Some people with high blood pressure report headaches (particularly at the back of the head and in the morning), as well as lightheadedness , vertigo , tinnitus (buzzing or hissing in the ears), altered vision or fainting episodes . [20] These symptoms, however, might be related to associated anxiety rather than the high blood pressure itself. [21] On physical examination , hypertension may be associated with the presence of changes in the optic fundus seen by ophthalmoscopy . [22] The severity of the changes typical of hypertensive retinopathy is graded from I to IV; grades I and II may be difficult to differentiate. [22] The severity of the retinopathy correlates roughly with the duration or the severity of the hypertension. [20] Secondary hypertension [ edit ] Main article: Secondary hypertension Hypertension with certain specific additional signs and symptoms may suggest secondary hypertension, i.e. hypertension due to an identifiable cause. For example, Cushing's syndrome frequently causes truncal obesity, glucose intolerance , moon face , a hump of fat behind the neck/shoulder (referred to as a buffalo hump), and purple abdominal stretch marks . [23] Hyperthyroidism frequently causes weight loss with increased appetite, fast heart rate , bulging eyes , and tremor. ... Insulin resistance , which is common in obesity and is a component of syndrome X (or the metabolic syndrome ), also contributes to hypertension. [40] Events in early life, such as low birth weight , maternal smoking , and lack of breastfeeding may be risk factors for adult essential hypertension, although the mechanisms linking these exposures to adult hypertension remain unclear. [41] An increased rate of high blood uric acid has been found in untreated people with hypertension in comparison with people with normal blood pressure, although it is uncertain whether the former plays a causal role or is subsidiary to poor kidney function. [42] Average blood pressure may be higher in the winter than in the summer. [43] Periodontal disease is also associated with high blood pressure. [44] Secondary hypertension [ edit ] Main article: Secondary hypertension Secondary hypertension results from an identifiable cause. Kidney disease is the most common secondary cause of hypertension. [23] Hypertension can also be caused by endocrine conditions, such as Cushing's syndrome , hyperthyroidism , hypothyroidism , acromegaly , Conn's syndrome or hyperaldosteronism , renal artery stenosis (from atherosclerosis or fibromuscular dysplasia ), hyperparathyroidism , and pheochromocytoma . [23] [45] Other causes of secondary hypertension include obesity , sleep apnea , pregnancy , coarctation of the aorta , excessive eating of liquorice , excessive drinking of alcohol, certain prescription medicines, herbal remedies, and stimulants such as cocaine and methamphetamine . [23] [46] Arsenic exposure through drinking water has been shown to correlate with elevated blood pressure. [47] [48] Depression was also linked to hypertension. [49] Loneliness is also a risk factor. [50] A 2018 review found that any alcohol increased blood pressure in males while over one or two drinks increased the risk in females. [51] Pathophysiology [ edit ] Main article: Pathophysiology of hypertension Determinants of mean arterial pressure Illustration depicting the effects of high blood pressure In most people with established essential hypertension , increased resistance to blood flow ( total peripheral resistance ) accounts for the high pressure while cardiac output remains normal. [52] There is evidence that some younger people with prehypertension or 'borderline hypertension' have high cardiac output, an elevated heart rate and normal peripheral resistance, termed hyperkinetic borderline hypertension. [53] These individuals develop the typical features of established essential hypertension in later life as their cardiac output falls and peripheral resistance rises with age. [53] Whether this pattern is typical of all people who ultimately develop hypertension is disputed. [54] The increased peripheral resistance in established hypertension is mainly attributable to structural narrowing of small arteries and arterioles , [55] although a reduction in the number or density of capillaries may also contribute. [56] It is not clear whether or not vasoconstriction of arteriolar blood vessels plays a role in hypertension. [57] Hypertension is also associated with decreased peripheral venous compliance [58] which may increase venous return , increase cardiac preload and, ultimately, cause diastolic dysfunction . ... In the United Kingdom, current best practice is to follow up a single raised clinic reading with ambulatory measurement, or less ideally with home blood pressure monitoring over the course of 7 days. [73] The United States Preventive Services Task Force also recommends getting measurements outside of the healthcare environment. [72] Pseudohypertension in the elderly or noncompressibility artery syndrome may also require consideration.
