Type II pseudohypoaldosteronism was the designation used by Schambelan et al. (1981) for this syndrome of chronic mineralocorticoid-resistant hyperkalemia with hypertension. ... Gordon et al. (1988) described an Australian family with 6 affected members in 2 generations and referred to the condition as Gordon syndrome or hyporeninemic hypoaldosteronism. (Gordon (1995) stated that de Wardener first termed it Gordon syndrome.) Studies suggested dysregulation of atrial natriuretic factor (ANP; 108780). ... At the other end of the age range were the infants with neonatal onset of Gordon syndrome described by Gereda et al. (1996). Two sisters developed Gordon syndrome within the first 2 weeks of life.
Description Familial hyperkalemic hypertension, also known as type II pseudohypoaldosteronism (PHAII) or Gordon syndrome, is a rare autosomal dominant disease in which a net positive sodium ion balance is associated with renal potassium ion retention, resulting in hypertension, hyperkalemia, and hyperchloremic metabolic acidosis (summary by Louis-Dit-Picard et al., 2012).
Chlorothiazide administration promptly corrected all features. The syndrome affected 7 members of 3 generations with instances of male-to-male transmission, thus indicating autosomal dominant inheritance.
Patients do not present renal failure. Spitzer-Weinstein syndrome is believed to be the early presentation of Pseudohypoaldosteronism type 2 (PHA2) with hypertension associated with other clinical findings such as short stature, muscle weakness, periodic paralysis and dental abnormalities.
Summary Clinical characteristics. Pseudohypoaldosteronism type II (PHAII) is characterized by hyperkalemia despite normal glomerular filtration rate (GFR) and frequently by hypertension. Other associated findings in both children and adults include hyperchloremia, metabolic acidosis, and suppressed plasma renin levels. Aldosterone levels are variable, but are relatively low given the degree of hyperkalemia (elevated serum potassium is a potent stimulus for aldosterone secretion). Hypercalciuria is well described. Diagnosis/testing. The diagnosis of PHAII is established in a proband: With hyperkalemia (in the setting of normal glomerular filtration), hypertension, metabolic acidosis, hyperchloremia, and suppressed plasma renin levels; AND/OR By the identification of a heterozygous pathogenic variant in CUL3 , WNK1 , or WNK4 or a heterozygous pathogenic variant or biallelic pathogenic variants in KLHL3 . Management. Treatment of manifestations: Electrolyte and blood pressure abnormalities of PHAII in children and adults are often corrected with thiazide diuretics.
A number sign (#) is used with this entry because pseudohypoaldosteronism type IIE (PHA2E) is caused by heterozygous mutation in the CUL3 gene (603136) on chromosome 2q36. For a phenotypic description and a discussion of genetic heterogeneity of pseudohypoaldosteronism type II, see PHA2A (145260). Clinical Features Boyden et al. (2012) studied a cohort of 52 PHAII kindreds, including 126 affected subjects with renal hyperkalemia and otherwise normal renal function; hypertension and acidosis were present in 71% and 82%, respectively. They detected 21 affected individuals from 17 kindreds with mutation in the CUL3 gene. The mean age at diagnosis or referral was 9 +/- 6 years, mean potassium was 7.5 +/- 0.9, and mean bicarbonate was 15.5 +/- 2.0.
Psuedohypoaldosteronism type 2 is an inborn error of metabolism. It is characterized by high blood pressure, high levels of potassium in the body, and metabolic acidosis . It is caused by mutations in the WNK1 or WNK4 gene. Treatment may involve dietary restriction of sodium and hydrochlorothiazide .
The diagnosis of AIP is made in the appropriate clinical setting in a patient who has a clinical presentation compatible with acute respiratory distress syndrome (ARDS; see this term) but without a clear etiology.
