat gonorrhea [17] (25–30%) Herpes (rare) HPV [18] Syphilis [17] (1%) [19] Hepatitis B (low risk) [20] HIV (0.01%) [21] Hepatitis C (unknown) Performing oral sex on a woman Herpes HPV [18] Throat gonorrhea [17] Throat chlamydia [17] Receiving oral sex—man Chlamydia Gonorrhea [17] Herpes Syphilis [17] (1%) [19] HPV Receiving oral sex—woman Herpes HPV Bacterial vaginosis [17] Gonorrhea [17] Vaginal sex—man Chlamydia (30–50%) [20] Crabs Scabies Gonorrhea (22%) [22] Hepatitis B Herpes (0.07% for HSV-2 ) [23] HIV (0.05%) [21] [23] HPV (high: around 40–50%) [24] Mycoplasma hominis infection [30] [31] [32] [33] [34] Mycoplasma genitalium [35] [36] [37] Syphilis Trichomoniasis Ureaplasma infection [38] [39] [34] Hepatitis C Vaginal sex—woman Chlamydia (30–50%) [20] Crabs Scabies Gonorrhea (47%) [25] Hepatitis B (50–70%) Herpes HIV (0.1%) [21] HPV (high; [20] around 40–50%) [24] Mycoplasma hominis infection [30] [31] [34] Syphilis Trichomoniasis Ureaplasma infection [38] [39] [34] Hepatitis C Anal sex —insertive Chlamydia Crabs Scabies (40%) Gonorrhea Hepatitis B Herpes HIV (0.62%) [27] HPV Syphilis (14%) [19] Hepatitis C Anal sex —receptive Chlamydia Crabs Scabies Gonorrhea Hepatitis B Herpes HIV (1.7%) [27] HPV Syphilis (1.4%) [19] Hepatitis C Anilingus Amoebiasis Cryptosporidiosis (1%) Giardiasis [40] Hepatitis A [41] (1%) Shigellosis [42] (1%) HPV (1%) Bacterial Chancroid ( Haemophilus ducreyi ) Chlamydia ( Chlamydia trachomatis ) Gonorrhea ( Neisseria gonorrhoeae ), colloquially known as "the clap" Granuloma inguinale or ( Klebsiella granulomatis ) Mycoplasma genitalium [31] [43] [44] [45] Mycoplasma hominis [30] [31] [32] [33] [46] Syphilis ( Treponema pallidum ) Ureaplasma infection [38] [39] Fungal Candidiasis (yeast infection) Viral Micrograph showing the viral cytopathic effect of herpes (ground glass nuclear inclusions, multi-nucleation). ... Retrieved 8 December 2017 . ^ International technical guidance on sexuality education: An evidence-informed approach (PDF) . Paris: UNESCO. 2018. p. 28. ISBN 978-92-3-100259-5 . ^ Centers for Disease Control Prevention (CDC) (August 2012). ... Cdc.gov. Archived from the original on 28 June 2013 . Retrieved 30 June 2013 . ^ MedlinePlus Encyclopedia : Gonorrhea ^ "STD Facts – Syphilis" .SULT2A1, ZAP70, KLK3, IFNE, AGRP, PREP, PAEP, ARTN, PTPN22, CXCL8, IL1B, TLR4, EXTL3, ERVK-6, CCL27, TNFRSF1A, UBE2B, WAS, ARSH, MARCHF8, ANC, MESP2, ARID1A, EMB, ESPL1, SART3, SMC5, CPAT1, CADM1, NLRP3, MLST8, ERVW-1, LHPP, TLR9, CRLS1, SARS2, FBXW7, IMPACT, PLXNA3, DDX41, RRM2, TRIM21, DEFA5, HSPD1, HSPA4, HLA-A, GRB2, GPI, FCGRT, CUX1, SRY, CRP, CCR5, CD38, CAMP, CALR, B2M, IFNA1, IFNA13, IFNG, IL6, IL16, CXCL10, KIT, LRP1, MSMB, NDUFAB1, NHS, PNP, PKHD1, PMAIP1, RPS6KA3, APP, SARS1, ERVK-20
-
Bronchiolitis
Wikipedia
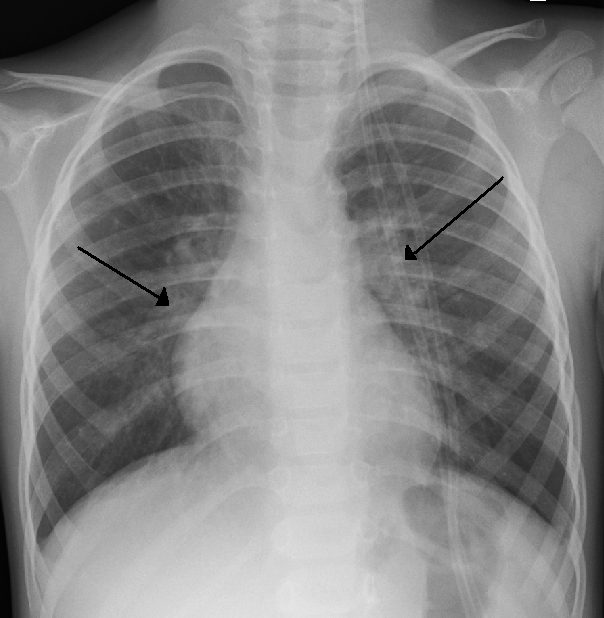
Chest X-ray is sometimes useful to exclude bacterial pneumonia , but not indicated in routine cases. [15] Chest x-ray may also be useful in people with impending respiratory failure. [16] Additional testing such as blood cultures, complete blood count, and electrolyte analyses are not recommended for routine use although may be useful in children with multiple comorbidities or signs of sepsis or pneumonia. [5] [16] Testing for the specific viral cause can be done but has little effect on management and thus is not routinely recommended. [15] RSV testing by direct immunofluorescence testing on nasopharyngeal aspirate had a sensitivity of 61% and specificity of 89%. [13] [16] Identification of those who are RSV-positive can help for disease surveillance, grouping ("cohorting") people together in hospital wards to prevent cross infection, predicting whether the disease course has peaked yet, and reducing the need for other diagnostic procedures (by providing confidence that a cause has been identified). [5] Identification of the virus may help reduce the use of antibiotics. [16] Infants with bronchiolitis between the age of two and three months have a second infection by bacteria (usually a urinary tract infection ) less than 6% of the time. [17] When further evaluated with a urinalysis, infants with bronchiolitis had a concomitant UTI 0.8% of the time. [18] Preliminary studies have suggested that elevated procalcitonin levels may assist clinicians in determining the presence of bacterial co-infection, which could prevent unnecessary antibiotic use and costs. [19] Differential diagnosis [ edit ] There are many childhood illnesses that can present with respiratory symptoms, particularly persistent cough and wheezing. [8] [20] Bronchiolitis may be differentiated from some of these by the characteristic pattern of preceding febrile upper respiratory tract symptoms lasting for 1 to 3 days followed by the persistent cough, tachypnea, and wheezing. [20] However, some infants may present without fever (30% of cases) or may present with apnea without other signs or with poor weight gain prior to onset of symptoms. [20] In such cases, additional laboratory testing and radiographic imaging may be useful. [8] [20] The following are some other diagnoses to consider in an infant presenting with signs of bronchiolitis: [ citation needed ] Asthma and reactive airway disease Bacterial pneumonia Congenital heart disease Heart failure Whooping cough Allergic reaction Cystic fibrosis Chronic pulmonary disease Foreign body aspiration Vascular ring Prevention [ edit ] Prevention of bronchiolitis relies strongly on measures to reduce the spread of the viruses that cause respiratory infections (that is, handwashing, and avoiding exposure to those symptomatic with respiratory infections). [5] [8] Guidelines are mixed on