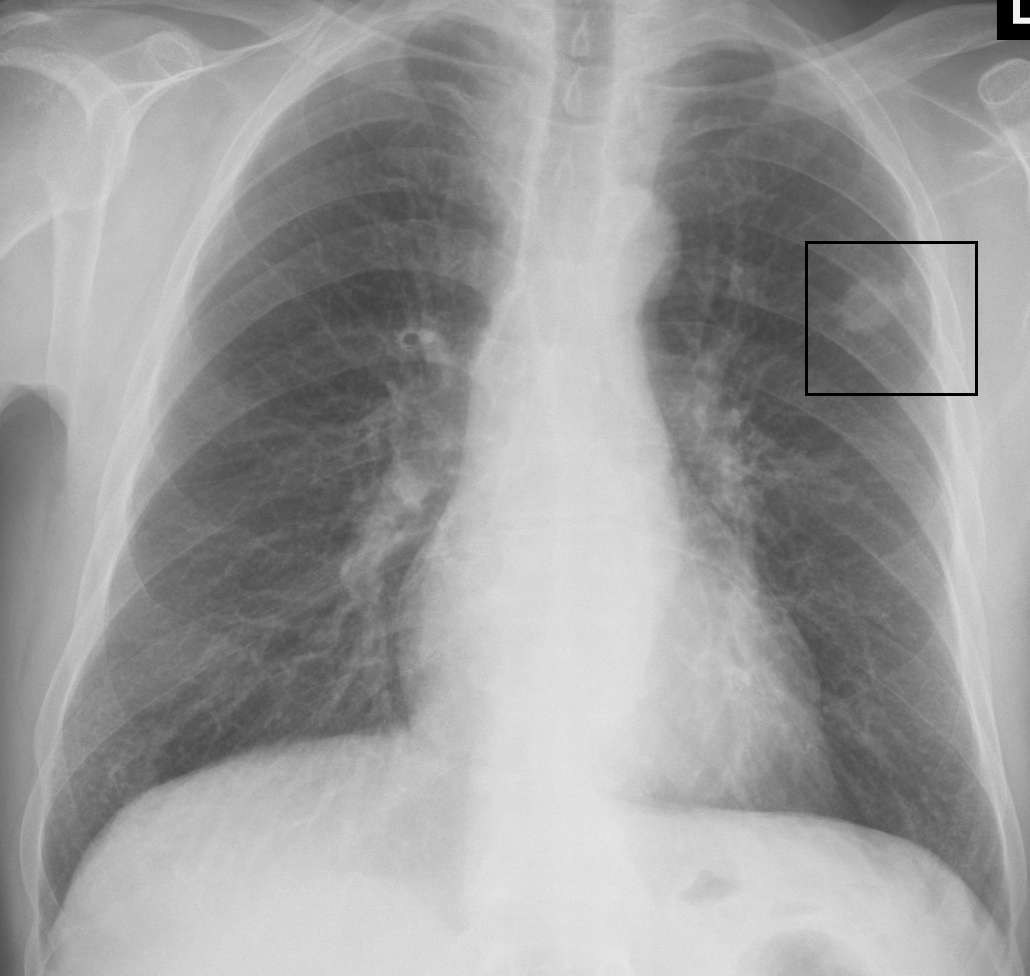
The body is remarkably good at hiding the symptoms and as a result people with RCC often have advanced disease by the time it is discovered. [5] The initial symptoms of RCC often include blood in the urine (occurring in 40% of affected persons at the time they first seek medical attention), flank pain (40%), a mass in the abdomen or flank (25%), weight loss (33%), fever (20%), high blood pressure (20%), night sweats and generally feeling unwell . [1] When RCC metastasises, it most commonly spreads to the lymph nodes , lungs , liver , adrenal glands , brain or bones. [6] Immunotherapy and targeted therapy have improved the outlook for metastatic RCC. [7] [8] RCC is also associated with a number of paraneoplastic syndromes (PNS) which are conditions caused by either the hormones produced by the tumour or by the body's attack on the tumour and are present in about 20% of those with RCC. [1] These syndromes most commonly affect tissues which have not been invaded by the cancer. [1] The most common PNSs seen in people with RCC are: high blood calcium levels , high red blood cell count , high platelet count and secondary amyloidosis . [6] Contents 1 Signs and symptoms 2 Risk factors 2.1 Lifestyle 2.2 Genetics 3 Pathophysiology 4 Diagnosis 4.1 Classification 4.2 Laboratory tests 4.2.1 Urine analysis 4.2.2 Complete blood cell count 4.2.3 Blood chemistry 4.3 Radiology 4.3.1 Computed tomography 4.3.2 Ultrasound 4.3.3 Magnetic resonance imaging 4.3.4 Intravenous pyelogram 4.3.5 Renal angiography 4.4 Staging 4.5 Histopathology 5 Prevention 6 Management 6.1 Active surveillance 6.2 Surgery 6.3 Percutaneous ablative therapies 6.4 Targeted drugs 6.5 Chemotherapy 6.6 Adjuvant and neoadjuvant therapy 7 Metastasis 8 Prognosis 9 Epidemiology 10 History 10.1 Hypernephroma controversy 11 See also 12 References 13 External links Signs and symptoms [ edit ] Historically, medical practitioners expected a person to present with three findings. ... Genetics [ edit ] Hereditary factors have a minor impact on individual susceptibility with immediate relatives of people with RCC having a two to fourfold increased risk of developing the condition. [22] Other genetically linked conditions also increase the risk of RCC, including hereditary papillary renal carcinoma , hereditary leiomyomatosis , Birt–Hogg–Dube syndrome , hyperparathyroidism-jaw tumor syndrome , familial papillary thyroid carcinoma , von Hippel–Lindau disease [23] and sickle cell disease . [24] The most significant disease affecting risk however is not genetically linked – patients with acquired cystic disease of the kidney requiring dialysis are 30 times more likely than the general population to develop RCC. [25] Pathophysiology [ edit ] The tumour arises from the cells of the proximal renal tubular epithelium. [1] It is considered an adenocarcinoma . [6] There are two subtypes: sporadic (that is, non-hereditary) and hereditary. [1] Both such subtypes are associated with mutations in the short-arm of chromosome 3 , with the implicated genes being either tumour suppressor genes ( VHL and TSC ) or oncogenes (like c-Met ). [1] Diagnosis [ edit ] The first steps taken to diagnose this condition are consideration of the signs and symptoms, and a medical history (the detailed medical review of past health state) to evaluate any risk factors. ... The