Clinical Features Say et al. (1971) described coxa vara in 5 members of 3 generations of a family in Cyprus. The proband was a 4-year-old boy who was examined for a 'waddling gait.' Physical examination revealed no abnormality except restriction of abduction of the hips. X-rays showed the femoral neck shaft angle to be 110 degrees. No other skeletal abnormalities were found. The proband's father and paternal grandmother showed the same abnormality.
Other names to describe mitral valve prolapse include: Barlow syndrome Billowing mitral valve syndrome Click-murmur syndrome Floppy valve syndrome Mitral prolapse Myxomatous mitral valve disease Symptoms Signs and symptoms of mitral valve prolapse are due to the amount of blood leaking backward through the valve. ... Mitral valve prolapse can occur in families (be inherited) and may be linked to several other conditions, including: Ebstein anomaly Ehlers-Danlos syndrome Graves' disease Marfan syndrome Muscular dystrophy Scoliosis Complications Potential complications of mitral valve prolapse may include: Mitral valve regurgitation.
Navicular syndrome , often called navicular disease , is a syndrome of lameness problems in horses . ... Contributing factors [ edit ] Conformation [ edit ] Certain conformational defects may contribute to navicular syndrome, especially defects that promote concussion. ... Prognosis [ edit ] The prognosis for a horse with navicular syndrome is guarded. Many times the horse does not return to its former level of competition. Others are retired. Eventually all horses with the syndrome will need to lessen the strenuousness of their work, but with proper management, a horse with navicular syndrome can remain useful for some time. ... Retrieved 2020-10-08 . ^ "Special Feature | Podotrochlosis: 'Navicular Syndrome' is No Longer the End of the Road for Horses" .
A number sign (#) is used with this entry because of evidence that Okur-Chung neurodevelopmental syndrome (OCNDS) is caused by heterozygous mutation in the CSNK2A1 gene (115440) on chromosome 20p13. Description Okur-Chung neurodevelopmental syndrome is an autosomal dominant disorder characterized by delayed psychomotor development, intellectual disability with poor speech, behavioral abnormalities, cortical malformations in some patients, and variable dysmorphic facial features. ... Clinical Features Okur et al. (2016) reported 5 unrelated girls, ranging in age from 2 to 13 years, with a syndromic neurodevelopmental disorder. Common features included developmental delay, intellectual disability with behavioral problems and delayed speech, hypotonia, and gastrointestinal problems such as dysphagia, gastric reflux, or constipation. ... The authors noted that some of these findings were suggestive of Kleefstra syndrome (610253), Coffin-Siris syndrome (135900), or Rubinstein-Taybi syndrome (180849).
Spontaneous pneumothorax is a complication of certain heritable disorders of connective tissue, particularly the Marfan syndrome (154700) and the Ehlers-Danlos syndrome (see, e.g., 130000). ... Although one of them was said to have had the Walker-Murdoch wrist sign characteristic of the Marfan syndrome (Walker and Murdoch, 1970), he showed no evidence of ectopia lentis or aortic root and mitral valve abnormalities on appropriate studies. ... Examination showed no signs of Marfan syndrome, Ehlers-Danlos syndrome, or other connective tissue disorders. ... Gunji et al. (2007) suggested that isolated pulmonary cysts and pneumothorax may be a milder form of BHD syndrome and that patients should be monitored for renal or skin lesions. ... Because of the strong association between primary spontaneous pneumothorax and the Birt-Hogg-Dube syndrome, Painter et al. (2005) suggested that patients with familial PSP may be at greater risk of developing renal cancer.
Reflex tachycardia and/or respiratory or circulatory compromise may be observed. Other syndromes (e.g. Birt-Hogg-Dube, Marfan or Ehlers-Danlos syndromes) may be associated.
In addition, several genetic disorders have been linked to primary spontaneous pneumothorax, including Marfan syndrome , homocystinuria , and Birt-Hogg-Dube syndrome .