the use of gloves, aprons, or personal protective equipment . [5] In addition to good hygiene, an improved immune system is a great tool for prevention. [ citation needed ] One way to improve the immune system is to feed the infant with breast milk, especially during the first month of life. [14] [21] Respiratory infections were shown to be significantly less common among breastfed infants and fully breastfed RSV-positive hospitalized infants had shorter hospital stays than non or partially breastfed infants. [8] Guidelines recommend exclusive breastfeeding for infants for the first 6 months of life. [8] Palivizumab , a monoclonal antibody against RSV, can be administered to prevent bronchiolitis to infants less than one year of age that were born very prematurely or that have underlying heart disease or chronic lung disease of prematurity. [8] Passive immunization therapy requires monthly injections during winter. [8] Otherwise healthy premature infants that were born after a gestational age of 29 weeks should not be administered palivizumab as the harms outweigh the benefits. [8] Passive protection through the administration of other novel monoclonal antibodies is also under evaluation. [16] The development of immunizations for RSV are being developed but there are none available currently. [16] [22] Tobacco smoke exposure has been shown to increase both the rates of lower respiratory disease in infants as well as the risk and severity of bronchiolitis. [8] Tobacco smoke lingers in the environment for prolonged periods and on clothing even when smoking outside the home. [8] Guidelines recommend that parents be fully educated on the risks of tobacco smoke exposure on children with bronchiolitis. [8] [20] Management [ edit ] Treatment of bronchiolitis is usually focused on the hydration and symptoms instead of the infection itself since the infection will run its course and complications are typically from the symptoms themselves. [23] Without active treatment, half of cases will go away in 13 days and 90% in three weeks. [24] Children with severe symptoms, especially poor feeding or dehydration, may be considered for hospital admission. [5] Oxygen saturation under 90%-92% as measured with pulse oximetry is also frequently used as an indicator of need for hospitalization. [5] High-risk infants, apnea , cyanosis , malnutrition, and diagnostic uncertainty are additional indications for hospitalization. [5] Most guidelines recommend sufficient fluids and nutritional support for affected children. [5] Measures for which the recommendations were mixed include nebulized hypertonic saline, nebulized epinephrine , and nasal suctioning. [1] [5] [25] [26] Treatments which the evidence does not support include salbutamol , steroids , antibiotics , antivirals , heliox , continuous positive airway pressure (CPAP), chest physiotherapy , and cool mist or steam inhalation. [1] [27] [28] [29] [30] Diet [ edit ] Maintaining hydration is an important part of management of bronchiolitis. [8] [16] [31] Infants with mild pulmonary symptoms may require only observation if feeding is unaffected. [8] However, oral intake may be affected by nasal secretions and increased work of breathing. [8] Poor feeding or dehydration, defined as less than 50% of usual intake, is often cited as an indication for hospital admission. [5] Guidelines recommend the use of nasogastric or intravenous fluids in children with bronchiolitis who cannot maintain usual oral intake. [8] [20] [16] The risk of health care caused hyponatremia and fluid retention are minimal with the use of isotonic fluids such as normal saline , breast milk, or formula. [8] Oxygen [ edit ] A newborn wearing a nasal CPAP device.SLC35C1, TAP2, CXCL8, CCL5, SDCCAG8, PLCG2, PLEC, IL10, TAPBP, TAP1, TLR4, IFNG, VDR, CD14, TLR1, TLR10, IL4, TLR2, IL9, SFTPD, NOS2, IL13, IL17A, TNF, SFTPA1, IL5, COPD, IL18, JUN, ISYNA1, TLR9, HMGB1, IFNL3, CENPJ, CCL2, PEA15, NR1I2, ADRB2, SCGB1A1, TNFRSF1A, TLR3, PRDX2, SLC2A1, IL1RL1, TLR6, PPIP5K1, ABCB6, PLF, MIR27A, IFNL1, PGAM5, IFNLR1, ORMDL3, IL33, TSLP, SEMA4A, MAVS, TLR7, HPGDS, KLRK1, PTGDR2, RAPGEF4, SLC27A4, POSTN, BET1, ATP6AP2, CX3CL1, PTGDS, CCL4, FUT2, IFNA13, IFNA5, IFNA1, IFIT1, IFI27, ICAM1, GSTT1, GSTP1, NR3C1, GC, DHPS, CCL3, CX3CR1, CTLA4, CRP, COL5A1, CCR5, CLC, CD38, CD19, RUNX3, CAMP, IL2, IL3, IL4R, IL6, RNASE3, RNASE2, MOK, NECTIN1, AGER, PTGDR, PRF1, PMCH, SERPINF2, SERPINE1, OCA2, NFKBIA, MUC5AC, MBL2, LTA, LAIR1, IRF3, IL15, IL10RB, CXCR2, IL7, KLRC4-KLRK1
-
Epstein–barr Virus-Associated Lymphoproliferative Diseases
Wikipedia
Mild and clearly uncomplicated cases can be treated conservatively focusing on obtaining relief of symptoms such as skin irritation, fever, and malaise. [28] However, cases with evidence of significant complications of CAEFV such as the development of hemophagocytosis, NK/T cell lymphoma, or aggressive NK cell lymphoma, support the use of the chemotherapeutic regimens directed at these complications. Cases of EBV+ SMBA associated with clear evidence of concurrent aggressive CAEBV have been treated with relative success by the 3 step regimen used to treat CAEBV. [25] Rare cases of SMBA have been reported to occur in individuals who have no apparent predisposing disease but later develop CAEBV. [27] [28] Such cases require careful evaluation and follow-up for development of a predisposing disorder. [28] Hydroa vacciniforme-like lymphoproliferative disease [ edit ] Main article: Hydroa vacciniforme Hydroa vacciniforme is a rare photodermatitis reaction in which sunlight causes itchy skin papules and vesicles that develop crusts and eventually become scarred tissue.