drugs aim to inhibit the growth of new blood vessels in the tumors, hence slowing growth and in some cases reducing the size of the tumors. [100] Side effects unfortunately are quite common with these treatments and include: [101] Gastrointestinal effects – nausea, vomiting, diarrhea, anorexia Respiratory effects – coughing, dyspnea (difficulty breathing) Cardiovascular effects – hypertension (high blood pressure) Neurological effects – intracranial hemorrhage (bleeding into the brain), thrombosis (blood clots) in the brain Effects on the skin and mucus membranes – rashes, hand-foot syndrome , stomatitis Bone marrow suppression – resulting in reduced white blood cells, increasing the risk of infections plus anemia and reduced platelets Renal effects – impaired kidney function Fatigue. ... For metastatic renal cell carcinoma, factors which may present a poor prognosis include a low Karnofsky performance-status score (a standard way of measuring functional impairment in patients with cancer), a low haemoglobin level, a high level of serum lactate dehydrogenase, and a high corrected level of serum calcium. [106] [107] For non-metastatic cases, the Leibovich scoring algorithm may be used to predict post-operative disease progression. [108] Renal cell carcinoma is one of the cancers most strongly associated with paraneoplastic syndromes , most often due to ectopic hormone production by the tumour. ... They concluded that these features indicated that the tumours arose from the epithelial cells of the renal convoluted tubule , thus finally settling one of the most debated issues in tumour pathology. [110] [115] See also [ edit ] Stauffer syndrome Knudson hypothesis [116] Interleukin-2 Kidney cancer Rapamycin Vinblastine Dysuria Interferon References [ edit ] ^ a b c d e f g Curti, B; Jana, BRP; Javeed, M; Makhoul, I; Sachdeva, K; Hu, W; Perry, M; Talavera, F (26 February 2014).
(Leu1438_His1439dup) variant is associated with a unique phenotypic presentation that includes many features commonly seen in individuals with CHARGE syndrome including coloboma, choanal atresia, congenital heart defects, growth deficiency, genitourinary anomalies, and DD/ID. ... See OMIM Phenotypic Series: Autosomal dominant ID, Autosomal recessive ID, Nonsyndromic X-linked ID, and Syndromic X-linked ID. Table 2. Disorders to Consider in the Differential Diagnosis of RERE -Related Disorders View in own window Disorder Gene / Genetic Mechanism MOI Clinical Features of Differential Diagnosis Disorder Overlapping w/ RERE -related disorders Distinguishing from RERE -related disorders CHARGE syndrome CHD7 AD Colobomata, congenital heart defects, choanal atresia, ear anomalies, & genitourinary anomalies Neurocognitive defects Hearing loss Growth deficiencies Cranial nerve dysfunction or anomaly Semicircular canal defects Tracheoesophageal fistula 1p36 deletion syndrome (OMIM 607872) Deletion of 1p36 See footnote 1 Central nervous system anomalies, ophthalmologic abnormalities, congenital heart defects, & renal & genitourinary anomalies Neurocognitive abnormalities Hearing loss Typical dysmorphic features (straight eyebrows, deeply set eyes, midface retrusion, wide & depressed nasal bridge, long philtrum, pointed chin, epicanthal folds, posteriorly rotated & low-set ears) Late-closing anterior fontanelle AD = autosomal dominant; MOI = mode of inheritance 1.
