-
Prenatal Cocaine Exposure
Wikipedia
Reporting was often sensational , favoring the direst predictions and shutting out skeptics. [18] Powder (left) and crack cocaine (right) Reporting on the effects of PCE may have been affected by publication bias , a disproportionate publication of studies indicating more severe outcomes as the crack epidemic emerged. [19] Scientific studies that report that PCE has significant effects may be more likely to be published than those that do not. [20] Between 1980 and 1989, 57% of studies showing cocaine has effects on a fetus were accepted by the Society for Pediatric Research, compared with only 11% of studies showing no effects. [21] Findings that other factors such as prematurity were behind symptoms that cocaine-exposed babies showed did not "fit within the narrative of what had become a national scare" and were given less attention. [22] Ideas about severe effects of PCE may have been more readily embraced because they "fit in with cultural stereotypes". [22] At the time, the proposed mechanism by which cocaine harmed fetuses was as a stimulant—it was predicted that cocaine would disrupt normal development of parts of the brain that dealt with stimulation, resulting in problems like bipolar disorder and attention deficit disorder . [2] Reports from the mid-1980s to early 90s raised concerns about links between PCE and slowed growth, deformed limbs, defects of the kidneys and genitourinary and gastrointestinal systems , neurological damage, small head size , atrophy or cysts in the cerebral cortex , bleeding into the brain's ventricles , and obstruction of blood supply in the central nervous system . [19] After the early studies that reported that PCE children would be severely disabled came studies that purported to show that cocaine exposure in utero has no important effects. [17] Almost every prenatal complication originally thought to be due directly to PCE was found to result from confounding factors such as poor maternal nutrition, use of other drugs, depression , and lack of prenatal care . [23] More recently the scientific community has begun to reach an understanding that PCE does have some important effects but that they are not severe as was predicted in the early studies. [17] The effects of PCE are subtle but they exist. [19] [24] [25] Most people who were exposed to cocaine in utero are normal or close to it. [12] Pathophysiology [ edit ] Cocaine is a small enough molecule to pass across the placental barrier into the bloodstream of the fetus. [26] Cocaine, a small molecule, is able to cross the placenta into the bloodstream of the fetus. [26] [27] In fact it may be present in a higher concentration in the amniotic fluid than it is in the mother's bloodstream. [28] The skin of the fetus is able to absorb the chemical directly from the amniotic fluid until the 24th week of pregnancy. [28] Cocaine can also show up in breast milk and affect the nursing baby. [28] [29] The severity of effects depends on how much of the drug is used, how often, and the stage in the development of the fetus. [30] Cocaine prevents the reuptake of the neurotransmitters dopamine , serotonin , and norepinephrine . [20] Thus they stay in the synapse longer, causing excitement of the sympathetic nervous system and evoking a stress response. [21] The euphoria experienced by cocaine users is thought to be largely due to the way it prevents the neurotransmitter serotonin from being reabsorbed by the presynaptic neuron which released it. [31] [1] [20] Use of cocaine during pregnancy can negatively affect both the mother and the fetus, [21] but the ways in which it affects the fetus are poorly understood. [23] There are three main mechanisms by which cocaine exposure harms a fetus: by altering brain chemistry , by altering the expression of certain genes , and by the constriction of blood vessels. [1] The neurotransmitters affected by cocaine are involved in the development of the fetus's brain, [30] so the drug may affect fetal development directly by altering the development of the brain's monoaminergic system. [32] The most important way cocaine affects fetal development is by binding to dopamine receptors . [12] Another possible mechanism by which cocaine harms the fetus may be in part by interfering with blood supply to the uterus. [28] [33] Cocaine causes vasoconstriction (narrowing of blood vessels) in both mother and fetus, which can cause hypoxia in the fetus. [34] Constricting blood vessels causes tissues to receive insufficient blood flow, killing cells, but this effect is less pronounced with cocaine than with nicotine . [8] The reduction in blood flow to the uterus limits the delivery of oxygen and nutrients to the fetus. [16] Cocaine also constricts the blood vessels in the fetus, which is potentially linked to slowed fetal growth and abnormal development of the genitourinary , cardiovascular , digestive , and musculoskeletal systems . [30] Cocaine causes changes in the mother's blood pressure that are thought to be the cause of strokes in the fetus; one study found that 6% of cocaine-exposed infants had had one or more strokes. [28] Such prenatal strokes may be the cause of neurological problems found in some cocaine-exposed infants after birth. [5] Blood vessel contraction can also cause premature labor and premature birth. [16] Cocaine has also been found to enhance the contractility of the tissue in the uterus , another factor that has been suggested as a possible mechanism for its contribution to increased prematurity rates. [33] Increased contractility of the uterus may also be behind the increased likelihood of placental abruption (the placenta tearing away from the uterine wall) which some findings have linked with PCE. [21] Diagnosis [ edit ] Cocaine use during pregnancy can be discovered by asking the mother, but sometimes women will not admit to having used drugs. [35] Mothers may lie for fear of prosecution [35] or having their children taken away, but even when they are willing to tell the truth their memories may not be very accurate. [8] It may also not be possible to be sure of the purity of the drug they have taken. [36] More reliable methods for detecting cocaine exposure involve testing the newborn's hair or meconium (the infant's earliest stool). [37] Hair analysis, however, can give false positives for cocaine exposure, [37] and a newborn may not have enough hair to test. [8] The newborn's urine can be tested for cocaine and metabolites , but it must be collected as soon as possible after birth. [36] It is not known how long after exposure the markers will still show up in a newborn's urine. [35] The mother's urine can also be tested for drugs, but it cannot detect drugs used too far in the past or determine how much or how often the drugs were used. [8] Tests cannot generally detect cocaine use over a week prior to sample collection. [35] Mothers are more honest about cocaine use when their urine is also tested, but many users still deny it. [35] Both maternal and neonatal urine tests can give false negatives . [35] Effects and prognosis [ edit ] Studies have returned widely varying reports of the effects of PCE: some claim the physical disabilities are severe and generalized, others find specific effects, others none all. [1] The timing of the dose of the drug is an important determinant of outcome, in addition to how much is used, for how long, and what kind of care is rendered after birth. [1] Drug use in the first trimester is the most harmful to the fetus in terms of neurological and developmental outcome. [38] The effects of PCE later in a child's life are poorly understood; there is little information about the effects of in utero cocaine exposure on children over the age of five years old. [4] Some studies have found PCE-related differences in height and weight while others have not; these differences are generally either small or are gone by the time children are school age. [4] Much is still not known about what factors may exist to aid children who were exposed to cocaine in utero . [23] It is unknown if the effects of PCE are increased once children reach adolescence, or whether the neural rewiring that occurs during this developmental period attenuates the effects. [20] A review of 27 studies performed between 2006 and 2012 found that cognitive development was mildly to moderately affected in PCE adolescents, but it was not clear how important these effects were in practical