-
Benzodiazepine Use Disorder
Wikipedia
Those who use stimulant and depressant drugs are more likely to report adverse reactions from stimulant use, more likely to be injecting stimulants and more likely to have been treated for a drug problem than those using stimulant but not depressant drugs. [25] Risk factors [ edit ] See also: List of benzodiazepines Individuals with a substance abuse history are at an increased risk of misusing benzodiazepines. [26] Several (primary research) studies, even into the last decade, claimed, that individuals with a history of familial abuse of alcohol or who are siblings or children of alcoholics appeared to respond differently to benzodiazepines than so called genetically healthy persons, with males experiencing increased euphoric effects and females having exaggerated responses to the adverse effects of benzodiazepines. [27] [28] [29] [30] Whilst all benzodiazepines have abuse potential, certain characteristics increase the potential of particular benzodiazepines for abuse.

-
Koro (Medicine)
Wikipedia
Secondary koro is proposed to have co-morbidity with a CNS disorder , another psychiatric disorder , or possible drug use. [10] Traditional Chinese medicine recognises koro as a sexual disease and classifies it into two categories, namely "cold conglomeration in liver " and "depletion of kidney 's yang ". [27] Differential diagnosis [ edit ] Men who present with this complaint may have koro, but they may also be misinformed about normal genital size. [6] Additionally, they may be suffering from penile dysmorphophobia. [28] Penile dysmorphophobia is related to body dysmorphic disorder (BDD), defined by the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (Text Revision) ( DSM-IV -TR) as a condition marked by excessive preoccupation with an imaginary or minor defect in a facial feature or localized part of the body.
-
Darier's Disease
Wikipedia
Using this technique, he was able to uncover the origins of Darier’s disease and a host of others that also bear his name. [28] James Clark White, a dermatologist at Harvard Medical School, independently characterized and published his observations on this dermatological disorder in the same year as Darier (1889), which is why Darier's disease is also referred to as Darier-White disease.ATP2A2, CEP290, TMEM67, BBS9, KIAA0586, WDR19, TMEM231, DYNC2H1, LRRCC1, TRAPPC3, BBS5, ARL13B, BBS2, ACE, ATP2C1, ATP2A3, IL6, TRPC1, PLA2G1B, SELENBP1, TGM5, CLOCK, OTP, ADRA1D, SMOC1, HPGDS, CCHCR1, POGLUT1, THOC5, PTH2, SLCO6A1, PER3, SOD1, WFS1, TGM3, CANX, CNR1, CRY1, DNAH8, DSP, EPHA3, IGFALS, IL2, CXCL8, KRT1, KRT14, KRT16, PAH, PTEN, PTH, PTGS2, PTPN11, SAT1, ATXN2, SHBG, APOE, GSTK1

-
Hip Fracture
Wikipedia
Skeletal traction pending surgery is not supported by the evidence. [26] Regional nerve blocks are useful for pain management in hip fractures. [27] Surgery can be performed under general anaesthesia or with neuraxial techniques - choice is based on surgical and patient factors, as outcomes such as mortality and post-procedure complications including pneumonia, MI, stroke or confusion, are not affected by anaesthetic technique. [28] Red blood cell transfusion is common for people undergoing hip fracture surgery due to the blood loss sustained during surgery and from the injury.

-
Sickle Cell Disease
Wikipedia
Most patients can be managed supportively; some need blood transfusion. [28] Haemolytic crisis [ edit ] Haemolytic crises are acute accelerated drops in haemoglobin level. ... Retrieved 2010-11-27 . ^ Kumar V, Abbas AK, Fausto N, Aster J (28 May 2009). Robbins and Cotran Pathologic Basis of Disease (Professional Edition: Expert Consult – Online (Robbins Pathology) ed.). ... PMID 21615795 . ^ Kumar V, Abbas AK, Fausto N, Aster J (28 May 2009). Robbins and Cotran Pathologic Basis of Disease (Professional Edition: Expert Consult – Online (Robbins Pathology) ed.).HBB, NFE2L2, HP, TNF, VCAM1, DHODH, NPPB, CAD, CACNA1C, UMPS, HMOX1, SPTA1, BCL11A, HBG2, UGT1A8, HBE1, UGT1A10, UGT1A4, UGT1A7, UGT1A6, UGT1A3, UGT1A9, UGT1A5, G6PD, UGT1A1, ARAP1, OR51B5, UBIAD1, EDN1, MYB, OR51I2, MCC, RN7SL263P, SELP, LINC01847, PGF, MUC4, MTHFR, NPRL3, RABEP1, HBG1, CD34, HBA2, HBA1, GABPA, SORCS2, NOS3, HBS1L, F5, HPX, SCD, RHCE, ALB, SELL, VWF, APOL1, MBL2, RHD, F2, CAT, HAMP, CSF3, BCAM, VEGFA, REN, F3, EPO, HPGDS, CCR5, UGT1A, IL6, HIF1A, IL1B, CXCL8, HLA-DRB1, SCT, SELE, SERPINE1, ABO, CYP2D6, PSMA7, GSTT1, GSTK1, FUT1, KLF1, DLL3, IFNG, IGF1, CCL2, SOD2, TBX6, IL4, SLCO6A1, TRV-AAC1-4, CSF2, TGFB1, MIPEP, ANXA5, SPHK1, HLA-DQB1, ANXA1, KL, THBD, AKT1, GSTM1, PLF, HBD, MIR144, MPO, APOB, RAPGEF5, AGT, THBS1, ANGPT2, MYH9, ICAM4, LCN2, ADRA1D, CXCL10, NT5E, IL18, PDE5A, IL10, MBTPS1, ADCY6, AGER, ADRB2, IL1A, PPBP, IGFBP3, PRKAR1A, TNFRSF1A, GSTP1, GCH1, VPS51, SCD5, SAR1A, ADAMTS13, COMT, FCGR3B, RUNX2, KDM1A, ATP2A2, ANTXR1, CD14, CAPN1, HES7, DECR1, CD59, CYP2C19, RBM45, CTLA4, CD38, TFPI, CPLANE1, PRDX2, LIN28A, NOD2, CDH23, PRRT2, UGGT1, CHD7, CAMKMT, KLF10, NLRP3, GALNT13, TIE1, TK2, APOA5, TLR2, CCR2, MIR454, TNFSF15, TALDO1, TACR1, KRT88P, ROS1, RPS19, RYR1, KRT90P, LOC107987479, SCN2A, HOPX, CCL5, CCL7, CX3CL1, MPIG6B, CBSL, SFTPD, SLC12A4, SLC14A1, SLCO1A2, SMPD1, SPG7, SPRR2A, CD24, LPCAT1, SLC35A2, TRIM21, TAC1, SPTBN1, NCF1, RIPPLY2, UGT2B7, PER2, MIR326, CBX3, ZPR1, MBD2, TRPA1, RSPH1, SPIN1, HPSE, SKA2, ZFYVE9, LIPG, GRAP2, DMRT2, MIR301A, MIR214, AHSA1, KAT5, VHLL, LINC01194, GDF15, APOBEC3B, TRIM13, LPCAT3, CEBPZ, NR1I3, PIEZO1, APLN, SMUG1, DIANPH, BEAN1, KEAP1, CPVL, MESP2, TRPV1, EOS, HBFQTL2, AIMP2, CXADRP1, AKAP1, BRAP, LOH19CR1, PLA2G6, PRRX2, NANOS1, AHSP, OR10A4, ICOS, IL37, HAVCR1, TNFSF14, SLC17A5, TNFRSF6B, POLDIP2, RNF19A, CLDN15, PROZ, LRSAM1, ABCA1, MOK, CLDN3, CYBB, CXADR, CTSK, CST3, MAPK14, CRYZ, CRP, CRK, COX8A, CD40LG, COL4A1, CCR4, CLCN7, CHM, CHIT1, CTSC, CDA, CD63, CD55, ACE, CYB5R3, DNASE1, FOXO3, FKBP4, FH, FES, FDPS, FCGR3A, FCGR2A, FAAH, ETFA, EPAS1, ELAVL2, ELANE, EGR1, S1PR1, ATN1, DRD3, DRD2, CD47, CD36, FOSB, AMBP, ARG1, ABCC6, FAS, APOE, APOA1, BIRC3, BIRC2, AMH, ALOX5, CD28, ALAS2, AKT2, ADORA2B, ADCY9, ADA, ACP3, ACP5, ACHE, ARR3, ASS1, ATP2B4, AVPR1A, CD19, CD6, CD1C, CD1B, CD1A, KRIT1, CBS, CASR, CASP3, CASP1, CALM3, CALM2, CALM1, BTK, BRCA1, BDNF, BAX, FOS, MTOR, PTX3, MYH2, P2RY6, OXCT1, OLR1, OAT, NOS1, NM, NHS, NGF, MUC1, LFNG, MST1R, MFGE8, MCL1, MAP6, SMAD2, SMAD1, LYZ, LTB, P4HB, PAPPA, PER1, PF4, PTH, PRNP, MAPK8, MAPK1, PRKCB, PRKCA, PPARG, PPARA, PON3, PON1, PLXNA2, PLG, PLA2G4A, PLA2G2A, PLA2G1B, SERPINA1, ABCB1, LGALS3, LDLR, FUCA2, GYPA, HLA-G, HLA-E, HLA-A, HFE, CFH, HEXA, SERPIND1, GZMM, GTF2I, LCAT, GSR, CXCL1, NR3C1, CBLIF, GH1, GAPDH, GAD1, ACKR1, HMGB1, HMGCR, HSP90AA1, ICAM1, LAMC2, KRT12, KLRC3, KCNN4, JUND, JUNB, JUN, ITGB2, ITGAL, ITGA4, INSIG1, IMPA1, IL17A, CXCR2, IL5, IL2, IGF1R, HBB-LCR

-
Microchimerism
Wikipedia
Postnatal tolerance to NIMAs [ edit ] NIMA-specific tolerance causes some interesting immunological phenotypes: sensitization to erythrocyte Rhesus factor (Rh) antigens is reduced among Rh- women born to Rh+ women, [26] long-term kidney allograft survival is improved in NIMA-matched donor-recipient sibling pairs, [27] or acuteness of bone marrow transplantation graft-versus-host disease is reduced, when recipients of donor stem cells are NIMA-matched. [28] Cross-fostering animal studies show that when postnatal NIMA exposure though breastfeeding is eliminated, survival of NIMA-matched allografts is reduced.
-
Male Infertility
Wikipedia
Thus, the diagnosis may be missed, leading to a risk of long-term complications. [21] In men, CD can reduce semen quality and cause immature secondary sex characteristics , hypogonadism and hyperprolactinaemia , which causes impotence and loss of libido . [22] The giving of gluten free diet and correction of deficient dietary elements can lead to a return of fertility. [21] [22] It is likely that an effective evaluation for infertility would best include assessment for underlying celiac disease, both in men and women. [23] Drugs , alcohol Strenuous riding ( bicycle riding , [24] horseback riding ) Medications, including those that affect spermatogenesis such as chemotherapy , anabolic steroids , cimetidine , spironolactone ; those that decrease FSH levels such as phenytoin ; those that decrease sperm motility such as sulfasalazine and nitrofurantoin Genetic abnormalities such as a Robertsonian translocation Tobacco smoking [ edit ] See also: Smoking and pregnancy There is increasing evidence that the harmful products of tobacco smoking may damage the testicles [25] and kill sperm, [26] [27] but their effect on male fertility is not clear. [28] Some governments require manufacturers to put warnings on packets.CFTR, NR5A1, AURKC, FSHB, ESR1, CYP1A1, MTHFR, LHCGR, AR, NOS3, POLG, MTR, MTRR, TP53, AHR, PON1, ACE, OGG1, SOD2, BCL2, PMFBP1, CYP17A1, NSUN7, ARMC2, GPX4, MDM2, DNAAF4, NANOS2, HOXD11, DROSHA, TSC22D3, ELOVL2, GNRH1, ENO1, STX2, TDRD7, KMT2D, CST8, NR1H4, SELENOP, CDC14A, ALDH2, LDHC, BAX, RAD23B, LHB, ENO4, CBL, TAS1R3, GNAT3, KIT, BSCL2, FAS, SPATA16, ARL2BP, FKBP6, CSNK2A2, ADAMTS16, SMAD1, AGFG1, CNOT7, TCTE1, CABYR, DAZ1, CYP19A1, USP9Y, CATSPER1, DAZ2, DDX3Y, SUN5, CATSPER2, TEX11, TSPY1, DAZ4, WT1, ADGRG2, DNAI2, DNAI1, SRY, PTPN11, DAZ3, RBMY1A1, HOXD13, VAMP7, GSTT1, POLR2F, MAP2K1, SOX10, SOX9, PRM1, GSTM1, TGFB1, MAP3K1, WWOX, AMHR2, AZF1, MORC4, DMRT3, TEX15, CLDN2, CTNS, PPP2R3C, DNAAF5, DAZL, USP26, STRC, BRAF, NR0B1, ZFPM2, GCM2, FCGR2A, GATA4, AMH, FSHR, BRD2, PRM2, SNRPN, HPGDS, ESR2, GSTP1, XRCC1, SLCO6A1, AGRP, SEPTIN12, GSTK1, H2BW1, ARTN, DNAH1, MLH3, STAG3, TEX101, QRICH2, DCAF17, BOLL, SEMG1, PIWIL2, THEG, DDX25, SPO11, MEST, PIWIL1, SHBG, NAT2, CAT, CSTF2T, CLOCK, HSPA4L, CRISP2, CLUAP1, TBC1D9, IL1B, IL1RN, IL6, TARDBP, TSPYL1, IL18, ADAMTS1, UBE2B, TDRD1, PICK1, SPEF2, IGF2, ERCC2, TNP1, CDY1B, WDR66, CGA, THRB, AGBL5, TTTY2, APOB, HSPA2, SOD1, TIMP2, CREM, ADAMTS5, GBA2, FANCM, TNF, AHRR, AGT, GGCT, CFAP44, DNMT1, KITLG, H19-ICR, MMP2, COMETT, MMP9, BGLAP, DNAH17, MSH5, DNMT3L, NFE2L2, GH1, BPY2, DPF3, HFE, CDY1, DEFB126, DNMT3B, MNS1, EGR4, VEGFA, VIP, HLA-A, CYP2B6, ABCB1, YBX2, MIR34B, BRDT, BRCA2, CFAP69, CASP9, CFAP43, GGNBP2, SPATA9, ACSBG2, CLC, SLC25A31, CETN2, CDC25A, SPAG16, MAGEB4, CRK, SPATA20, SEMA5B, CYP2D6, DDX3X, ALKBH5, DDX4, RNF216, TAF7L, MOV10L1, DEFB1, CYP1B1, CMPK1, OAZ3, AZIN1, VPS54, PHF7, HOOK1, NME8, PARPBP, MTPAP, CLEC7A, EPPIN, CPEB1, COMT, PERP, LGR6, NCOA5, RPTOR, TTC29, CRP, RNF220, CRYGD, PRDM9, FAM20C, LRRC8A, MAPK14, CST3, MEG3, BRCA1, SLC26A8, TSSK1B, NANOS3, MIR10A, GOLGA2P3Y, ACTB, PICSAR, DNAJB13, PARP1, BMP8A, DNAAF3, H1-7, MIR145, SLC25A5, KLHL10, TUSC1, FBXO43, RNF212, EMC10, IZUMO1, LAMA1, MIR125B2, MIR196A2, KATNAL1, MIR486-1, SPGF2, HOTTIP, TSPY10, IZUMO3, TSPY3, GMNC, SPATA31A1, RAD21L1, MIR509-1, MIR210, MIR525, MIR383, BPY2C, BPY2B, PRY2, PGAM4, MIR93, MIR320A, TSSK4, NPHP4, IS1, NLRP3, TBC1D20, ATP2B1, AK7, CPXM2, CFAP70, ATP2B4, BDNF, CCDC151, SAT2, CFAP65, PYGO2, FATE1, PLCZ1, HSFY1, CCDC62, GOLGA2P2Y, CCDC115, BMPR1B, CMPK2, ATM, PRSS37, ARNTL, PXT1, GPRC6A, LRWD1, TDRD6, TYSND1, ANXA5, APEX1, GALNTL5, APOE, PATE1, HSFY2, KLK3, CMTM4, PIWIL4, PSMA8, RSS, RPL10L, DMRT1, RNF19A, PDE11A, HSPA1B, SOD3, HSPB1, SMN2, SMN1, SLC22A5, SLCO2A1, SLC19A1, SLC1A1, HTC2, SET, IGF1, RPL10, RNF4, IGFALS, IL1A, RAG1, PRPS2, SOX3, HSPA1A, ASAP1, SOX11, XPA, VDAC3, VDAC2, USF1, TXN, HLA-B, HLA-DQB1, NR2E1, TGFB3, HMOX1, TERT, TEP1, DYNLT1, HRG, SULT2A1, HSF1, HSF2, PROS1, IL11, MAPK1, PRKDC, OXTR, KRT18, ODF1, NRF1, NPR2, STMN1, NOS2, NOS1, LEP, LEPR, LIG4, MTHFD1, MSH2, MRC1, MPG, MMP7, MLH1, REG3A, PCBD1, PDHA2, PMS2, SRGN, PRB3, PPP1CC, INHA, POMC, INSL3, KDR, PLAU, PDZK1, PLAG1, PIP, PIK3CG, PIK3CD, PIK3CB, PIK3CA, PGR, HIF1A, XRCC3, AIMP2, KCNQ1OT1, MKRN2, ERCC1, ATP6V0A2, ERCC4, SIRT1, DICER1, PUM2, SLC9A8, ACSL6, AGTPBP1, CEP131, CLCA4, TUSC2, PDAP1, PARK7, RABL2A, RABL2B, TSSK1A, PRDX5, POC1A, DNASE1, SYCP3, PSAT1, DMWD, DNAH5, DNAH9, SETD2, POLL, RBMXL2, LIPE, IL37, DKKL1, PELP1, DNMT3A, SLC26A3, POLDIP2, E2F1, SOX30, PAPOLA, GSTM2, GADD45G, PRC1, GOLGA2, HAP1, SNURF, CCNA1, ASAP2, AKAP4, BECN1, EIF4G3, NR3C1, TP63, ACP3, ELP1, RANBP3, PPM1D, PDIA3, STK24, RGN, SLC16A7, ZMYM3, FOXO3, MRPS30, FKBP4, AHSA1, GNLY, CIB1, FOXO1, DNM1L, GAS6, GDNF, IFT140, UTP14C, PRDX6, NPEPPS, GRAP2, ADIPOQ, GBA, LOC110408762
-
Emerging Infectious Disease
Wikipedia
In response, the Coalition for Epidemic Preparedness Innovation was launched at the World Economic Forum in 2017 with the objective of accelerating the development of vaccines against emerging infectious diseases to be able to offer them to affected populations during outbreaks. [27] CEPI promotes the idea that a proactive approach is required to "create a world in which epidemics are no longer a threat to humanity". [28] Classification [ edit ] One way to classify emerging infections diseases is by time and how humans were involved in the emergence: [29] Newly emerging infectious diseases – diseases that were not previously described in humans, such as HIV/AIDS Re-emerging infectious diseases – diseases that have spread to new places or which previous treatments no longer control, such as methicillin-resistant Staphylococcus aureus Deliberately emerging infectious diseases – diseases created by humans for bioterrorism Accidentally emerging infectious diseases – diseases created or spread unintentionally by humans, such as vaccine-derived poliovirus Contributing factors [ edit ] The 1992 IOM report [23] distinguished 6 factors contributing to emergence of new diseases (Microbial adaptation and change; Economic development and land use; Human demographics and behavior; International travel and commerce; Technology and industry; Breakdown of public health measures) which were extended to 13 factors in the 2003 report [25] (Chapter 3 of the report detailing each of them) Microbial adaptation and change Human susceptibility to infection Climate and weather Changing ecosystems Human demographics and behavior Economic development and land use International travel and commerce Technology and industry Breakdown of public health measures Poverty and social inequality War and famine Lack of political will Intent to harm Their classification serves as a basis for many others. ... CS1 maint: others ( link ) ^ "Global outbreak alert and response" (PDF) . WHO . Geneva, Switzerland. 26–28 April 2000. hdl : 10665/66750 . Retrieved 10 September 2020 . ^ "A brief history of vaccines and how they changed the world" . ... Archived from the original on 18 April 2020. ^ "Blueprint for R&D preparedness and response to public health emergencies due to highly infectious pathogens" . www.who.int . Archived from the original on 28 April 2020. ^ Woolhouse, Mark; Gaunt, Eleanor (January 2007).