Symptoms may not be noticed right away. Hypoplastic left heart syndrome. A major part of the heart fails to develop properly. In hypoplastic left heart syndrome, the left side of the heart hasn't developed enough to effectively pump enough blood to the body. ... Congenital heart defects sometimes run in families (are inherited) and may be associated with a genetic syndrome. Many children with an extra 21st chromosome (Down syndrome) have congenital heart defects.
A rare pulmonary condition characterized by accumulation of pus in the pleural cavity, most commonly as a consequence of pneumonia, but also trauma and surgical procedures. Clinical signs and symptoms depend on host factors, as well as the nature of the causative microorganism, among others, and include cough, chest pain, dyspnea, and fever.
Reading and spoken language are often impaired as well. [2] Gerstmann syndrome agraphia is the impairment of written language production associated with the following structural symptoms: difficulty discriminating between one's own fingers , difficulty distinguishing left from right, and difficulty performing calculations . [6] All four of these symptoms result from pathway lesions. [ citation needed ] Gerstmann's syndrome may additionally be present with alexia and mild aphasia. [3] [6] Global agraphia also impairs an individuals' orthographic memory although to a greater extent than deep agraphia. ... The eight other areas are considered associative areas and are the right anterior cerebellum , the left posterior nucleus of the thalamus , the left inferior frontal gyrus , the right posterior cerebellum, the right superior frontal cortex , the right inferior parietal lobule , the left fusiform gyrus and the left putamen . [10] The specific type of agraphia resulting from brain damage will depend on which area of the brain was damaged. [ citation needed ] Diagram of human brain showing surface gyri and the primary auditory cortex Angular gyrus Supramarginal gyrus Broca's area Wernicke's area Primary auditory cortex Phonological agraphia is linked to damage in areas of the brain involved in phonological processing skills (sounding out words), [7] specifically the language areas around the sylvian fissure , such as Broca's area , Wernicke's area , and the supramarginal gyrus . [2] Lexical agraphia is associated with damage to the left angular gyrus and/or posterior temporal cortex . [2] The damage is typically posterior and inferior to the perisylvian language areas. [2] Deep agraphia involves damage to the same areas of the brain as lexical agraphia plus some damage to the perisylvian language areas as well. [2] More extensive left hemisphere damage can lead to global agraphia. [2] Gerstmann's syndrome is caused by a lesion of the dominant (usually the left) parietal lobe, usually an angular gyrus lesion. [3] Apraxic agraphia with ideomotor apraxia is typically caused by damage to the superior parietal lobe (where graphomotor plans are stored) or the premotor cortex (where the plans are converted into motor commands). [1] Additionally, some individuals with cerebellar lesions (more typically associated with non-apraxic motor dysfunction) develop apraxic agraphia. [1] Apraxic agraphia without ideomotor apraxia may be caused by damage to either of the parietal lobes, the dominant frontal lobe, or to the dominant thalamus. [1] Visuospatial agraphia typically has a right hemisphere pathology. [8] Damage to the right frontal area of the brain may cause more motor defects, whereas damage to the posterior part of the right hemisphere leads predominantly to spatial defects in writing. [11] [ citation needed ] Alzheimer's disease [ edit ] Agraphia is often seen in association with Alzheimer's Disease (AD). ... S2CID 16422157 . ^ a b Rusconi E, Pinel P, Dehaene S, Kleinschmidt A (February 2010). "The enigma of Gerstmann's syndrome revisited: a telling tale of the vicissitudes of neuropsychology" .