Primary spontaneous pneumothorax is an abnormal accumulation of air in the space between the lungs and the chest cavity (called the pleural space) that can result in the partial or complete collapse of a lung. This type of pneumothorax is described as primary because it occurs in the absence of lung disease such as emphysema. Spontaneous means the pneumothorax was not caused by an injury such as a rib fracture. Primary spontaneous pneumothorax is likely due to the formation of small sacs of air (blebs) in lung tissue that rupture, causing air to leak into the pleural space. Air in the pleural space creates pressure on the lung and can lead to its collapse.
A number sign (#) is used with this entry because of evidence that bone marrow failure syndrome-3 (BMFS3) is caused by homozygous mutation in the DNAJC21 gene (617048) on chromosome 5p13. Description Bone marrow failure syndrome-3 is an autosomal recessive disorder characterized by onset of pancytopenia in early childhood. ... BMFS3 has a distinct phenotype and may include features that overlap with Shwachman-Diamond syndrome (SDS1; 260400), such as pancreatic insufficiency and short stature, and with dyskeratosis congenita (see, e.g., DKCA1, 127550), such as dental and hair abnormalities and shortened telomeres. ... Clinical Features Tummala et al. (2016) reported 4 unrelated children with a bone marrow failure syndrome. All children were born of consanguineous parents, and none had a family history of the disorder. ... Dhanraj et al. (2017) reported 4 patients from 3 unrelated families with a bone marrow failure syndrome suggestive of Shwachman-Diamond syndrome.
A number sign (#) is used with this entry because it represents a contiguous gene deletion syndrome. Description The interstitial 16q22 deletion syndrome is a multiple congenital anomaly disorder associated with failure to thrive in infancy, poor growth, delayed psychomotor development, hypotonia, and dysmorphic features, including large anterior fontanel, high forehead, diastasis of the cranial sutures, broad nasal bridge, hypertelorism, low-set abnormal ears, and short neck. The phenotypic features and deletion sizes are variable, but deletion of 16q22 appears to be critical for manifestations of the syndrome (summary by Fujiwara et al., 1992). ... The findings suggested that 1 feature of the 16q22 deletion syndrome, large fontanels, may be due to haploinsufficiency of CBFB. ... INHERITANCE - Isolated cases GROWTH Height - Low birth length Weight - Low birth weight Other - Failure to thrive - Postnatal growth retardation HEAD & NECK Head - High forehead - Frontal bossing Face - Micrognathia Ears - Low-set ears - Posteriorly rotated ears - Dysplastic ears Eyes - Hypertelorism - Epicanthal folds - Upslanting palpebral fissures - Short palpebral fissures Nose - Broad flat nasal bridge Mouth - High-arched palate Neck - Short neck CHEST External Features - Narrow thorax Breasts - Widely spaced nipples ABDOMEN Gastrointestinal - Poor suck SKELETAL Skull - Large anterior fontanel - Diastasis of cranial sutures - Wormian bones Hands - Flexed fingers Feet - Broad first toe NEUROLOGIC Central Nervous System - Hypotonia - Delayed psychomotor development MISCELLANEOUS - Contiguous gene deletion syndrome MOLECULAR BASIS - A contiguous gene syndrome caused by deletion of chromosome 16q22 including the CBFB gene ( 121360 ) ▲ Close
Over time, additional clinical features appear: Poor growth Early (often severe) osteoporosis Subclinical or overt pulmonary involvement Renal involvement Hemophagocytic lymphohistiocytosis/macrophagic activation syndrome Biochemical laboratory features Elevated plasma ammonia after a protein-rich meal. ... Renal tubular acidosis or findings consistent with reduced phosphate reabsorption and generalized aminoaciduria indicate underlying complex proximal tubular disease (Fanconi syndrome). Kidney histology reveals immune-mediated glomerulonephritis as well as chronic tubulointerstitial nephritis with glomerulosclerosis in the absence of immune deposits [Estève et al 2017]. ... A clinical presentation resembling hemophagocytic lymphohistiocytosis/macrophagic activation syndrome has been repeatedly observed. Erythroblastophagocytosis and decreased megakaryocytes may be found in bone marrow aspirate. ... Hemophagocytic lymphohistiocytosis/macrophagic activation syndrome. Failure to thrive, hepatosplenomegaly, fever, hypertriglyceridemia, increased serum ferritin concentration, anemia, and other blood abnormalities suggest acquired or familial hemophagocytic lymphohistiocytosis. ... Treatment of hemophagocytic lymphohistiocytosis / macrophagic activation syndrome in LPI should be formulated under the direction of a specialist.