terms. [20] Unlike fetal alcohol syndrome , no set of characteristics has been discovered that results uniquely from cocaine exposure in utero . [23] Cocaine exposure in utero may affect the structure and function of the brain, predisposing children to developmental problems later, or these effects may be explained by children of crack-using mothers being at higher risk for domestic violence , deadbeat parenting , and maternal depression . [4] When researchers are able to identify effects of PCE, these effects are typically small. [23] Pregnancy and birth [ edit ] Premature baby Studies have found after controlling for other factors that some effects are present in pregnancies involving cocaine: abruptio placenta , prematurity , low birth weight , and small size compared to babies of the same gestational time. [27] PCE newborns have smaller heads and shorter bodies. [9] [1] PCE effects are more severe when the amounts of cocaine are greater. [27] As many as 17–27% of cocaine-using pregnant women deliver prematurely. [33] In association with prematurity, growth in the womb is reduced, and low birth weight is connected to PCE. [20] There are also data associating spontaneous abortion with cocaine use. [15] Cocaine reduces the appetite and has been linked with reduced maternal weight gain during pregnancy; in addition, constriction of the blood vessels may further limit supply of nutrients to the fetus. [39] Using cocaine while pregnant also heightens the chances of maternal and fetal vitamin deficiencies, respiratory distress syndrome for the baby, and infarction of the bowels. [28] Early reports found that cocaine-exposed babies were at high risk for sudden infant death syndrome ; [19] however, by itself, cocaine exposure during fetal development has not subsequently been identified as a risk factor for the syndrome. [40] Some, but not all, PCE children experience hypertonia (excessive muscle tone ), [41] and reduced reflexes and motor function have been found in babies four to six weeks old. [20] While newborns who were exposed prenatally to drugs such as barbiturates or heroin frequently have symptoms of drug withdrawal ( neonatal abstinence syndrome ), this does not happen with babies exposed to crack in utero ; at least, such symptoms are difficult to separate in the context of other factors such as prematurity or prenatal exposure to other drugs. [16] Mental, emotional, and behavioral outcomes [ edit ] Studies have shown small deficits in behavioral, cognitive, attention, emotional, and language function in PCE infants, children, and adolescents. [20] However, other studies attribute findings of negative effects on cognitive development to confounding factors. [8] Studies suggest that the environment in which a child grows up makes a more important contribution to outcome in cognitive, behavioral and other outcomes than does the cocaine exposure itself. [9] School performance is mildly affected in older children. [27] In IQ studies, cocaine-exposed children do not appear to score lower than others. [1] Although PCE is correlated with low IQ scores, scientists generally believe that PCE alone does not cause this effect; rather it is more likely due to associated factors. [9] In school-age and younger children, PCE does not appear in studies to predispose children to poorer intellectual performance. [4] Poor performance on IQ tests could actually be due to trouble with sustaining attention if the tests fail to account for this factor separately. [8] Cocaine causes impaired growth of the fetus's brain, an effect that is most pronounced with high levels of cocaine and prolonged duration of exposure throughout all three trimesters of pregnancy. [41] Prenatal cocaine exposure has been found to affect the cognitive performance of individuals and affect speech and language development, behavior, physical and cognitive growth, and function. ... Prenatal Exposure to Drugs/Alcohol: Characteristics And Educational Implications of Fetal Alcohol Syndrome And Cocaine/polydrug Effects . ... External links [ edit ] Crack Babies: A Tale from the Drug Wars , a documentary from The New York Times v t e Infants and their care Health ( Pediatrics ) Baby food Birth weight Breast pump Breastfeeding Breastfeeding and medications Bottle feeding Colic Immunizations Cradle cap Cross eyed Failure to thrive Immunization Infant and toddler safety Infant bathing Infant food safety Infant formula Infant massage Infant food safety Infant nutrition Infant respiratory distress syndrome Infant sleep training Neo-natal intensive care unit Newborn care and safety Oral rehydration therapy Pedialyte Preterm birth Shaken baby syndrome Soy formula Sudden infant death syndrome Breastfeeding and mental health Development Attachment parenting Baby-led weaning Baby talk Babbling Childbirth Congenital disorder Crawling Infant visual development Diaper rash Gestational age Infant cognitive development Kangaroo care Mother Nursery Rhyme Object permanence Parent Parenting Peekaboo Play Prenatal development Prenatal development table Teething Types of crying Walking Weaning Socialization and Culture Attachment Babysitting Child abuse Child custody Child's rights UN Child rights Circumcision Daycare Foster care Grandparent visitation Infant swimming Milk bank Nanny Wet nurse Infant care and equipment Baby bouncer Baby gate Baby monitor / Hidden camera Baby powder Baby shampoo Baby toy Baby walker Bib Baby swing Baby transport Bassinet Car seat safety Cloth diaper Cradle board Diaper Diaper bag Baby wipes Haberman Feeder High chair Infant bed (American 'crib' and 'cradle', British 'cot') Infant carrier Infant clothing Pacifier Playpen Stroller Supplemental nursing system Swaddling Swim diaper Teether Travel cot Other topics Baby shower Babywearing Child neglect Closed adoption Cry room Infant ear piercing Open adoption Prenatal cocaine exposure Neonatal withdrawal syndrome Parental child abduction Parental responsibility Parenting plan Paternity Paternity fraud v t e Recreational drug use Major recreational drugs Depressants Barbiturates Benzodiazepines Carbamates Ethanol (alcohol) Alcoholic drinks Beer Wine Gabapentinoids GHB Inhalants Medical Nitrous oxide Hazardous solvents contact adhesives Gasoline nail polish remover Paint thinner Other Freon Kava Nonbenzodiazepines Quinazolinones Opioids Buprenorphine Suboxone Subutex Codeine Desomorphine Krokodil Dextropropoxyphene Darvocet Darvon Fentanyl Diamorphine Heroin Hydrocodone Hydromorphone Dilaudid Methadone Mitragyna speciosa Kratom Morphine Opium Oxycodone /paracetamol Tramadol Stimulants Amphetamine Arecoline Areca Betel Caffeine Coffee Energy drinks Tea Cathinone Khat Cocaine Coca Crack Ephedrine Ephedra MDPV Mephedrone Methamphetamine Methylone Methylphenidate Modafinil Nicotine Tobacco Theobromine Cocoa Chocolate Entactogens 2C series 6-APB Benzofury AMT MDA MDMA Ecstasy Hallucinogens Psychedelics Bufotenin Psychoactive toads Vilca Yopo DMT Ayahuasca LSA LSD-25 Mescaline Peruvian torch Peyote San Pedro Psilocybin / Psilocin Psilocybin mushrooms Dissociatives DXM Glaucine Inhalants Nitrous oxide alkyl nitrites poppers amyl nitrite Ketamine MXE Muscimol Amanita muscaria PCP Salvinorin A Salvia divinorum Deliriants Atropine and Scopolamine Atropa belladonna Datura Hyoscyamus niger Mandragora officinarum Dimenhydrinate Diphenhydramine Cannabinoids JWH-018 THC Cannabis (Marijuana) Hashish Hash oil Oneirogens Calea zacatechichi Silene capensis Club drugs Cocaine Quaaludes MDMA (Ecstasy) Nitrous oxide Poppers Drug culture Cannabis culture 420 Cannabis cultivation Cannabis smoking Head shop Legal history of cannabis in the United States Legality of cannabis Marijuana Policy Project Medical cannabis NORML Cannabis and religion Stoner film Coffee culture Coffee break Coffeehouse Latte art Tea house Drinking culture Bartending Beer culture Beer festival Binge drinking Diethyl ether Drinking games Drinking song Happy hour Hip flask Nightclub Pub Pub crawl Sommelier Sports bar Tailgate party Wine bar Wine tasting Psychedelia Psychonautics Art Drug Era Experience Literature Music Microdosing Therapy Smoking culture Cigarette card Fashion cigarettes Cloud-chasing Loosie Smokeasy Smoking fetishism Tobacco smoking Other Club drug Counterculture of the 1960s Dance party Drug paraphernalia Drug tourism Entheogen Hippie Needle sharing Nootropic Party and play Poly drug use Rave Religion and drugs Self-medication Sex and drugs Whoonga Drug production and trade