Contents 1 Examples 1.1 Nausea (morning sickness) 1.2 Bleeding 1.3 Back pain 1.4 Pelvic girdle pain 1.5 Carpal tunnel syndrome 1.6 Leg cramps 1.7 Constipation 1.8 Contractions 1.9 Dehydration 1.10 Edema 1.11 Regurgitation and heartburn 1.12 Varicose veins 1.13 Hemorrhoids 1.14 Pica 1.15 Round Ligament or Lower abdominal pain 1.16 Increased urinary frequency 1.17 Diastasis recti or abdominal separation 1.18 Striae gravidarum 1.19 Generalized itching 2 See also 3 References Examples [ edit ] Nausea (morning sickness) [ edit ] Main article: Morning sickness Morning sickness occurs in about seventy percent of all pregnant women, and typically improves after the first trimester. [1] Although described as "morning sickness", women can experience this nausea during the afternoon, evening, and throughout the entire day. ... Moderate-quality evidence from a systematic review suggest that exercise or acupuncture reduced pelvic pain or lumbo-pelvic pain more than usual care. [13] Carpal tunnel syndrome [ edit ] Occurs in between an estimated 21% to 62% of cases, possibly due to edema . [14] Leg cramps [ edit ] Leg cramps (involuntary spasms in calf muscles) can affect between 30% to 50% of women during pregnancy, especially during the last three months of pregnancy. [15] Leg cramps can be extremely painful and whilst they usually last only a few seconds, they can last for minutes. [16] It is not clear whether some oral drug treatments (such as magnesium, calcium, vitamin B or vitamin C) are effective in treating leg cramps during pregnancy, nor whether these treatments are safe for the mother or her baby. [17] There is no evidence to assess the effectiveness and safety of other non-drug treatments such as heat therapy, massage or stretching the muscles (or dorso-flexion of the foot). [17] These Are Some Examples Of Pregnancy Constipation [ edit ] Constipation is believed to be caused by decreased bowel mobility secondary to elevated progesterone (normal in pregnancy), which can lead to greater absorption of water, but it can also be caused or worsened by iron supplementation. [5] It causes the " smooth muscle " along the walls of the intestines to relax. ... "Long term follow-up of carpal tunnel syndrome during pregnancy: a cohort study and review of the literature". ... PMID 26342714 . ^ Lawrensia S, Khan YS (July 2020). "Inferior Vena Cava Syndrome" . StatPearls. PMID 32809720 .
Related visual distortion conditions include macropsia , a less common condition with the reverse effect, and Alice in Wonderland Syndrome , a condition that has symptoms that can include both micropsia and macropsia. ... Women appear to be affected more than men by a factor of almost 3 to 1. [24] Society and culture [ edit ] Comparison with Alice's Adventures in Wonderland [ edit ] Alice in Wonderland Syndrome , a neurological condition associated with both micropsia and macropsia, is named after Lewis Carroll's famous 19th century novel Alice's Adventures in Wonderland . ... A number of surgical treatments are also being investigated for macular degeneration lesions that may not qualify for laser treatment, including macular translocation to a healthier area of the eye, displacement of submacular blood using gas, and removing membranes by surgery. [26] See also [ edit ] Alice in Wonderland syndrome Convergence micropsia Dysmetropsia Macropsia References [ edit ] ^ Lipsanen T, Korkeila J, Saarijärvi S, Lauerma H (March 2003). ... PMID 13748178 . ^ Cinbis M, Aysun S (May 1992). "Alice in Wonderland syndrome as an initial manifestation of Epstein-Barr virus infection" (PDF) .
Overview Laryngitis is an inflammation of your voice box (larynx) from overuse, irritation or infection. Inside the larynx are your vocal cords — two folds of mucous membrane covering muscle and cartilage. Normally, your vocal cords open and close smoothly, forming sounds through their movement and vibration. How speech occurs Speech occurs when air flows from the lungs, up the windpipe (trachea) and through the voice box (larynx). This causes the vocal cords to vibrate, creating sound. Sound is shaped into words by the muscles controlling the soft palate, tongue and lips.