Lysinuric protein intolerance is a disorder caused by the body's inability to digest and use certain protein building blocks (amino acids), namely lysine, arginine, and ornithine. Because the body cannot effectively break down these amino acids, which are found in many protein-rich foods, nausea and vomiting are typically experienced after ingesting protein. People with lysinuric protein intolerance have features associated with protein intolerance, including an enlarged liver and spleen (hepatosplenomegaly), short stature, muscle weakness, impaired immune function, and progressively brittle bones that are prone to fracture (osteoporosis ). A lung disorder called pulmonary alveolar proteinosis may also develop. This disorder is characterized by protein deposits in the lungs , which interfere with lung function and can be life-threatening.
Oyanagi et al. (1970) described severe mental retardation, physical retardation, mild intestinal malabsorption syndrome, and increased urinary excretion of lysine, ornithine, and arginine in 2 Japanese sisters with second-cousin parents.
Lysinuric protein intolerance (LPI) is a very rare inherited multisystem condition caused by distrubance in amino acid metabolism. Epidemiology It is mainly found in Italy and Finland where prevalence is 1/60,000. Clinical description The metabolic disturbance in LPI causes increased renal excretion and reduced absorption from intestine of cationic amino acids, and orotic aciduria. Patients affected by LPI may present with vomiting, diarrhea, failure to thrive, hepatosplenomegaly, bone marrow abnormalities, osteopenia, episodes of hyperammoniaemic coma, mental retardation, altered immune response, chronic renal disease, and lung involvement (mostly pulmonary alveolar proteinosis - PAP - and, to a lesser extent, interstitial lung disease). Etiology It is caused by defective cationic amino acid transport at the basolateral membrane of epithelial cells in the kidney and intestine.
Lysinuric protein intolerance (LPI) is a genetic condition that is caused by the body's inability to digest the amino acids lysine, arginine, and ornithine. These are some of the building blocks of protein. Because the body cannot effectively break down these amino acids, which are found in many protein-rich foods, individuals experience nausea and vomiting after ingesting protein. Symptoms usually develop after infants are weaned and begin to eat solid foods. Without treatment, other signs and symptoms associated with protein intolerance may also occur, including short stature, muscle weakness, impaired immune function, and weak brittle bones (osteoporosis). The most serious symptoms involve the lung, kidney and heart. A lung disorder called pulmonary alveolar proteinosis may develop in some individuals, as can end-stage renal disease , coma and intellectual disability.