Drug production Coca production in Colombia Drug precursors Opium production in Afghanistan Rolling meth lab Drug trade Illegal drug trade Colombia Darknet market Drug distribution Beer shop Cannabis shop Liquor store Liquor license Issues with drug use Abuse Date rape drug Impaired driving Drug harmfulness Effects of cannabis Addiction Dependence Prevention Opioid replacement therapy Rehabilitation Responsible use Drug-related crime Fetal alcohol spectrum disorder Long-term effects of cannabis Neurotoxicity Overdose Passive smoking of tobacco or other substances Legality of drug use International 1961 Narcotic Drugs 1971 Psychotropic Substances 1988 Drug Trafficking Council of the European Union decisions on designer drugs State level Drug policy Decriminalization Prohibition Supply reduction Policy reform Demand reduction Drug Policy Alliance Harm reduction Law Enforcement Action Partnership Liberalization Latin America Students for Sensible Drug Policy Transform Drug Policy Foundation Drug policy by country Australia Canada Germany India Netherlands Portugal Slovakia Soviet Union Sweden Switzerland United States Just Say No Office of National Drug Control Policy School district drug policies California Colorado Maryland Virginia Other Arguments for and against drug prohibition Capital punishment for drug trafficking Cognitive liberty Designer drug Drug court Drug possession Drug test Narc Politics of drug abuse War on drugs Mexican drug war Plan Colombia Philippine drug war Zero tolerance Lists of countries by... Alcohol legality Alcohol consumption Anabolic steroid legality Cannabis legality Annual use Lifetime use Cigarette consumption Cocaine legality Cocaine use Methamphetamine legality Opiates use Psilocybin mushrooms legality Salvia legality v t e Congenital malformation due to substance exposure Fetal alcohol spectrum disorder Fetal hydantoin syndrome Fetal warfarin syndrome Prenatal amphetamine exposure Prenatal cannabis exposure Prenatal cocaine exposure Prenatal nicotine exposure Other Substance use disorder v t e Psychoactive substance-related disorder General SID Substance intoxication / Drug overdose Substance-induced psychosis Withdrawal : Craving Neonatal withdrawal Post-acute-withdrawal syndrome (PAWS) SUD Substance abuse / Substance-related disord
-
Benzodiazepine Use Disorder
Wikipedia
Pronunciation: / ˌ b ɛ n z oʊ d aɪ ˈ æ z ə p iː n / Benzodiazepine List of benzodiazepines Benzodiazepine overdose Benzodiazepine dependence Benzodiazepine misuse Benzodiazepine withdrawal syndrome Effects of long-term benzodiazepine use v t e Benzodiazepine use disorder ( BUD ), also called misuse or abuse , [1] is the use of benzodiazepines without a prescription , often for recreational purposes , which poses risks of dependence , withdrawal and other long-term effects . [2] [3] Benzodiazepines are one of the more common prescription drugs used recreationally. ... However, there is only limited research into the adverse effects of benzodiazepines in drug misusers and further research is needed to demonstrate whether this is the result of cause or effect. [12] Contents 1 Signs and symptoms 1.1 Common withdrawal symptoms 1.2 Background 1.3 Health related complications 2 Risk factors 3 Epidemiology 4 Society and culture 4.1 Drug-related crime 4.2 Drug regulation and enforcement 4.2.1 Europe 4.2.2 Oceania 4.2.3 North America 4.2.4 East and Southeast Asia 5 See also 6 References 7 External links Signs and symptoms [ edit ] See also: Benzodiazepine withdrawal syndrome and Benzodiazepine dependence Benzodiazepines can induce a severe benzodiazepine withdrawal syndrome as well as drug seeking behavior . ... A high degree of tolerance often occurs in chronic benzodiazepine abusers due to the typically high doses they consume which can lead to a severe benzodiazepine dependence . The benzodiazepine withdrawal syndrome seen in chronic high dose benzodiazepine abusers is similar to that seen in therapeutic low dose users but of a more severe nature. ... The severity of the benzodiazepine withdrawal syndrome has been described by one benzodiazepine drug misuser who stated that: [14] I'd rather withdraw off heroin any day. ... External links [ edit ] Classification D ICD - 10 : F13.1 External resources eMedicine : article/290585 v t e Benzodiazepines 1,4-Benzodiazepines 2-Oxoquazepam 3-Hydroxyphenazepam Bromazepam BMS-906024 * Camazepam Carburazepam Chlordiazepoxide Cinazepam Cinolazepam Clonazepam Cloniprazepam Clorazepate Cyprazepam Delorazepam Demoxepam Desmethylflunitrazepam Devazepide * Diazepam Diclazepam Difludiazepam Doxefazepam Elfazepam Ethyl carfluzepate Ethyl dirazepate Ethyl loflazepate Flubromazepam Fletazepam Fludiazepam Flunitrazepam Flurazepam Flutemazepam Flutoprazepam Fosazepam Gidazepam Halazepam Iclazepam Irazepine Kenazepine Ketazolam Lorazepam Lormetazepam Lufuradom * Meclonazepam Medazepam Menitrazepam Metaclazepam Motrazepam N -Desalkylflurazepam Nifoxipam Nimetazepam Nitemazepam Nitrazepam Nitrazepate Nordazepam Nortetrazepam Oxazepam Phenazepam Pinazepam Pivoxazepam Prazepam Proflazepam Quazepam QH-II-66 Reclazepam RO4491533 * Ro05-4082 Ro5-4864 * SH-I-048A Sulazepam Temazepam Tetrazepam Tifluadom * Timelotem * Tolufazepam Triflunordazepam Tuclazepam Uldazepam 1,5-Benzodiazepines Arfendazam Clobazam CP-1414S Lofendazam Triflubazam 2,3-Benzodiazepines* Girisopam GYKI-52466 GYKI-52895 Nerisopam Talampanel Tofisopam Triazolobenzodiazepines Adinazolam Alprazolam Balovaptan * Bromazolam Phenazolam Rilmazolam (active metabolite of Rilmazafone ) Clonazolam Estazolam Flualprazolam Flubromazolam Flunitrazolam Nitrazolam Pyrazolam Triazolam Imidazobenzodiazepines Bretazenil Climazolam EVT-201 FG-8205 Flumazenil GL-II-73 Imidazenil 123 I-Iomazenil L-655,708 Loprazolam Midazolam PWZ-029 Remimazolam Ro15-4513 Ro48-6791 Ro48-8684 Ro4938581 Sarmazenil SH-053-R-CH3-2′F Oxazolobenzodiazepines Cloxazolam Flutazolam Haloxazolam Mexazolam Oxazolam Thienodiazepines Bentazepam Clotiazepam Thienotriazolodiazepines Brotizolam Ciclotizolam Deschloroetizolam Etizolam Fluclotizolam Israpafant * JQ1 * Metizolam Thienobenzodiazepines * Olanzapine Telenzepine Pyridodiazepines Lopirazepam Pyridotriazolodiazepines Zapizolam Pyrazolodiazepines Razobazam * Ripazepam Zolazepam Zomebazam Zometapine * Pyrrolodiazepines Premazepam Tetrahydroisoquinobenzodiazepines Clazolam Pyrrolobenzodiazepines * Anthramycin Benzodiazepine prodrugs Alprazolam triazolobenzophenone Avizafone Rilmazafone * atypical activity profile (not GABA A receptor ligands) v t e Psychoactive substance-related disorder General SID Substance intoxication / Drug overdose Substance-induced psychosis Withdrawal : Craving Neonatal withdrawal Post-acute-withdrawal syndrome (PAWS) SUD Substance abuse / Substance-related disorders Physical dependence / Psychological dependence / Substance dependence Combined substance use SUD Polysubstance dependence SID Combined drug intoxication (CDI) Alcohol SID Cardiovascular diseases Alcoholic cardiomyopathy Alcohol flush reaction (AFR) Gastrointestinal diseases Alcoholic liver disease (ALD): Alcoholic hepatitis Auto-brewery syndrome (ABS) Endocrine diseases Alcoholic ketoacidosis (AKA) Nervous system diseases Alcohol-related dementia (ARD) Alcohol intoxication Hangover Neurological disorders Alcoholic hallucinosis Alcoholic polyneuropathy Alcohol-related brain damage Alcohol withdrawal syndrome (AWS): Alcoholic hallucinosis Delirium tremens (DTs) Fetal alcohol spectrum disorder (FASD) Fetal alcohol syndrome (FAS) Korsakoff syndrome Positional alcohol nystagmus (PAN) Wernicke–Korsakoff syndrome (WKS, Korsakoff psychosis) Wernicke encephalopathy (WE) Respiratory tract diseases Alcohol-induced respiratory reactions Alcoholic lung disease SUD Alcoholism (alcohol use disorder (AUD)) Binge drinking Caffeine SID Caffeine-induced anxiety disorder Caffeine-induced sleep disorder Caffeinism SUD Caffeine dependence Cannabis SID Cannabis arteritis Cannabinoid hyperemesis syndrome (CHS) SUD Amotivational syndrome Cannabis use disorder (CUD) Synthetic cannabinoid use disorder Cocaine SID Cocaine intoxication Prenatal cocaine exposure (PCE) SUD Cocaine dependence Hallucinogen SID Acute intoxication from hallucinogens (bad trip) Hallucinogen persisting perception disorder (HPPD) Nicotine SID Nicotine poisoning Nicotine withdrawal SUD Nicotine dependence Opioids SID Opioid overdose SUD Opioid use disorder (OUD) Sedative / hypnotic SID Kindling (sedative–hypnotic withdrawal) benzodiazepine : SID Benzodiazepine overdose Benzodiazepine withdrawal SUD Benzodiazepine use disorder (BUD) Benzodiazepine dependence barbiturate : SID Barbiturate overdose SUD Barbiturate dependence Stimulants SID Stimulant psychosis amphetamine : SUD Amphetamine dependence Volatile solvent SID Sudden sniffing death syndrome (SSDS) Toluene toxicity SUD Inhalant abuse v t e Unnecessary health care Causes Direct-to-consumer advertising Overscreening Overdiagnosis Fee-for-service Defensive medicine Unwarranted variation Overmedication Over medicalization Prescription cascade Quaternary prevention Disease mongering Political abuse of psychiatry Overused health care Caesarean delivery on maternal request Antibiotic misuse Benzodiazepine use disorder Effects of long-term benzodiazepine use Opioid use disorder Psychoactive drug Proton-pump inhibitor Polypharmacy treatment of incidentaloma Tools and Situations Deprescribing Choosing Wisely Medication discontinuation Withdrawal syndrome Antidepressant discontinuation syndrome Benzodiazepine withdrawal syndrome Works about unnecessary health care Overtreated The Treatment Trap Selling Sickness Overdosed America