The talk page may contain suggestions. ( May 2009 ) Hemiballismus Other names Ballismus or Ballism Specialty Neurology Hemiballismus or hemiballism is a basal ganglia syndrome resulting from damage to the subthalamic nucleus in the basal ganglia . [1] Hemiballismus is a rare hyperkinetic movement disorder , [2] that is characterized by violent involuntary limb movements, [1] [3] on one side of the body, [4] and can cause significant disability. [5] Ballismus affects both sides of the body and is much rarer. [4] Symptoms can decrease during sleep. [6] Hemiballismus differs from chorea in that the movements occur in the proximal limbs whereas in chorea the limb movements are in the distal limbs. [4] Also in chorea the movements are more dance-like, flowing from one region to another. [7] Contents 1 Presentation 2 Causes 3 Anatomy 4 Diagnosis 5 Treatments 6 Prognosis 7 History 8 See also 9 References 10 External links Presentation [ edit ] Ballism was defined by Meyers in 1968 [8] as "Repetitive, but constantly varying, large amplitude involuntary movements of the proximal parts of the limbs. ... External links [ edit ] Classification D ICD - 10 : G25.5 ICD - 9-CM : 333.5 MeSH : D020820 v t e Diseases of the nervous system , primarily CNS Inflammation Brain Encephalitis Viral encephalitis Herpesviral encephalitis Limbic encephalitis Encephalitis lethargica Cavernous sinus thrombosis Brain abscess Amoebic Brain and spinal cord Encephalomyelitis Acute disseminated Meningitis Meningoencephalitis Brain / encephalopathy Degenerative Extrapyramidal and movement disorders Basal ganglia disease Parkinsonism PD Postencephalitic NMS PKAN Tauopathy PSP Striatonigral degeneration Hemiballismus HD OA Dyskinesia Dystonia Status dystonicus Spasmodic torticollis Meige's Blepharospasm Athetosis Chorea Choreoathetosis Myoclonus Myoclonic epilepsy Akathisia Tremor Essential tremor Intention tremor Restless legs Stiff-person Dementia Tauopathy Alzheimer's Early-onset Primary progressive aphasia Frontotemporal dementia / Frontotemporal lobar degeneration Pick's Dementia with Lewy bodies Posterior cortical atrophy Vascular dementia Mitochondrial disease Leigh syndrome Demyelinating Autoimmune Inflammatory Multiple sclerosis For more detailed coverage, see Template:Demyelinating diseases of CNS Episodic/ paroxysmal Seizures and epilepsy Focal Generalised Status epilepticus For more detailed coverage, see Template:Epilepsy Headache Migraine Cluster Tension For more detailed coverage, see Template:Headache Cerebrovascular TIA Stroke For more detailed coverage, see Template:Cerebrovascular diseases Other Sleep disorders For more detailed coverage, see Template:Sleep CSF Intracranial hypertension Hydrocephalus Normal pressure hydrocephalus Choroid plexus papilloma Idiopathic intracranial hypertension Cerebral edema Intracranial hypotension Other Brain herniation Reye syndrome Hepatic encephalopathy Toxic encephalopathy Hashimoto's encephalopathy Both/either Degenerative SA Friedreich's ataxia Ataxia–telangiectasia MND UMN only: Primary lateral sclerosis Pseudobulbar palsy Hereditary spastic paraplegia LMN only: Distal hereditary motor neuronopathies Spinal muscular atrophies SMA SMAX1 SMAX2 DSMA1 Congenital DSMA Spinal muscular atrophy with lower extremity predominance (SMALED) SMALED1 SMALED2A SMALED2B SMA-PCH SMA-PME Progressive muscular atrophy Progressive bulbar palsy Fazio–Londe Infantile progressive bulbar palsy both: Amyotrophic lateral sclerosis v t e Symptoms and signs relating to movement and gait Gait Gait abnormality CNS Scissor gait Cerebellar ataxia Festinating gait Marche à petit pas Propulsive gait Stomping gait Spastic gait Magnetic gait Truncal ataxia Muscular Myopathic gait Trendelenburg gait Pigeon gait Steppage gait Antalgic gait Coordination Ataxia Cerebellar ataxia Dysmetria Dysdiadochokinesia Pronator drift Dyssynergia Sensory ataxia Asterixis Abnormal movement Athetosis Tremor Fasciculation Fibrillation Posturing Abnormal posturing Opisthotonus Spasm Trismus Cramp Tetany Myokymia Joint locking Paralysis Flaccid paralysis Spastic paraplegia Spastic diplegia Spastic paraplegia Syndromes Monoplegia Diplegia / Paraplegia Hemiplegia Triplegia Tetraplegia / Quadruplegia General causes Upper motor neuron lesion Lower motor neuron lesion Weakness Hemiparesis Other Rachitic rosary Hyperreflexia Clasp-knife response
Overview Genital warts are one of the most common types of sexually transmitted infections. Nearly all sexually active people will become infected with at least one type of human papillomavirus (HPV), the virus that causes genital warts, at some point during their lives. Genital warts affect the moist tissues of the genital area. They can look like small, flesh-colored bumps or have a cauliflower-like appearance. In many cases, the warts are too small to be visible. Some strains of genital HPV can cause genital warts, while others can cause cancer. Vaccines can help protect against certain strains of genital HPV . Symptoms In women, genital warts can grow on the vulva, the walls of the vagina, the area between the external genitals and the anus, the anal canal, and the cervix.