Obstructed defecation Other names rectal outlet obstruction, evacuatory dysfunction, obstructed defecation syndrome, outlet constipation, pelvic outlet obstruction [1] Specialty Gastroenterology , general surgery Obstructed defecation is "difficulty in evacuation or emptying the rectum [which] may occur even with frequent visits to the toilet and even with passing soft motions". [2] The conditions that can create the symptom are sometimes grouped together as defecation disorders. ... Another source defines evacuatory dysfunction as "a constellation of symptoms such as prolonged repeated straining at bowel movements, sensation of incomplete evacuation, and the need for digital manipulation". [1] Some describe an "obstructed defecation syndrome", defining it loosely as "difficulty in evacuation, which may or may not be associated with constipation." [2] Others inappropriately equate obstructed defecation with anismus . [3] Although anismus is a type of obstructed defecation, obstructed defecation has many other possible causes other than anismus. Contents 1 Signs and symptoms 2 Causes 2.1 Incomplete evacuation 3 Diagnosis 3.1 Classification 4 Treatment 5 See also 6 References Signs and symptoms [ edit ] incomplete or unsuccessful attempts to evacuate prolonged episodes on the toilet rectal pain posturing digitations or perineal massage to aid defecation enema dependency Fecal incontinence to gas, liquid, solid stool, or mucus in the presence of obstructed defecation symptoms may indicate occult rectal prolapse (i.e. rectal intussusception ), internal / external anal sphincter dysfunction, or descending perineum syndrome . [1] Causes [ edit ] One review stated that the most common causes of disruption to the defecation cycle are associated with pregnancy and childbirth, gynaecological descent or neurogenic disturbances of the brain-bowel axis. [4] Patients with obstructed defecation appear to have impaired pelvic floor function. [5] Specific causes include: Anismus [4] and pelvic floor dysfunction [6] Rectocele [6] [4] "Rectal invagination" (likely refers to rectal intussusception ) [4] Internal anal sphincter hypertonia [3] Anal stenosis [6] Fecal impaction [6] Rectal or anal cancer [6] Descending perineum syndrome [6] Incomplete evacuation [ edit ] Obstructed defecation may be a cause of incomplete evacuation of stool. [7] Normal emptying of rectal contents is 90-100%. <90% evacuation could be defined as incomplete evacuation. ... "[Functional obstructed defecation syndrome]". Duodecim; Laaketieteellinen Aikakauskirja . 125 (2): 221–5. ... "Five-Item Score for Obstructed Defecation Syndrome: Study of Validation". Surgical Innovation . 20 (2): 119–25. doi : 10.1177/1553350612446354 .
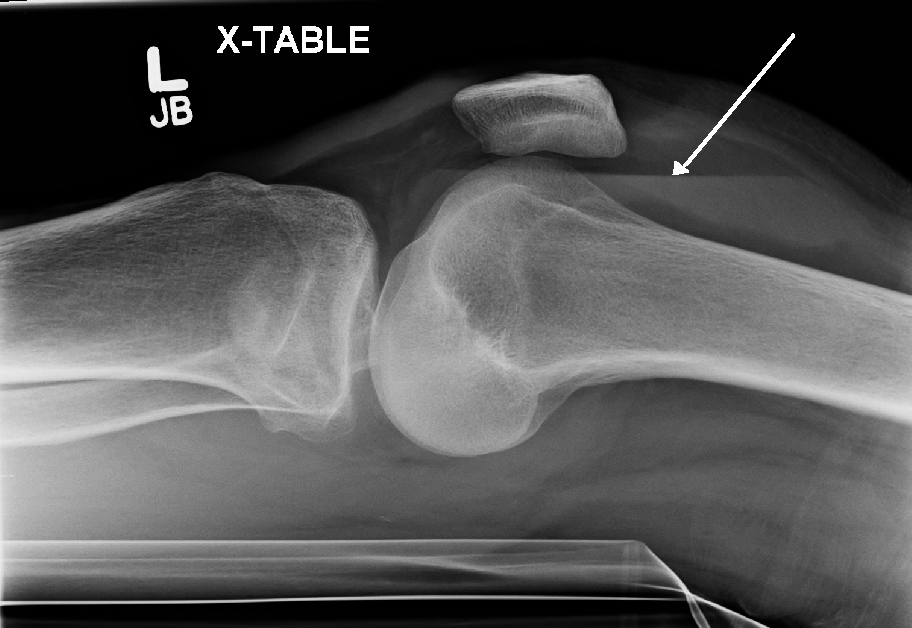
It can be associated with knee joint arthroplasty . [1] It has also been reported as a part of hemorrhagic syndrome in the Crimean-Congo Hemorrhagic Fever, suggesting a viral cause to the bleeding in a joint space. [2] [3] Diagnosis [ edit ] Synovial fluid examination [4] [5] Type WBC per mm 3 % neutrophils Viscosity Appearance Normal <200 0 High Transparent Osteoarthritis <5000 <25 High Clear yellow Trauma <10,000 <50 Variable Bloody Inflammatory 2,000-50,000 50-80 Low Cloudy yellow Septic arthritis >50,000 >75 Low Cloudy yellow Gonorrhea ~10,000 60 Low Cloudy yellow Tuberculosis ~20,000 70 Low Cloudy yellow Inflammatory = gout , rheumatoid arthritis , rheumatic fever Hemarthrosis is diagnosed through the methods listed below: A physical examination is the first step, the joints