-
Neural Tube Defect
Wikipedia
Supplementing folic acid during pregnancy reduces the prevalence of NTDs by not exposing this otherwise sub-clinical mutation to aggravating conditions. [27] Other potential causes can include folate antimetabolites (such as methotrexate ), mycotoxins in contaminated corn meal, arsenic , hyperthermia in early development, and radiation. [28] [29] [30] Maternal obesity has also been found to be a risk factor for NTDs. [31] Studies have shown that both maternal cigarette smoking and maternal exposure to secondhand smoke increased the risk for neural tube defects in offspring. [32] A mechanism by which maternal exposure to cigarette smoke could increase NTD risk in offspring is suggested by several studies that show an association between cigarette smoking and elevations of homocysteine levels. [ citation needed ] Cigarette smoke during pregnancy, including secondhand exposure, can increase the risk of neural tube defects. [33] All of the above may act by interference with some aspect of normal folic acid metabolism and folate linked methylation related cellular processes as there are multiple genes of this type associated with neural tube defects. [34] Other [ edit ] Folic acid supplementation reduces the prevalence of neural tube defects by approximately 70% of neural tube defects indicating that 30% are not folate-dependent and are due to some cause other than alterations of methylation patterns. [35] Multiple other genes related to neural tube defects exist which are candidates for folate insensitive neural tube defects. [34] There are also several syndromes such as Meckel syndrome , and Triploid Syndrome which are frequently accompanied by neural tube defects that are assumed to be unrelated to folate metabolism [36] Diagnosis [ edit ] Tests for neural tube defects include ultrasound examination and measurement of maternal serum alpha-fetoprotein ( MSAFP ). ... Retrieved September 15, 2017 . ^ Broekman, Marike; Hoving, Eelco (2008). " " Nasal encephalocele in a child with Beckwith-Wiedemann syndrome " " . Journal of Neurosurgery . 6 (1): 485–7. doi : 10.3171/PED/2008/1/6/485 . ... "Survey of prenatal screening policies in Europe for structural malformations and chromosome anomalies, and their impact on detection and termination rates for neural tube defects and Down's syndrome" . BJOG: An International Journal of Obstetrics and Gynaecology . 115 (6): 689–696. doi : 10.1111/j.1471-0528.2008.01700.x . ... Joseph's Hospital and Medical Center Fetal Care Center Preventing Neural Tube Birth Defects: A Prevention Model and Resource Guide : Centers for Disease Control and Prevention (CDC) Classification D ICD - 10 : Q00 , Q01 , Q05 ICD - 9-CM : 740 , 741 , 742 OMIM : 182940 301410 MeSH : D009436 DiseasesDB : 8926 External resources eMedicine : neuro/244 ped/2805 v t e Congenital malformations and deformations of nervous system Brain Neural tube defect Anencephaly Acephaly Acrania Acalvaria Iniencephaly Encephalocele Chiari malformation Other Microcephaly Congenital hydrocephalus Dandy–Walker syndrome other reduction deformities Holoprosencephaly Lissencephaly Microlissencephaly Pachygyria Hydranencephaly Septo-optic dysplasia Megalencephaly Hemimegalencephaly CNS cyst Porencephaly Schizencephaly Polymicrogyria Bilateral frontoparietal polymicrogyria Spinal cord Neural tube defect Spina bifida Rachischisis Other Currarino syndrome Diastomatomyelia SyringomyeliaVANGL1, VANGL2, FUZ, MTHFD1, MTHFR, PAX3, FOLR1, GRHL3, BHMT, CECR2, FOLR2, ZIC2, PTK7, SHROOM3, ZIC5, CYP1A2, SPINT2, NAT2, CCL2, TBXT, GLI3, CSF2, INS, IFNG, GHRL, SKI, NPY1R, PRSS8, PYY, RRM1, RFC1, CDH1, AFP, PGPEP1, MTRR, MTR, PRCP, SETBP1, BMP1, CBSL, SLC19A1, CBS, TP53, MTHFD1L, PDGFRA, FOLH1, PAX1, TCN2, PARD3, SHMT1, CASP8, GLDC, TYMS, FZD3, CELSR1, UCP2, LMNB1, LRP6, IGF2, SOX3, ALDH1A2, SCRIB, ZIC3, DVL2, DHFR, COMT, CASP9, GCLC, PPARGC1A, MARCKS, ALDH1L1, MGMT, MSX2, MMUT, NFKB1, NOS2, PCMT1, TRAF4, CASP3, NOG, PRKACB, PRICKLE1, PTCH1, BMP4, SHH, TBX1, FZD6, ALX1, UGCG, CUBN, LRP2, RAB11FIP3, FOXO3, RAB23, HLA-A, F2RL2, GRHL2, MARCKSL1, EPHA4, INPP5E, DVL1, NHLRC2, H4C14, H4C8, H4C2, EED, MIR206, PTF1A, H4C5, H4C13, MIR197, FOXN1, TAGLN2, MIR129-2, MIR30B, CYP26B1, SELENOH, CUL4B, TRADD, MIRLET7G, ZGPAT, H4C3, H4C11, MALL, LST1, PERCC1, CDH23, GORASP1, CRPPA, POU5F1P4, CSRP3, DVL1P1, ARID1A, H4C9, POU5F1P3, SALL4, H4C1, H4C4, H4C6, H4C12, H4C15, TNFSF12, PCSK9, SLC19A2, PEMT, SEC24B, SLC46A1, PRRT2, WDR20, TRIM4, EMG1, CARM1, NKX2-8, CITED2, TCTN3, TXN2, TUBGCP2, SLC22A16, FKBP8, KDM2B, KCNQ1OT1, ANKRD6, DLC1, RXYLT1, WNK1, SHROOM1, SIRT1, TRPM6, NOL3, RIN2, FTO, PPIG, SUFU, DACT1, CD320, TNIP1, H4-16, LIN28A, TUBA3D, PRX, SLC40A1, KEAP1, WLS, ZEB2, GPR161, NAT1, ZIC1, GOLGA4, EZH2, FASN, FGF8, GPC5, FOXO1, FUT2, GCH1, GCKR, CBLIF, GJA1, GLI2, GNAS, CFHR1, TRDMT1, HHEX, HIF1A, HLA-B, HLA-C, HMOX1, HOXB7, HOXD@, ID1, ID2, IGF1, IL10, ITGA3, DVL3, SARDH, XPC, ATRX, ACTB, ADA, AHR, AKT2, ALX3, AMT, ANXA5, ANXA11, APAF1, APOB, SHROOM2, ASCL1, BCHE, DLX5, C5, C5AR1, CALCA, CD6, CDC25C, CLDN3, CRABP2, CTNNA1, CYP1B1, DAPK3, DDIT3, DIO3, ITGB1, ITPK1, JARID2, TERC, RELA, S100B, SALL2, CXCL6, SLC2A2, SNAI2, SMARCC1, SOX2, SULT1A1, SYT1, TCF7L2, TCN1, TFAP2A, KCNQ1, TGFB3, TGIF1, TNF, TRIP6, TUBA4A, TUBA3C, TULP3, TXN, KDM6A, VCL, WNT7B, WNT2B, MAPK8, PRKCB, PRKCA, PRKACA, KRT1, LAMC2, LEP, LEPR, LGALS1, LIFR, LIG3, MAB21L1, MAP3K5, MLH1, MRC1, ABCC1, MSH2, MUC2, MYH2, MYLK, NAP1L2, NCAM1, SEPTIN2, NFE2L2, NOS1, NOS3, POU3F1, POU5F1, PPBP, RN7SL263P
-
Temporal Lobe Epilepsy
Wikipedia
The finding of a lesion such as hippocampal sclerosis (a scar in the hippocampus), tumour, or dysplasia , on magnetic resonance imaging (MRI) predicts the intractability of seizures. [19] Personality [ edit ] Main article: Geschwind syndrome The effect of temporal lobe epilepsy on personality is a historical observation dating to the 1800s. Personality and behavioural change in temporal lobe epilepsy is seen as a chronic condition when it persists for more than three months. [20] Geschwind syndrome is a set of behavioural phenomena seen in some people with TLE. Documented by Norman Geschwind , signs include: hypergraphia (compulsion to write (or draw) excessively), hyperreligiosity (intense religious or philosophical experiences or interests), hyposexuality (reduced sexual interest or drive), circumstantiality (result of a non-linear thought pattern, talks at length about irrelevant and trivial details). [21] The personality changes generally vary by hemisphere. [21] The existence of a "temporal lobe epileptic personality" and of Geschwind syndrome have been disputed and research is inconclusive. [21] Causes [ edit ] The causes of TLE include mesial temporal sclerosis , traumatic brain injury , brain infections, such as encephalitis and meningitis , hypoxic brain injury , stroke, cerebral tumours, and genetic syndromes. ... He found a constellation of symptoms that included hypergraphia , hyperreligiosity , collapse , and pedantism , now called Geschwind syndrome . Vilayanur S. Ramachandran explored the neural basis of the hyperreligiosity seen in TLE using the galvanic skin response (GSR), which correlates with emotional arousal, to determine whether the hyperreligiosity seen in TLE was due to an overall heightened emotional state or was