In addition, 10–15% of severe aplastic anemia cases evolve into myelodysplastic syndrome and leukemia . [ citation needed ] According to a study, for children who underwent immunosuppressive therapy, about 15.9% of children who responded to immunosuppressive therapy encountered relapse. [18] Milder disease can resolve on its own. [ citation needed ] Etymology [ edit ] Aplastic is a combination of two ancient Greek elements: a- meaning "not", and -plasis "forming into a shape." [19] Anemia is a combination of the ancient Greek element an- meaning "not", and -emia from new Latin from Greek -(h)aimia "blood." [20] Epidemiology [ edit ] Aplastic anemia is a rare, non cancerous disorder where the blood marrow is unable to adequately produce blood cells required for survival. [21] [22] It is estimated that the incidence of aplastic anemia is 0.7-4.1 cases per million people worldwide with the prevalence between men and women being approximately equal. [23] The incidence rate of aplastic anemia in Asia is 2-3 times higher than it is in the West, with the incidence of the disease in the United States is 300-900 cases per year. [22] [23] The disease most commonly affects adults aged 15–25 and over the age of 60, but the disease can be observed in all age groups. [22] The majority of instances of this disease are acquired during life and not inherited. [21] These acquired cases are often linked to environmental exposures such as chemicals, drugs, and infectious agents that damage the blood marrow and compromise the ability of the marrow to generate new blood cells. [23] However, in many instances the underlying cause for the disease is not found. ... External links [ edit ] Mayo Clinic MedlinePlus Encyclopedia : 000554 —Idiopathic aplastic anemia Classification D ICD - 10 : D60 - D61 ICD - 9-CM : 284 OMIM : 609135 MeSH : D000741 DiseasesDB : 866 External resources MedlinePlus : 000554 eMedicine : med/162 v t e Diseases of red blood cells ↑ Polycythemia Polycythemia vera ↓ Anemia Nutritional Micro- : Iron-deficiency anemia Plummer–Vinson syndrome Macro- : Megaloblastic anemia Pernicious anemia Hemolytic (mostly normo- ) Hereditary enzymopathy : Glucose-6-phosphate dehydrogenase deficiency glycolysis pyruvate kinase deficiency triosephosphate isomerase deficiency hexokinase deficiency hemoglobinopathy : Thalassemia alpha beta delta Sickle cell disease / trait Hereditary persistence of fetal hemoglobin membrane : Hereditary spherocytosis Minkowski–Chauffard syndrome Hereditary elliptocytosis Southeast Asian ovalocytosis Hereditary stomatocytosis Acquired AIHA Warm antibody autoimmune hemolytic anemia Cold agglutinin disease Donath–Landsteiner hemolytic anemia Paroxysmal cold hemoglobinuria Mixed autoimmune hemolytic anemia membrane paroxysmal nocturnal hemoglobinuria Microangiopathic hemolytic anemia Thrombotic microangiopathy Hemolytic–uremic syndrome Drug-induced autoimmune Drug-induced nonautoimmune Hemolytic disease of the newborn Aplastic (mostly normo- ) Hereditary : Fanconi anemia Diamond–Blackfan anemia Acquired: Pure red cell aplasia Sideroblastic anemia Myelophthisic Blood tests Mean corpuscular volume normocytic microcytic macrocytic Mean corpuscular hemoglobin concentration normochromic hypochromic Other Methemoglobinemia Sulfhemoglobinemia Reticulocytopenia
Overview Aplastic anemia is a condition that occurs when your body stops producing enough new blood cells. The condition leaves you fatigued and more prone to infections and uncontrolled bleeding. A rare and serious condition, aplastic anemia can develop at any age. It can occur suddenly, or it can come on slowly and worsen over time. It can be mild or severe. Treatment for aplastic anemia might include medications, blood transfusions or a stem cell transplant, also known as a bone marrow transplant.