-
Alcohol And Cancer
Wikipedia
The local cytotoxic effect of ethanol may also explain the known synergistic effect of alcohol and tobacco use on the risk of these cancers. [21] Epithelial-mesenchymal transition [ edit ] A study found that alcohol stimulates the epithelial-mesenchymal transition (EMT), in which ordinary cancer cells change into a more aggressive form and begin to spread throughout the body. [22] [23] Effect of alcohol on the progress of cancer when established [ edit ] A study of the influence of alcohol intake on tumor growth of hepatocellular carcinoma (HCC) in patients with type C cirrhosis , found that alcohol influenced tumor volume doubling time (TVDT). [24] A study of chick embryos suggests that alcohol stimulates their tumor growth by fueling the production of a growth factor that stimulates blood vessel development in tumors. [25] A 2006 study in mice showed moderate drinking resulted in larger and stronger tumors via a process known as angiogenesis . [26] [27] A study where high amounts of alcohol were given to mice suggests that it accelerates their cancer growth by speeding up the loss of body fat and depressing immune activity. [28] Genetic variation and cancer risk [ edit ] A study found that "the ADH1C *1 allele and genotype ADH1C*1/1 were significantly more frequent in patients with alcohol-related cancers…" [13] A European study has found two gene variants which offer "significant" protection against mouth and throat cancers. [29] Alcohol is a known porphyrinogenic chemical. ... Centre for Addiction and Mental Health , Science Daily . 28 September 2007 . Retrieved 29 June 2009 . ^ Warnakulasuriya S, Parkkila S, Nagao T, et al. (2007).

-
Mouth Ulcer
Wikipedia
. ^ a b "Balsam of Peru contact allergy" . Dermnetnz.org. 28 December 2013 . Retrieved 5 March 2014 . ^ a b Gottfried Schmalz; Dorthe Arenholt Bindslev (2008).EDN1, LEP, STAT4, IL10, TAP2, CRLF1, IL19, CRB1, TRIM31, EHMT2, IKZF1, TCIRG1, MAPKAPK2, FAS, KLRC4, IL20, TNXB, TNFAIP3, TLR4, TAP1, SRP54, SPP1, C1QA, SCHIP1, ERAP1, PTPRC, PSORS1C2, IL12A-AS1, MUC22, ARL17B, IQCJ-SCHIP1, SPATA48, LINC01100, GIMAP6, UBAC2, NSMCE2, PSORS1C1, LZTFL1, IL23R, SLC46A1, ZNRD1ASP, GSDMD, GTDC1, DCLRE1C, NOD2, IFT80, PGPEP1, RELA, RREB1, PSMB9, IL12RB1, IL7R, IFNGR1, HLA-J, HLA-DQA2, HLA-DPB1, HLA-DPA1, HLA-B, HLA-A, GFI1, SLC37A4, ELANE, CYP21A2, CCR1, CDSN, CAT, C4A, C1R, IL12A, IRF8, IRAK1, LTF, PPP5C, PDE4D, NOTCH4, NFKB1, MEFV, LYZ, LINC02009, CRP, TNF, VEGFA, IL2, CSF3, ENO1, ITGAM, IL2RA, NGF, SOCS3, MIR223, MTHFR, PLAAT4, FCGR2A, RNPC3, SOCS1, GEM, ISG20, HGF, KIR3DL1, IFIH1, LGALS1, IL21, TPMT, GYPA

-
Temporal Lobe Epilepsy
Wikipedia
However, although the virus is found in temporal lobe tissue at surgery for TLE, it has not been recognised as a major factor in febrile seizures or TLE. [26] [27] [28] Reelin [ edit ] Dispersion of the granule cell layer in the hippocampal dentate gyrus is occasionally seen in temporal lobe epilepsy and has been linked to the downregulation of reelin , a protein that normally keeps the layer compact by containing neuronal migration . ... "The recurrent mossy fiber pathway of the epileptic brain". Neurochemical Research . 28 (11): 1649–1658. doi : 10.1023/a:1026004904199 .GRM1, NPY, GRM5, SLC12A5, VDR, P2RX7, KDR, SLC12A2, TRPV1, SLIT2, SLC1A1, NPY2R, GRM2, TEK, BDKRB1, BDKRB2, COX3, P2RX4, VEGFA, KCNC4, CNR1, GRM4, GRM3, ABCB1, MTOR, NTRK2, RGMA, NSF, NOS1, CXCR4, GLUL, HCN1, ADK, AGT, DTNBP1, FYN, GLUD1, GRIK5, PRICKLE1, DLG4, KCNA1, SHH, CYFIP1, CABP1, MAP2, MBP, VDAC2, SLC6A1, PTPRZ1, ACTB, ADD1, DBN1, CDC42, CRH, CACNA1A, AK2, CRHBP, AVP, APOE, LGI1, GABBR1, BDNF, IL1B, SLC6A4, SLC1A2, MIR146A, MIR155, PDYN, PVALB, AQP4, STIN2-VNTR, PRNP, SMUG1, TNF, RELN, TLR4, HTR1A, GRIA2, TBC1D9, GRIN2A, CPA6, GFAP, GRIN1, GPHN, TSPO, SST, SOD1, HSPA4, APP, OPRM1, SCN2A, HTR2A, AIF1, AZGP1, IL1RN, BCL2, JRK, ACE, GAL, KCNJ10, SCN1A, CALB1, S100B, ZFYVE9, CNTNAP2, MAOA, MAPK8, CASP3, MMP9, ADAM10, KLK8, NFE2L2, TRPV4, SCN8A, MIR134, MAPK14, ENO2, MIR23A, F2R, CALHM1, MIR21, DNMT1, GRIN2B, GABRB3, DNMT3A, MIRLET7B, CFH, DCX, FLT4, GRIA1, ADIPOQ, MIR34A, MIR139, TNFRSF10A, HAP1, GNA14, APOBEC1, DEPDC5, MIR204, KEAP1, GRAP2, GABBR2, CDYL, MIR221, GAB2, BIN1, TNFSF10, MIR222, DUSP26, MIR331, IRS2, TNFRSF1A, TP53, LOC110806262, TXNRD1, ATP1A2, AQP9, GATD3B, PGR-AS1, VEGFC, MICA, FTX, MIR1260A, MIR1183, C20orf181, AIMP2, GLRA3, MLRL, GATD3A, DOC2A, SEMA7A, CCR2, MIR451A, CASP8AP2, PDE5A, MIRLET7C, TUBB3, MIR132, KCNMB4, SLC46A1, KCNH7, ZDHHC8, UBQLN1, ATL1, WNT3A, SHANK3, SUCO, PEX5L, RBFOX1, PAG1, RETN, EFCAB2, AGTR2, RTN4, SNX25, TLN2, SOX7, SEMA6A, DHX40, SRR, MICAL1, TNFRSF13C, GLS2, RNU1-1, OPN5, WNK3, FAM3C, CXCL13, AHSA1, TNFSF13B, PDE10A, NWD1, NEAT1, ACOT7, NLRP1, MAPK8IP3, SPAG8, AKT1, VPS13A, SMG6, ADRA2A, PADI4, RSS, TPH2, PANX1, RNF19A, POLDIP2, DROSHA, DBP, TLR2, NRG1, CYBB, CTSD, GRIA3, GRN, GRIK1, GRIK2, CTSB, NR3C1, CSF2, CRP, CRK, GSK3B, HDAC2, HIF1A, CDX2, HRC, HES1, HSP90AB1, HTC2, ICAM1, IGF1, IL1A, IL2, IL7, CXCR2, IL13, IL17A, IL18, GLP1R, GJA1, GHRH, GAPDH, DECR1, DFFB, TIMM8A, DNM1, DNAH8, DPYSL2, DSCAM, EGR1, EGR2, EIF2S1, EIF4EBP1, EPHA4, EPHX2, ESR1, FEB1, FEB2, FHL2, FOXO3, FOLR1, DAPK1, DAP, GABRA1, GABRA2, GABRA5, GABRB2, GAD1, GAD2, IRS1, KCND2, THOP1, SCNN1D, MAPK1, MAPK10, PSEN2, PTGS2, PTPN11, CXCR5, REN, UPF1, RRBP1, S100A1, SC5D, SCN1B, SCN7A, CCL3, KCNE1, CCL4, CXCL12, SELP, SELENOW, SH3GL2, HCN2, SLC6A9, SLC16A1, SMS, SOX2, SPAST, SRF, SSTR2, PRKG2, PLD2, PLD1, PLAT, KCNJ9, KCNQ3, KLK1, KLKB1, KNG1, LAMC2, LEP, LETM1, SMAD3, CCK, MAPT, MDM2, MECP2, MGAT1, MMP3, MPO, MST1, CASP1, MYD88, CAST, NPY1R, C3, SERPING1, OPRL1, BTN1A1, PRDX1, SERPINE1, LINC02605