specific to religious stimuli. ... Patients with mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS) had significantly higher SSRS scores than those with other epileptic syndromes and, than in individuals of the CG (control Group) ^ d'Orsi, Giuseppe; Tinuper, Paolo (2006). " " I heard voicesGRM1, NPY, GRM5, SLC12A5, VDR, P2RX7, KDR, SLC12A2, TRPV1, SLIT2, SLC1A1, NPY2R, GRM2, TEK, BDKRB1, BDKRB2, COX3, P2RX4, VEGFA, KCNC4, CNR1, GRM4, GRM3, ABCB1, MTOR, NTRK2, RGMA, NSF, NOS1, CXCR4, GLUL, HCN1, ADK, AGT, DTNBP1, FYN, GLUD1, GRIK5, PRICKLE1, DLG4, KCNA1, SHH, CYFIP1, CABP1, MAP2, MBP, VDAC2, SLC6A1, PTPRZ1, ACTB, ADD1, DBN1, CDC42, CRH, CACNA1A, AK2, CRHBP, AVP, APOE, LGI1, GABBR1, BDNF, IL1B, SLC6A4, SLC1A2, MIR146A, MIR155, PDYN, PVALB, AQP4, STIN2-VNTR, PRNP, SMUG1, TNF, RELN, TLR4, HTR1A, GRIA2, TBC1D9, GRIN2A, CPA6, GFAP, GRIN1, GPHN, TSPO, SST, SOD1, HSPA4, APP, OPRM1, SCN2A, HTR2A, AIF1, AZGP1, IL1RN, BCL2, JRK, ACE, GAL, KCNJ10, SCN1A, CALB1, S100B, ZFYVE9, CNTNAP2, MAOA, MAPK8, CASP3, MMP9, ADAM10, KLK8, NFE2L2, TRPV4, SCN8A, MIR134, MAPK14, ENO2, MIR23A, F2R, CALHM1, MIR21, DNMT1, GRIN2B, GABRB3, DNMT3A, MIRLET7B, CFH, DCX, FLT4, GRIA1, ADIPOQ, MIR34A, MIR139, TNFRSF10A, HAP1, GNA14, APOBEC1, DEPDC5, MIR204, KEAP1, GRAP2, GABBR2, CDYL, MIR221, GAB2, BIN1, TNFSF10, MIR222, DUSP26, MIR331, IRS2, TNFRSF1A, TP53, LOC110806262, TXNRD1, ATP1A2, AQP9, GATD3B, PGR-AS1, VEGFC, MICA, FTX, MIR1260A, MIR1183, C20orf181, AIMP2, GLRA3, MLRL, GATD3A, DOC2A, SEMA7A, CCR2, MIR451A, CASP8AP2, PDE5A, MIRLET7C, TUBB3, MIR132, KCNMB4, SLC46A1, KCNH7, ZDHHC8, UBQLN1, ATL1, WNT3A, SHANK3, SUCO, PEX5L, RBFOX1, PAG1, RETN, EFCAB2, AGTR2, RTN4, SNX25, TLN2, SOX7, SEMA6A, DHX40, SRR, MICAL1, TNFRSF13C, GLS2, RNU1-1, OPN5, WNK3, FAM3C, CXCL13, AHSA1, TNFSF13B, PDE10A, NWD1, NEAT1, ACOT7, NLRP1, MAPK8IP3, SPAG8, AKT1, VPS13A, SMG6, ADRA2A, PADI4, RSS, TPH2, PANX1, RNF19A, POLDIP2, DROSHA, DBP, TLR2, NRG1, CYBB, CTSD, GRIA3, GRN, GRIK1, GRIK2, CTSB, NR3C1, CSF2, CRP, CRK, GSK3B, HDAC2, HIF1A, CDX2, HRC, HES1, HSP90AB1, HTC2, ICAM1, IGF1, IL1A, IL2, IL7, CXCR2, IL13, IL17A, IL18, GLP1R, GJA1, GHRH, GAPDH, DECR1, DFFB, TIMM8A, DNM1, DNAH8, DPYSL2, DSCAM, EGR1, EGR2, EIF2S1, EIF4EBP1, EPHA4, EPHX2, ESR1, FEB1, FEB2, FHL2, FOXO3, FOLR1, DAPK1, DAP, GABRA1, GABRA2, GABRA5, GABRB2, GAD1, GAD2, IRS1, KCND2, THOP1, SCNN1D, MAPK1, MAPK10, PSEN2, PTGS2, PTPN11, CXCR5, REN, UPF1, RRBP1, S100A1, SC5D, SCN1B, SCN7A, CCL3, KCNE1, CCL4, CXCL12, SELP, SELENOW, SH3GL2, HCN2, SLC6A9, SLC16A1, SMS, SOX2, SPAST, SRF, SSTR2, PRKG2, PLD2, PLD1, PLAT, KCNJ9, KCNQ3, KLK1, KLKB1, KNG1, LAMC2, LEP, LETM1, SMAD3, CCK, MAPT, MDM2, MECP2, MGAT1, MMP3, MPO, MST1, CASP1, MYD88, CAST, NPY1R, C3, SERPING1, OPRL1, BTN1A1, PRDX1, SERPINE1, LINC02605

-
Gastroenteritis
Wikipedia
Specialty Infectious disease Symptoms Diarrhea , vomiting , abdominal pain, fever [1] [2] Complications Dehydration [2] [3] Causes Viruses , bacteria , parasites , fungus [2] [4] Diagnostic method Based on symptoms, occasionally stool culture [2] Differential diagnosis Inflammatory bowel disease , malabsorption syndrome , lactose intolerance [5] Prevention Hand washing , drinking clean water , proper disposal of human waste , breastfeeding [2] Treatment Oral rehydration solution (combination of water, salts, and sugar), intravenous fluids [2] Frequency 2.4 billion (2015) [6] Deaths 1.3 million (2015) [7] Gastroenteritis , also known as infectious diarrhea and gastro , is inflammation of the gastrointestinal tract —the stomach and intestine . [8] Symptoms may include diarrhea , vomiting and abdominal pain . [1] Fever , lack of energy and dehydration may also occur. [2] [3] This typically lasts less than two weeks. [8] It is not related to influenza , though it has erroneously been called the " stomach flu ". [9] Gastroenteritis is usually caused by viruses . [4] However, bacteria , parasites , and fungus can also cause gastroenteritis. [2] [4] In children, rotavirus is the most common cause of severe disease. [10] In adults, norovirus and Campylobacter are common causes. [11] [12] Eating improperly prepared food, drinking contaminated water or close contact with a person who is infected can spread the disease. [2] Treatment is generally the same with or without a definitive diagnosis, so testing to confirm is usually not needed. [2] Prevention includes hand washing with soap, drinking clean water , breastfeeding babies instead of using formula [2] and proper disposal of human waste . The rotavirus vaccine is recommended as a prevention for children. [2] [10] Treatment involves getting enough fluids. [2] For mild or moderate cases, this can typically be achieved by drinking oral rehydration solution (a combination of water, salts and sugar). [2] In those who are breastfed, continued breastfeeding is recommended. [2] For more severe cases, intravenous fluids may be needed. [2] Fluids may also be given by a nasogastric tube . [13] Zinc supplementation is recommended in children. [2] Antibiotics are generally not needed. [14] However, antibiotics are recommended for young children with a fever and bloody diarrhea. [1] In 2015, there were two billion cases of gastroenteritis, resulting in 1.3 million deaths globally. [6] [7] Children and those in the developing world are affected the most. [15] In 2011, there were about 1.7 billion cases, resulting in about 700,000 deaths of children under the age of five. [16] In the developing world, children less than two years of age frequently get six or more infections a year. [17] It is less common in adults, partly due to the development of immunity . [18] Contents 1 Signs and symptoms 2 Cause 2.1 Viral 2.2 Bacterial 2.3 Parasitic 2.4 Transmission 2.5 Non-infectious 3 Pathophysiology 4 Diagnosis 4.1 Dehydration 4.2 Differential diagnosis 5 Prevention 5.1 Lifestyle 5.2 Vaccination 6 Management 6.1 Rehydration 6.2 Dietary 6.3 Antiemetics 6.4 Antibiotics 6.5 Antimotility agents 7 Epidemiology 8 History 9 Society and culture 10 Research 11 Other animals 12 References 12.1 Notes 13 External links Signs and symptoms [ edit ] Bristol stool chart Gastroenteritis usually involves both diarrhea and vomiting . [18] Sometimes, only one or the other is present. [1] This may be accompanied by abdominal cramps. [1] Signs and symptoms usually begin 12–72 hours after contracting the infectious agent. [15] If due to a virus, the condition usually resolves within one week. [18] Some viral infections also involve fever , fatigue, headache and muscle pain . [18] If the stool is bloody , the cause is less likely to be viral [18] and more likely to be bacterial. [19] Some bacterial infections cause severe abdominal pain and may persist for several weeks. [19] Children infected with rotavirus usually make a full recovery within three to eight days. [20] However, in poor countries treatment for severe infections is often out of reach and persistent diarrhea is common. [21] Dehydration is a common complication of diarrhea . [22] Severe dehydration in children may be recognized if the skin color and position returns slowly when pressed. [23] This is called "prolonged capillary refill " and "poor skin turgor ". [23] Abnormal breathing is another sign of severe dehydration. [23] Repeat infections are typically seen in areas with poor sanitation, and malnutrition . [15] Stunted growth and long-term cognitive delays can result. [17] Reactive arthritis occurs in 1% of people following infections with Campylobacter species. [19] Guillain–Barré syndrome occurs in 0.1%. [19] Hemolytic uremic syndrome (HUS) may occur due to infection with Shiga toxin -producing Escherichia coli or Shigella species. [24] HUS causes low platelet counts , poor kidney function , and low red blood cell count (due to their breakdown) . [24] Children are more predisposed to getting HUS than adults. [17] Some viral infections may produce benign infantile seizures . [1] Cause [ edit ] Viruses (particularly rotavirus ) and the bacteria Escherichia coli and Campylobacter species are the primary causes of gastroenteritis. [15] [25] There are, however, many other infectious agents that can cause this syndrome including parasites and fungus . [17] [4] Non-infectious causes are seen on occasion, but they are less likely than a viral or bacterial cause. [1] Risk of infection is higher in children due to their lack of immunity . [1] Children are also at higher risk because they are less likely to practice good hygiene habits. [1] Children living in areas