Without treatment there may be poor muscle tone, trouble with coordination, trouble talking, and seizures . [18] The causes of cerebral folate deficiency include mutations of genes responsible for folate metabolism and transport. [19] Mutations of the SLC46A1 gene that encodes the proton-coupled folate transporter (PCFT) result in CFD syndromes with both systemic folate deficiency and cerebral folate deficiency. ... "The proton-coupled folate transporter (PCFT-SLC46A1) and the syndrome of systemic and cerebral folate deficiency of infancy: Hereditary folate malabsorption" . ... External links [ edit ] Classification D ICD - 10 : D52 E53.8 ICD - 9-CM : 266.2 MeSH : D005494 DiseasesDB : 4894 External resources MedlinePlus : 000354 eMedicine : med/802 v t e Malnutrition Protein-energy malnutrition Kwashiorkor Marasmus Catabolysis Vitamin deficiency B vitamins B 1 Beriberi Wernicke–Korsakoff syndrome Wernicke's encephalopathy Korsakoff's syndrome B 2 Riboflavin deficiency B 3 Pellagra B 6 Pyridoxine deficiency B 7 Biotin deficiency B 9 Folate deficiency B 12 Vitamin B 12 deficiency Other A: Vitamin A deficiency Bitot's spots C: Scurvy D: Vitamin D deficiency Rickets Osteomalacia Harrison's groove E: Vitamin E deficiency K: Vitamin K deficiency Mineral deficiency Sodium Potassium Magnesium Calcium Iron Zinc Manganese Copper Iodine Chromium Molybdenum Selenium Keshan disease Growth Delayed milestone Failure to thrive Short stature Idiopathic General Anorexia Weight loss Cachexia Underweight
Kraus et al. (1986) demonstrated that mean activity of cystathionine synthase (CBS; 613381), which is on chromosome 21, is 166% in cultured fibroblasts from Down syndrome patients compared with controls. Brattstrom et al. (1987) suggested that if cystathionine synthase deficiency is involved in the pathophysiology of arteriosclerosis, Down syndrome patients might be protected against arteriosclerosis. Indeed, Murdoch et al. (1977) found that arteriosclerosis was rare in Down syndrome and referred to this disorder as an 'atheroma-free model.' Brattstrom et al. (1987) likewise found a remarkable freedom from arteriosclerosis in Down syndrome. In cultured human hepatocytes and vascular endothelial and aortic smooth muscle cells, Werstuck et al. (2001) found that homocysteine-induced endoplasmic reticulum (ER) stress activated both the unfolded protein response and sterol regulatory element-binding proteins (SREBPs).
T-cell large granular lymphocyte leukemia is a rare cancer of a type of white blood cells called lymphocytes. T-cell large granular lymphocyte leukemia causes a slow increase in white blood cells called T lymphocytes, or T cells, which originate in the lymph system and bone marrow and help to fight infection. This disease usually affects people in their sixties. Symptoms include anemia; low levels of platelets (thrombocytopenia) and infection-fighting neutrophils ( neutropenia ) in the blood; and an enlarged spleen . About one-third of patients are asymptomatic at the time of diagnosis. The exact cause of LGL leukemia is unknown. Doctors can diagnose this disease through a bone marrow biopsy , or by using a specialized technique in which various types of blood or bone marrow cells are separated, identified, and counted.
Song et al. (2013) showed in mice that muscle-specific mitsugumin-53 (MG53; 613288) mediates the degradation of the insulin receptor and Irs1, and when upregulated causes metabolic syndrome featuring insulin resistance, obesity, hypertension, and dyslipidemia. Mg53 expression is markedly elevated in models of insulin resistance, and Mg53 overexpression suffices to trigger muscle insulin resistance and metabolic syndrome sequentially. Conversely, ablation of Mg53 prevents diet-induced metabolic syndrome by preserving the insulin receptor, Irs1, and insulin signaling integrity.
Description The paraoxonase (PON) gene family includes 3 genes, PON1, PON2 (602447), and PON3 (602720), aligned next to each other on chromosome 7. PON1 (EC 3.1.1.2) hydrolyzes the toxic oxon metabolites of several organophosphorous insecticides, including parathion, diazinon, and chlorpyrifos, as well as nerve agents, such as sarin and soman. PON1 also hydrolyzes aromatic esters, preferably those of acetic acid. In addition, PON1 hydrolyzes a variety of aromatic and aliphatic lactones, and it also catalyzes the reverse reaction, lactonization, of gamma- and delta-hydroxycarboxylic acids. Human PON1 is synthesized in liver and secreted into blood, where it is associated exclusively with high density lipoproteins (HDLs) and may protect against development of atherosclerosis (Draganov et al., 2005).
During experiments aimed at building a contiguous group of YACs spanning 22q11, Dunham et al. (1992) found that the HP500 sequence often deleted in the velocardiofacial syndrome (VCFS; 192430) was located within the same 450-kb YAC as the COMT gene. They raised the question of whether low COMT might be responsible for psychotic illness, which is a feature of the VCF syndrome in adolescents and adults (Shprintzen et al., 1992). Biochemical Features Gustavson et al. (1973, 1982) reported that COMT activity was about 40% higher in Down syndrome children than in normal controls.