of the patient are moved and bent to study the functioning. [6] Synovial Fluid analysis is another method to diagnose Hemarthrosis. ... PMID 21901684 . ^ Goldberg A, Stansby G "Surgical Talk" 2nd edition External links [ edit ] Classification D ICD - 10 : M25.0 ICD - 9-CM : 719.1 MeSH : D006395 DiseasesDB : 29653 v t e Diseases of joints General Arthritis Monoarthritis Oligoarthritis Polyarthritis Symptoms Joint pain Joint stiffness Inflammatory Infectious Septic arthritis Tuberculosis arthritis Crystal Chondrocalcinosis CPPD (Psudogout) Gout Seronegative Reactive arthritis Psoriatic arthritis Ankylosing spondylitis Other Juvenile idiopathic arthritis Rheumatoid arthritis Felty's syndrome Palindromic rheumatism Adult-onset Still's disease Noninflammatory Hemarthrosis Osteoarthritis Heberden's node Bouchard's nodes Osteophyte v t e Disorders of bleeding and clotting Coagulation · coagulopathy · Bleeding diathesis Clotting By cause Clotting factors Antithrombin III deficiency Protein C deficiency Activated protein C resistance Protein S deficiency Factor V Leiden Prothrombin G20210A Platelets Sticky platelet syndrome Thrombocytosis Essential thrombocythemia DIC Purpura fulminans Antiphospholipid syndrome Clots Thrombophilia Thrombus Thrombosis Virchow's triad Trousseau sign of malignancy By site Deep vein thrombosis Bancroft's sign Homans sign Lisker's sign Louvel's sign Lowenberg's sign Peabody's sign Pratt's sign Rose's sign Pulmonary embolism Renal vein thrombosis Bleeding By cause Thrombocytopenia Thrombocytopenic purpura : ITP Evans syndrome TM TTP Upshaw–Schulman syndrome Heparin-induced thrombocytopenia May–Hegglin anomaly Platelet function adhesion Bernard–Soulier syndrome aggregation Glanzmann's thrombasthenia platelet storage pool deficiency Hermansky–Pudlak syndrome Gray platelet syndrome Clotting factor Hemophilia A/VIII B/IX C/XI von Willebrand disease Hypoprothrombinemia/II Factor VII deficiency Factor X deficiency Factor XII deficiency Factor XIII deficiency Dysfibrinogenemia Congenital afibrinogenemia Signs and symptoms Bleeding Bruise Hematoma Petechia Purpura Nonthrombocytopenic purpura By site head Epistaxis Hemoptysis Intracranial hemorrhage Hyphema Subconjunctival hemorrhage torso Hemothorax Hemopericardium Pulmonary hematoma abdomen Gastrointestinal bleeding Hemobilia Hemoperitoneum Hematocele Hematosalpinx joint Hemarthrosis
Although these features are no longer used in making a diagnosis, the name has remained. Cat eye syndrome , caused by the short arm (p) and a small section of the long arm (q) of human chromosome 22 being present three (trisomic) or four times (tetrasomic) instead of the usual two times. ... Treacher Collins syndrome , autosomal dominant syndrome caused by mutation of TCOF1 . Coloboma is part of a set of characteristic facies that features craniofacial malformations, such as downslanting eyes, ear anomalies, or hypoplasia of zygomatic bone and jaw (micrognathia). Tilted Disc Syndrome: An unusual congenital malformation associated with myopic astigmatism characterized by tilting of the intraocular tip of the optic nerve (the optic disc), also known as Fuchs coloboma. Causes [ edit ] Coloboma can be associated with a mutation in the PAX2 gene. [3] Eye abnormalities have been shown to occur in over 90% of children with fetal alcohol syndrome . [4] Diagnosis [ edit ] Typically a coloboma appears oval- or comet-shaped with round end towards the centre. ... PMID 9783702 . ^ "Eye abnormalities in fetal alcohol syndrome" . Ulster Med J . 78 : 164–5. Sep 2009.