without easy access to water and soap are especially vulnerable. [1] Viral [ edit ] Rotavirus , norovirus , adenovirus , and astrovirus are known to cause viral gastroenteritis . [18] [26] Rotavirus is the most common cause of gastroenteritis in children, [25] and produces similar rates in both the developed and developing world . [20] Viruses cause about 70% of episodes of infectious diarrhea in the pediatric age group. [13] Rotavirus is a less common cause in adults due to acquired immunity. [27] Norovirus is the cause in about 18% of all cases. [28] Generally speaking, viral gastroenteritis accounts for 21%-40% of the cases of infectious diarrhea in developed countries. [29] Norovirus is the leading cause of gastroenteritis among adults in America accounting for about 90% of viral gastroenteritis outbreaks. [18] These localized epidemics typically occur when groups of people spend time in close physical proximity to each other, such as on cruise ships , [18] in hospitals, and in restaurants. [1] People may remain infectious even after their diarrhea has ended. [18] Norovirus is the cause of about 10% of cases in children. [1] Bacterial [ edit ] Salmonella enterica serovar Typhimurium (ATCC 14028) as seen with a microscope at 1000 fold magnification and following Gram staining. ... Of the twenty most common conditions seen in the emergency department, rates of noninfectious gastroenteritis had the largest decrease in visits in that time period. [39] Pathophysiology [ edit ] Gastroenteritis is defined as vomiting or diarrhea due to inflammation of the small or large bowel , often due to infection. [17] The changes in the small bowel are typically noninflammatory, while the ones in the large bowel are inflammatory. [17] The number of pathogens required to cause an infection varies from as few as one (for Cryptosporidium ) to as many as 10 8 (for Vibrio cholerae ). [17] Diagnosis [ edit ] Gastroenteritis is typically diagnosed clinically, based on a person's signs and symptoms. [18] Determining the exact cause is usually not needed as it does not alter management of the condition. [15] However, stool cultures should be performed in those with blood in the stool, those who might have been exposed to food poisoning , and those who have recently traveled to the developing world. [13] It may also be appropriate in children younger than 5, old people, and those with poor immune function. [40] Diagnostic testing may also be done for surveillance. [18] As hypoglycemia occurs in approximately 10% of infants and young children, measuring serum glucose in this population is recommended. [23] Electrolytes and kidney function should also be checked when there is a concern about severe dehydration. [13] Dehydration [ edit ] A determination of whether or not the person has dehydration is an important part of the assessment, with dehydration typically divided into mild (3–5%), moderate (6–9%), and severe (≥10%) cases. [1] In children, the most accurate signs of moderate or severe dehydration are a prolonged capillary refill , poor skin turgor , and abnormal breathing. [23] [41] Other useful findings (when used in combination) include sunken eyes, decreased activity, a lack of tears, and a dry mouth. [1] A normal urinary output and oral fluid intake is reassuring. [23] Laboratory testing is of little clinical benefit in determining the degree of dehydration. [1] Thus the use of urine testing or ultrasounds is generally not needed. [42] Differential diagnosis [ edit ] Other potential causes of signs and symptoms that mimic those seen in gastroenteritis that need to be ruled out include appendicitis , volvulus , inflammatory bowel disease , urinary tract infections , and diabetes mellitus . [13] Pancreatic insufficiency, short bowel syndrome , Whipple's disease , coeliac disease , and laxative abuse should also be considered. [43] The differential diagnosis can be complicated somewhat if the person exhibits only vomiting or diarrhea (rather than both). [1] Appendicitis may present with vomiting, abdominal pain, and a small amount of diarrhea in up to 33% of cases. [1] This is in contrast to the large amount of diarrhea that is typical of gastroenteritis. [1] Infections of the lungs or urinary tract in children may also cause vomiting or diarrhea. [1] Classical diabetic ketoacidosis (DKA) presents with abdominal pain, nausea, and vomiting, but without diarrhea. [1] One study found that 17% of children with DKA were initially diagnosed as having gastroenteritis. [1] Prevention [ edit ] Percentage of rotavirus tests with positive results, by surveillance week, United States, July 2000 – June 2009. ... Classification D ICD - 10 : A02.0 , A08 , A09 , J10.8 , J11.8 , K52 ICD - 9-CM : 008.8 009.0 , 009.1 , 558 MeSH : D005759 DiseasesDB : 30726 External resources MedlinePlus : 000252 eMedicine : emerg/213 v t e Diseases of the digestive system Upper GI tract Esophagus Esophagitis Candidal Eosinophilic Herpetiform Rupture Boerhaave syndrome Mallory–Weiss syndrome UES Zenker's diverticulum LES Barrett's esophagus Esophageal motility disorder Nutcracker esophagus Achalasia Diffuse esophageal spasm Gastroesophageal reflux disease (GERD) Laryngopharyngeal reflux (LPR) Esophageal stricture Megaesophagus Esophageal intramural pseudodiverticulosis Stomach Gastritis Atrophic Ménétrier's disease Gastroenteritis Peptic (gastric) ulcer Cushing ulcer Dieulafoy's lesion Dyspepsia Pyloric stenosis Achlorhydria Gastroparesis Gastroptosis Portal hypertensive gastropathy Gastric antral vascular ectasia Gastric dumping syndrome Gastric volvulus Buried bumper syndrome Gastrinoma Zollinger–Ellison syndrome Lower GI tract Enteropathy Small intestine ( Duodenum / Jejunum / Ileum ) Enteritis Duodenitis Jejunitis Ileitis Peptic (duodenal) ulcer Curling's ulcer Malabsorption : Coeliac Tropical sprue Blind loop syndrome Small bowel bacterial overgrowth syndrome Whipple's Short bowel syndrome Steatorrhea Milroy disease Bile acid malabsorption Large intestine ( Appendix / Colon ) Appendicitis Colitis Pseudomembranous Ulcerative Ischemic Microscopic Collagenous Lymphocytic Functional colonic disease IBS Intestinal pseudoobstruction / Ogilvie syndrome Megacolon / Toxic megacolon Diverticulitis / Diverticulosis / SCAD Large and/or small Enterocolitis Necrotizing Gastroenterocolitis IBD Crohn's disease Vascular : Abdominal angina Mesenteric ischemia Angiodysplasia Bowel obstruction : Ileus Intussusception Volvulus Fecal impaction Constipation Diarrhea Infectious Intestinal adhesions Rectum Proctitis Radiation proctitis Proctalgia fugax Rectal prolapse Anismus Anal canal Anal fissure / Anal fistula Anal abscess Hemorrhoid Anal dysplasia Pruritus ani GI bleeding Blood in stool Upper Hematemesis Melena Lower Hematochezia Accessory Liver Hepatitis Viral hepatitis Autoimmune hepatitis Alcoholic hepatitis Cirrhosis PBC Fatty liver NASH Vascular Budd–Chiari syndrome Hepatic veno-occlusive disease Portal hypertension Nutmeg liver Alcoholic liver disease Liver failure Hepatic encephalopathy Acute liver failure Liver abscess Pyogenic Amoebic Hepatorenal syndrome Peliosis hepatis Metabolic disorders Wilson's disease Hemochromatosis Gallbladder Cholecystitis Gallstone / Cholelithiasis Cholesterolosis Adenomyomatosis Postcholecystectomy syndrome Porcelain gallbladder Bile duct / Other biliary tree Cholangitis Primary sclerosing cholangitis Secondary sclerosing cholangitis Ascending Cholestasis / Mirizzi's syndrome Biliary fistula Haemobilia Common bile duct Choledocholithiasis Biliary dyskinesia Sphincter of Oddi dysfunction Pancreatic Pancreatitis Acute Chronic Hereditary Pancreatic abscess Pancreatic pseudocyst Exocrine pancreatic insufficiency Pancreatic fistula Other Hernia Diaphragmatic Congenital Hiatus Inguinal Indirect Direct Umbilical Femoral Obturator Spigelian Lumbar Petit's Grynfeltt-Lesshaft Undefined location Incisional Internal hernia Richter's Peritoneal Peritonitis Spontaneous bacterial peritonitis Hemoperitoneum Pneumoperitoneum v t e Infectious diseases – viral systemic diseases Oncovirus DNA virus HBV Hepatocellular carcinoma HPV Cervical cancer Anal cancer Penile cancer Vulvar cancer Vaginal cancer Oropharyngeal cancer KSHV Kaposi's sarcoma EBV Nasopharyngeal carcinoma Burkitt's lymphoma Hodgkin lymphoma Follicular dendritic cell sarcoma Extranodal NK/T-cell lymphoma, nasal type MCPyV Merkel-cell carcinoma RNA virus HCV Hepatocellular carcinoma Splenic marginal zone lymphoma HTLV-I Adult T-cell leukemia/lyF2RL1, ANPEP, CDK2AP1, PRSS57, CAT, AHI1, NCKIPSD, BCAR3, IFNG, MAPK1, RTN2, AIMP2, RIDA, GRAP2, IFNA13, AHSA1, RNF19A, POLDIP2, PRRT2, IFNB1, SLC5A2, IFNA1, EGFR, CRK, MAPK14, ERICD, IL17A, PABPC1, PDP1, CDSN, IL22, SIGLEC8, LAMP3, ACAD8, CPE, IRF3, CFH, ATF6, CRP, IL1RAP, SH2D3C, EIF2AK3, CDC42, SARS2, MARCHF1, ATG16L1, CCDC88A, ENAH, GORASP1, NBEAL1, WNK1, ATP4A, PGLYRP3, ASZ1, ZBTB46, PLB1, IRGM, ATP12A, MIR222, DDX1, IL6, PLA2G6, RPL10, KRT10, LPA, LSAMP, MME, NM, CCN3, PLA2G1B, PLA2G2A, PLXNA1, CTSA, CBLIF, MAPK8, RB1, RELA, FUT2, ST8SIA2, SARS1, SCN1A, SCN1B, APOH, SLC5A5, SPI1, SYT1, TFRC, TNF, VTN, XBP1, YWHAZ, ERN1, IFN1@, STX2