-
Late Talker
Wikipedia
The assessments carried out on the child needs to be appropriate for the child's cultural setting. [26] Tests cannot be translated as this affects the data and can result in a child being misdiagnosed. [26] For children who speak more than one language, assessments need to be catered to that. [2] A standardized test is not enough to diagnose a child who is bilingual . [2] Bilingual children need to be assessed using a combination of ethnographic interviewing, language sampling, dynamic assessment, standardised tests and observation techniques to be accurately diagnosed as a late talker. [2] Treatment [ edit ] The earlier interventions are put in place to help a toddler overcome LLE, the better the outcome. [9] Language interventions (with the help of speech pathologists) are needed, so late talkers eventually catch-up. [2] Some common approaches are monitoring, indirect and direct language stimulation. [10] Late talkers struggle with learning vocabulary and phonological acquisition. [6] Targeting vocabulary and increasing their vocabulary bank, will simultaneously improve their phonological development . [6] When deciding which approach to take in treating a toddler, cultural background needs to be taken into consideration. [10] Some types of intervention may work for some cultures, but may not work nor be appropriate for others. [15] Language intervention [ edit ] Late talkers can be treated with a variety of language intervention methods. [28] The earlier a child is diagnosed and treated the better his language skills will develop when growing up. [29] General language stimulation [ edit ] General Language Stimulation involves providing the child with an environment that is full of language stimulation. [11] [12] This includes giving the child the opportunity to participate in reading books, playing, cooking and other everyday activities the child is interested in. [11] The key to this intervention is to follow the late talker's lead. [11] Once a child is interested in a specific object the parent or carer will then take part in parallel talk, that is, talking about the object rather than directly modelling the word. [11] The parent or carer is then required to repeat the child's utterance , regardless of how incorrect it is, and complement this with semantic and grammatical detail. [11] Focused language stimulation [ edit ] Focused language stimulation requires the parent or carer to have a list of goal words for the child to learn and produce. [11] [13] The average number of target words is ten, but this will vary from child to child. [15] [11] The parent or carer will then have to allow the child to be exposed to the target language as much as possible. [11] The adult has to produce the target language in a meaningful and functional context such as, in a sentence or question form. [13] The child is then prompted (not instructed) to repeat the target word. [11] If the target word is produced incorrectly, the parent follows with a recast . [11] Once the child has learnt these words the adult replaces these with new ones and the process is repeated. [15] Milieu teaching [ edit ] Milieu Teaching involves changing the child's environment to give him as many opportunities to talk and produce the target language. [11] [30] In this intervention method it is necessary to have a set of language goals for the child to achieve. [11] Incorrect production of target language follows by the adult modelling the word for the child to imitate. [11] [30] Correct production of target language follows by the adult providing a recast. [11] [30] Culture and treatment [ edit ] Culture diversity is a considerable factor in choosing the right type of intervention for a child. [31] Speech pathologist are the ones responsible for choosing a treatment that is culturally appropriate for the child and his family. [15] Treatments such as General Language Stimulation, Focused language stimulation and Milieu Teaching are designed appropriately to meet the needs of the majority in the United States. [15] These methods are adapted to meet the needs of other cultures in the community for the child to have a higher success rate. [15] The nature and context of social interactions is observed when modifying a standard treatment to meet the norms of a child's culture and background. [15] For example, in some cultures it is not common for parents to be so involved in play with their child. [31] [15] The treatment is then adapted for other family members (siblings, cousins, other peers) to deliver the intervention. [15] The location where these treatments are usually provided is the family home.