Coloboma of choroid and retina is a rare, genetic developmental defect during embryogenesis characterized by the partial absence of retinal pigment epithelium and choroid, most frequently located in the inferonasal quadrant. Patients usually present reduced vision and have an increased risk for retinal detachment. Other ocular anomalies (e.g. coloboma of iris, microcornea, nystagmus, strabismus, microphthalmos) are usually associated, however it may also be isolated.
Some individuals have coloboma as part of a syndrome that affects other organs and tissues in the body. These forms of the condition are described as syndromic. When coloboma occurs by itself, it is described as nonsyndromic or isolated. ... When coloboma occurs as a feature of a genetic syndrome or chromosomal abnormality, it may cluster in families according to the inheritance pattern for that condition, which may be autosomal dominant, autosomal recessive, or X-linked.
During acute infection both direct peripheral nervous involvement, most commonly bilateral facial palsy, and an acute inflammatory demyelinating polyneuropathy ( Guillian-Barré syndrome ) have been reported. As the disease process progresses, diffuse infiltrative lymphocytosis syndrome may include a lymphocytic inflammation of peripheral nerves which results in a painful symmetric polyneuropathy. ... PMID 21527960 . ^ Chowdhury D, Arora A (May 2001). "Axonal Guillain-Barré syndrome: a critical review". Acta Neurologica Scandinavica . 103 (5): 267–77. doi : 10.1034/j.1600-0404.2001.103005267.x . ... "Diagnosis and management of Guillain-Barré syndrome in ten steps" . Nature Reviews. ... OCLC 972843900 . ^ Leypoldt F, Wandinger KP (March 2014). "Paraneoplastic neurological syndromes" . Clinical and Experimental Immunology . 175 (3): 336–48. doi : 10.1111/cei.12185 . ... "Diagnosis and management of Guillain-Barré syndrome in ten steps" . Nature Reviews.
A number sign (#) is used with this entry because it represents a contiguous gene syndrome caused by deletion of chromosome 17p13.1 Clinical Features Krepischi-Santos et al. (2009) reported a girl from the United Kingdom and 3 Brazilian boys, who were each found to have a microdeletion within or spanning chromosome 17p13.1. ... Molecular Genetics In 4 patients with syndromic mental retardation, Krepischi-Santos et al. (2009) identified microdeletions of chromosome 17p13.3-p13.1, ranging in size from 287 kb to 4.4 Mb, each with unique breakpoints. ... Although the TP53 gene was within the deleted region in this patient, she did not fulfill the criteria for Li-Fraumeni (151623) or Li-Fraumeni-like syndrome, as she had no tumor and a negative family history. ... The authors reviewed 7 previously reported patients with 17p13.1 microdeletions, including those of Krepischi-Santos et al. (2009) and Schwarzbraun et al. (2009), and stated that although all had mental retardation of variable degrees, their dysmorphic features were not specific and no recognizable syndrome emerged from comparison of the patients. ... In 4 of the patients, deletions were limited to the TP53 gene, and all 4 had childhood cancer and pedigrees consistent with the Li-Fraumeni syndrome but no neurocognitive symptoms.