-
Infantile Hemangioma
Wikipedia
Infantile hemangioma Other names Infantile haemangioma, emangioma, capillary hemangioma, capillary angioma, juvenile [1] A small hemangioma of infancy Specialty Dermatology , gastroenterology , Oral and Maxillofacial Surgery Symptoms Raised red or blue lesion [2] Complications Pain, bleeding, ulcer formation, heart failure , disfigurement [1] Usual onset First 4 weeks of life [1] Types Superficial, deep, mixed [1] Risk factors Females, white people , preemies , low birth weight babies [1] Diagnostic method Based on symptoms and appearance [1] Differential diagnosis Congenital hemangioma , pyogenic granuloma , kaposiform hemangioendothelioma , tufted angioma , venous malformation [1] Treatment Close observation, medication [3] [1] Medication Propranolol , Timolol , steroids [3] [1] Frequency Up to 5% [3] An infantile hemangioma ( IH ) is a type of benign vascular tumor that affects babies. [1] They appear as a red or blue raised lesion . [2] Typically they begin during the first four weeks of life, grow until about five months of life, and then shrink in size over the next few years. [1] Often skin changes remain following involution. [1] [3] Complications may include pain, bleeding, ulcer formation, heart failure , or disfigurement . [1] The underlying reason for their occurrence is not clear. [1] In about 10% of cases they appear to run in families. [1] A few cases are associated with other abnormalities such as PHACE syndrome . [1] Diagnosis is generally based on the symptoms and appearance. [1] Occasionally medical imaging can assist in the diagnosis. [1] In most cases no treatment is needed, other than close observation. [3] [1] Certain cases, however, may result in problems and the use of medication such as propranolol or steroids are recommended. [3] [1] Occasionally surgery or laser treatment may be used. [1] It is one of the most common benign tumors in babies, occurring in about 5%. [3] [1] They occur more frequently in females, white people , preemies , and low birth weight babies. [1] The word "hemangioma" comes from the Greek haima (αἷμα) meaning "blood"; angeion (ἀγγεῖον) meaning "vessel"; and -oma (-ωμα) meaning "tumor". [4] Contents 1 Signs and symptoms 1.1 Complications 2 Causes 3 Diagnosis 4 Treatment 4.1 Medication 4.2 Surgery 4.3 Laser 5 Prognosis 6 Terminology 7 References 8 External links Signs and symptoms [ edit ] A flat hemangioma in a baby A resolving hemangioma Infantile hemangioma, well-circumscribed red, violet, exophytic vascular tumor on the nose of a one-year-old child [5] Infantile hemangiomas typically develop in the first few weeks or months of life. [6] They are more common in Caucasians , in premature children whose birth weight is less than 3 pounds (1.4 kg), in females, and in twin births. [7] Early lesions may resemble a red scratch or patch, a white patch, or a bruise. ... Large segmental hemangiomas of the head and neck can be associated with a disorder called PHACES syndrome . [12] [13] Large segmental hemangiomas over the lumbar spine can be associated with dysraphism, renal, and urogenital problems in association with a disorder called LUMBAR syndrome. ... For example, a patient with a large facial hemangioma who is found to meet criteria for PHACE syndrome will require potentially ongoing neurologic, cardiac, and/or ophthalmologic monitoring. ... "The cerebral vasculopathy of PHACES syndrome" . Stroke . 39 (2): 308–16. doi : 10.1161/strokeaha.107.485185 . ... CS1 maint: multiple names: authors list ( link ) External links [ edit ] Classification D ICD - 10 : D18.0 ( ILDS D18.010) ICD - 9-CM : 228.0 ICD-O : M9120/0 MeSH : D006391 DiseasesDB : 30033 External resources MedlinePlus : 001459 eMedicine : derm/201 v t e Diseases of the skin and appendages by morphology Growths Epidermal Wart Callus Seborrheic keratosis Acrochordon Molluscum contagiosum Actinic keratosis Squamous-cell carcinoma Basal-cell carcinoma Merkel-cell carcinoma Nevus sebaceous Trichoepithelioma Pigmented Freckles Lentigo Melasma Nevus Melanoma Dermal and subcutaneous Epidermal inclusion cyst Hemangioma Dermatofibroma (benign fibrous histiocytoma) Keloid Lipoma Neurofibroma Xanthoma Kaposi's sarcoma Infantile digital fibromatosis Granular cell tumor Leiomyoma Lymphangioma circumscriptum Myxoid cyst Rashes With epidermal involvement Eczematous Contact dermatitis Atopic dermatitis Seborrheic dermatitis Stasis dermatitis Lichen simplex chronicus Darier's disease Glucagonoma syndrome Langerhans cell histiocytosis Lichen sclerosus Pemphigus foliaceus Wiskott–Aldrich syndrome Zinc deficiency Scaling Psoriasis Tinea ( Corporis Cruris Pedis Manuum Faciei ) Pityriasis rosea Secondary syphilis Mycosis fungoides Systemic lupus erythematosus Pityriasis rubra pilaris Parapsoriasis Ichthyosis Blistering Herpes simplex Herpes zoster Varicella Bullous impetigo Acute contact dermatitis Pemphigus vulgaris Bullous pemphigoid Dermatitis herpetiformis Porphyria cutanea tarda Epidermolysis bullosa simplex Papular Scabies Insect bite reactions Lichen planus Miliaria Keratosis pilaris Lichen spinulosus Transient acantholytic dermatosis Lichen nitidus Pityriasis lichenoides et varioliformis acuta Pustular Acne vulgaris Acne rosacea Folliculitis Impetigo Candidiasis Gonococcemia Dermatophyte Coccidioidomycosis Subcorneal pustular dermatosis Hypopigmented Tinea versicolor Vitiligo Pityriasis alba Postinflammatory hyperpigmentation Tuberous sclerosis Idiopathic guttate hypomelanosis Leprosy Hypopigmented mycosis fungoides Without epidermal involvement Red Blanchable Erythema Generalized Drug eruptions Viral exanthems Toxic erythema Systemic lupus erythematosus Localized Cellulitis Abscess Boil Erythema nodosum Carcinoid syndrome Fixed drug eruption Specialized Urticaria Erythema ( Multiforme Migrans Gyratum repens Annulare centrifugum Ab igne ) Nonblanchable Purpura Macular Thrombocytopenic purpura Actinic/solar purpura Papular Disseminated intravascular coagulation Vasculitis Indurated Scleroderma / morphea Granuloma annulare Lichen sclerosis et atrophicus Necrobiosis lipoidica Miscellaneous disorders Ulcers Hair Telogen effluvium Androgenic alopecia Alopecia areata Systemic lupus erythematosus Tinea capitis Loose anagen syndrome Lichen planopilaris Folliculitis decalvans Acne keloidalis nuchae Nail Onychomycosis Psoriasis Paronychia Ingrown nail Mucous membrane Aphthous stomatitis Oral candidiasis Lichen planus Leukoplakia Pemphigus vulgaris Mucous membrane pemphigoid Cicatricial pemphigoid Herpesvirus Coxsackievirus Syphilis Systemic histoplasmosis Squamous-cell carcinoma v t e Tumours of blood vessels Blood vessel Hemangiosarcoma Blue rubber bleb nevus syndrome Hemangioendothelioma Composite Endovascular papillary Epithelioid Kaposiform Infantile Retiform ) Spindle cell Proliferating angioendotheliomatosis Hemangiopericytoma Venous lake Kaposi's sarcoma African cutaneous African lymphadenopathic AIDS-associated Classic Immunosuppression-associated Hemangioblastoma Hemangioma Capillary Cavernous Glomeruloid Microvenular Targeted hemosiderotic Angioma Cherry Seriginosum Spider Tufted Universal angiomatosis Angiokeratoma of Mibelli Angiolipoma Pyogenic granuloma Lymphatic Lymphangioma / lymphangiosarcoma Lymphangioma circumscriptum Acquired progressive lymphangioma PEComa Lymphangioleiomyomatosis Cystic hygroma Multifocal lymphangioendotheliomatosis Lymphangiomatosis Either Angioma / angiosarcoma Angiofibroma

-
Multiple Sclerosis
Wikipedia