-
Gastroenteritis
Wikipedia
The rotavirus vaccine is recommended as a prevention for children. [2] [10] Treatment involves getting enough fluids. [2] For mild or moderate cases, this can typically be achieved by drinking oral rehydration solution (a combination of water, salts and sugar). [2] In those who are breastfed, continued breastfeeding is recommended. [2] For more severe cases, intravenous fluids may be needed. [2] Fluids may also be given by a nasogastric tube . [13] Zinc supplementation is recommended in children. [2] Antibiotics are generally not needed. [14] However, antibiotics are recommended for young children with a fever and bloody diarrhea. [1] In 2015, there were two billion cases of gastroenteritis, resulting in 1.3 million deaths globally. [6] [7] Children and those in the developing world are affected the most. [15] In 2011, there were about 1.7 billion cases, resulting in about 700,000 deaths of children under the age of five. [16] In the developing world, children less than two years of age frequently get six or more infections a year. [17] It is less common in adults, partly due to the development of immunity . [18] Contents 1 Signs and symptoms 2 Cause 2.1 Viral 2.2 Bacterial 2.3 Parasitic 2.4 Transmission 2.5 Non-infectious 3 Pathophysiology 4 Diagnosis 4.1 Dehydration 4.2 Differential diagnosis 5 Prevention 5.1 Lifestyle 5.2 Vaccination 6 Management 6.1 Rehydration 6.2 Dietary 6.3 Antiemetics 6.4 Antibiotics 6.5 Antimotility agents 7 Epidemiology 8 History 9 Society and culture 10 Research 11 Other animals 12 References 12.1 Notes 13 External links Signs and symptoms [ edit ] Bristol stool chart Gastroenteritis usually involves both diarrhea and vomiting . [18] Sometimes, only one or the other is present. [1] This may be accompanied by abdominal cramps. [1] Signs and symptoms usually begin 12–72 hours after contracting the infectious agent. [15] If due to a virus, the condition usually resolves within one week. [18] Some viral infections also involve fever , fatigue, headache and muscle pain . [18] If the stool is bloody , the cause is less likely to be viral [18] and more likely to be bacterial. [19] Some bacterial infections cause severe abdominal pain and may persist for several weeks. [19] Children infected with rotavirus usually make a full recovery within three to eight days. [20] However, in poor countries treatment for severe infections is often out of reach and persistent diarrhea is common. [21] Dehydration is a common complication of diarrhea . [22] Severe dehydration in children may be recognized if the skin color and position returns slowly when pressed. [23] This is called "prolonged capillary refill " and "poor skin turgor ". [23] Abnormal breathing is another sign of severe dehydration. [23] Repeat infections are typically seen in areas with poor sanitation, and malnutrition . [15] Stunted growth and long-term cognitive delays can result. [17] Reactive arthritis occurs in 1% of people following infections with Campylobacter species. [19] Guillain–Barré syndrome occurs in 0.1%. [19] Hemolytic uremic syndrome (HUS) may occur due to infection with Shiga toxin -producing Escherichia coli or Shigella species. [24] HUS causes low platelet counts , poor kidney function , and low red blood cell count (due to their breakdown) . [24] Children are more predisposed to getting HUS than adults. [17] Some viral infections may produce benign infantile seizures . [1] Cause [ edit ] Viruses (particularly rotavirus ) and the bacteria Escherichia coli and Campylobacter species are the primary causes of gastroenteritis. [15] [25] There are, however, many other infectious agents that can cause this syndrome including parasites and fungus . [17] [4] Non-infectious causes are seen on occasion, but they are less likely than a viral or bacterial cause. [1] Risk of infection is higher in children due to their lack of immunity . [1] Children are also at higher risk because they are less likely to practice good hygiene habits. [1] Children living in areas without easy access to water and soap are especially vulnerable. [1] Viral [ edit ] Rotavirus , norovirus , adenovirus , and astrovirus are known to cause viral gastroenteritis . [18] [26] Rotavirus is the most common cause of gastroenteritis in children, [25] and produces similar rates in both the developed and developing world . [20] Viruses cause about 70% of episodes of infectious diarrhea in the pediatric age group. [13] Rotavirus is a less common cause in adults due to acquired immunity. [27] Norovirus is the cause in about 18% of all cases. [28] Generally speaking, viral gastroenteritis accounts for 21%-40% of the cases of infectious diarrhea in developed countries. [29] Norovirus is the leading cause of gastroenteritis among adults in America accounting for about 90% of viral gastroenteritis outbreaks. [18] These localized epidemics typically occur when groups of people spend time in close physical proximity to each other, such as on cruise ships , [18] in hospitals, and in restaurants. [1] People may remain infectious even after their diarrhea has ended. [18] Norovirus is the cause of about 10% of cases in children. [1] Bacterial [ edit ] Salmonella enterica serovar Typhimurium (ATCC 14028) as seen with a microscope at 1000 fold magnification and following Gram staining. ... Archived from the original on 2014-10-28. ^ Allen SJ, Martinez EG, Gregorio GV, Dans LF (2010). ... Archived from the original on 2015-11-28. ^ World Health Organization. "Enterotoxigenic Escherichia coli (ETEC)" . ... Archived from the original on 2015-11-28. ^ Zimmerman, Jeffrey; Karriker, Locke; Ramirez, Alejandro; Kent Schwartz; Gregory Stevenson (15 May 2012). ... ISBN 978-0-8138-2267-9 . Archived from the original on 28 November 2015. Notes [ edit ] Dolin, Raphael; Mandell, Gerald L.; Bennett, John E., eds. (2010).F2RL1, ANPEP, CDK2AP1, PRSS57, CAT, AHI1, NCKIPSD, BCAR3, IFNG, MAPK1, RTN2, AIMP2, RIDA, GRAP2, IFNA13, AHSA1, RNF19A, POLDIP2, PRRT2, IFNB1, SLC5A2, IFNA1, EGFR, CRK, MAPK14, ERICD, IL17A, PABPC1, PDP1, CDSN, IL22, SIGLEC8, LAMP3, ACAD8, CPE, IRF3, CFH, ATF6, CRP, IL1RAP, SH2D3C, EIF2AK3, CDC42, SARS2, MARCHF1, ATG16L1, CCDC88A, ENAH, GORASP1, NBEAL1, WNK1, ATP4A, PGLYRP3, ASZ1, ZBTB46, PLB1, IRGM, ATP12A, MIR222, DDX1, IL6, PLA2G6, RPL10, KRT10, LPA, LSAMP, MME, NM, CCN3, PLA2G1B, PLA2G2A, PLXNA1, CTSA, CBLIF, MAPK8, RB1, RELA, FUT2, ST8SIA2, SARS1, SCN1A, SCN1B, APOH, SLC5A5, SPI1, SYT1, TFRC, TNF, VTN, XBP1, YWHAZ, ERN1, IFN1@, STX2

-
Influenza Pandemic
Wikipedia
The 1889–1890 and 1918–1919 flu pandemics each came in three or four waves of increasing lethality. [27] But within a wave, mortality was greater at the beginning of the wave. [28] Variable mortality [ edit ] Mortality varies widely in a pandemic. ... The first problem is this: seasonal influenza vaccines require a single injection of 15 μg haemagluttinin in order to give protection; H5 seems to evoke only a weak immune response and a large multicentre trial found that two injections of 90 µg H5 given 28 days apart provided protection in only 54% of people. [124] Even if it is considered that 54% is an acceptable level of protection, the world is currently capable of producing only 900 million doses at a strength of 15 μg (assuming that all production were immediately converted to manufacturing H5 vaccine); if two injections of 90 μg are needed then this capacity drops to only 70 million. [125] Trials using adjuvants such as alum , AS03 , AS04 or MF59 to try and lower the dose of vaccine are urgently needed.

-
Wallerian Degeneration
Wikipedia
Wallerian degeneration slow [ edit ] Mice belonging to the strain C57BL/ Wld s have delayed Wallerian degeneration, [28] and, thus, allow for the study of the roles of various cell types and the underlying cellular and molecular processes.NMNAT1, CCAR2, SIRT1, UBE4B, RXRA, TIMP3, TIMP2, TGFB2, TGFB1, SRSF3, ERBB2, ERBB3, NPY1R, NF1, NEFL, NEFH, NEFM, MAG, IL18, FCGR2A, PLA2G4A
