Specialty Neurology Symptoms Double vision, blindness in one eye, muscle weakness, trouble with sensation , trouble with coordination [1] Usual onset Age 20–50 [2] Duration Long term [1] Causes Unknown [3] Diagnostic method Based on symptoms and medical tests [4] Treatment Medications, physical therapy [1] Prognosis 5–10 year shorter life expectancy [5] Frequency 2 million (2015) [6] Deaths 18,900 (2015) [7] Multiple sclerosis ( MS ), also known as encephalomyelitis disseminata , is a demyelinating disease in which the insulating covers of nerve cells in the brain and spinal cord are damaged. [1] This damage disrupts the ability of parts of the nervous system to transmit signals , resulting in a range of signs and symptoms , including physical, mental , and sometimes psychiatric problems. [5] [8] [9] Specific symptoms can include double vision , blindness in one eye, muscle weakness and trouble with sensation or coordination. [1] MS takes several forms, with new symptoms either occurring in isolated attacks (relapsing forms) or building up over time (progressive forms). [10] [11] Between attacks, symptoms may disappear completely; however, permanent neurological problems often remain, especially as the disease advances. [11] While the cause is unclear, the underlying mechanism is thought to be either destruction by the immune system or failure of the myelin -producing cells. [3] Proposed causes for this include genetics and environmental factors being triggered by a viral infection . [8] [12] MS is usually diagnosed based on the presenting signs and symptoms and the results of supporting medical tests. [4] There is no known cure for multiple sclerosis. [1] Treatments attempt to improve function after an attack and prevent new attacks. [8] Medications used to treat MS, while modestly effective, can have side effects and be poorly tolerated. [1] Physical therapy can help with people's ability to function. [1] Many people pursue alternative treatments , despite a lack of evidence of benefit. [13] The long-term outcome is difficult to predict; good outcomes are more often seen in women, those who develop the disease early in life, those with a relapsing course, and those who initially experienced few attacks. [14] Life expectancy is on average five to ten years lower than that of the unaffected population. [5] Multiple sclerosis is the most common immune-mediated disorder affecting the central nervous system . [15] In 2015, about 2.3 million people were affected globally, with rates varying widely in different regions and among different populations. [6] [16] In that year, about 18,900 people died from MS, up from 12,000 in 1990. [7] [17] The disease usually begins between the ages of twenty and fifty and is twice as common in women as in men. [2] MS was first described in 1868 by French neurologist Jean-Martin Charcot . [18] The name multiple sclerosis refers to the numerous glial scars (or sclerae – essentially plaques or lesions) that develop on the white matter of the brain and spinal cord. [18] A number of new treatments and diagnostic methods are under development. [19] Contents 1 Signs and symptoms 2 Causes 2.1 Geography 2.2 Genetics 2.3 Infectious agents 2.4 Other 3 Pathophysiology 3.1 Lesions 3.2 Inflammation 3.3 Blood–brain barrier 4 Diagnosis 5 Types and variants 5.1 Special courses 5.2 Variants 6 Management 6.1 Acute attacks 6.2 Disease-modifying treatments 6.2.1 Relapsing remitting multiple sclerosis 6.2.2 Progressive multiple sclerosis 6.2.3 Adverse effects 6.3 Associated symptoms 6.4 Alternative treatments 7 Prognosis 8 Epidemiology 9 History 9.1 Medical discovery 9.2 Diagnosis history 9.3 Historical cases 10 Research 10.1 Medications 10.2 Pathogenesis 10.3 Disease biomarkers 10.4 Chronic cerebrospinal venous insufficiency 11 See also 12 References 13 Further reading 14 External links Signs and symptoms Main article: Multiple sclerosis signs and symptoms Main symptoms of multiple sclerosis A person with MS can have almost any neurological symptom or sign, with autonomic , visual, motor, and sensory problems being the most common. [5] The specific symptoms are determined by the locations of the lesions within the nervous system, and may include loss of sensitivity or changes in sensation such as tingling, pins and needles or numbness, muscle weakness, blurred vision , [20] very pronounced reflexes , muscle spasms , or difficulty in moving; difficulties with coordination and balance ( ataxia ); problems with speech or swallowing , visual problems ( nystagmus , optic neuritis or double vision ), feeling tired , acute or chronic pain , and bladder and bowel difficulties (such as neurogenic bladder ), among others. [5] Difficulties thinking and emotional problems such as depression or unstable mood are also common. [5] Uhthoff's phenomenon , a worsening of symptoms due to exposure to higher than usual temperatures, and Lhermitte's sign , an electrical sensation that runs down the back when bending the neck, are particularly characteristic of MS. [5] The main measure of disability and severity is the expanded disability status scale (EDSS), with other measures such as the multiple sclerosis functional composite being increasingly used in research. [21] [22] [23] The condition begins in 85% of cases as a clinically isolated syndrome (CIS) over a number of days with 45% having motor or sensory problems, 20% having optic neuritis , and 10% having symptoms related to brainstem dysfunction, while the remaining 25% have more than one of the previous difficulties. [4] The course of symptoms occurs in two main patterns initially: either as episodes of sudden worsening that last a few days to months (called relapses , exacerbations, bouts, attacks, or flare-ups) followed by improvement (85% of cases) or as a gradual worsening over time without periods of recovery (10–15% of cases). [2] A combination of these two patterns may also occur [11] or people may start in a relapsing and remitting course that then becomes progressive later on. [2] Relapses are usually not predictable, occurring without warning. [5] Exacerbations rarely occur more frequently than twice per year. [5] Some relapses, however, are preceded by common triggers and they occur more frequently during spring and summer. [24] Similarly, viral infections such as the common cold , influenza , or gastroenteritis increase their risk. [5] Stress may also trigger an attack. [25] Women with MS who become pregnant experience fewer relapses; however, during the first months after delivery the risk increases. [5] Overall, pregnancy does not seem to influence long-term disability. [5] Many events have been found not to affect relapse rates including vaccination , breast feeding , [5] physical trauma, [26] and Uhthoff's phenomenon . [24] Causes The cause of MS is unknown; however, it is believed to occur as a result of some combination of genetic and environmental factors such as infectious agents. [5] Theories try to combine the data into likely explanations, but none has proved definitive. ... Currently, the United States National Multiple Sclerosis Society and the Multiple Sclerosis International Federation , describes four types of MS (revised in 2013): [56] [57] [58] Clinically isolated syndrome (CIS) Relapsing-remitting MS (RRMS) Primary progressive MS (PPMS) Secondary progressive MS (SPMS) Relapsing-remitting MS is characterized by unpredictable relapses followed by periods of months to years of relative quiet ( remission ) with no new signs of disease activity. Deficits that occur during attacks may either resolve or leave problems , the latter in about 40% of attacks and being more common the longer a person has had the disease. [5] [4] This describes the initial course of 80% of individuals with MS. [5] The relapsing-remitting subtype usually begins with a clinically isolated syndrome (CIS). In CIS, a person has an attack suggestive of demyelination, but does not fulfill the criteria for multiple sclerosis. [5] [59] 30 to 70% of persons who experience CIS, later develop MS. [59] Primary progressive MS occurs in approximately 10–20% of individuals, with no remission after the initial symptoms. [4] [60] It is characterized by progression of disability from onset, with no, or only occasional and minor, remissions and improvements. [11] The usual age of onset for the primary progressive subtype is later than of the relapsing-remitting subtype. ... They are interferon beta-1a , interferon beta-1b , [74] glatiramer acetate , mitoxantrone , natalizumab , [75] fingolimod , [76] teriflunomide , [77] [78] dimethyl fumarate , [79] [80] alemtuzumab , [81] [82] ocrelizumab , [83] [84] siponimod , [84] [85] [86] cladribine , [84] [87] and ozanimod . [88] [89] [90] Their cost effectiveness as of 2012 is unclear. [91] In March 2017, the FDA approved ocrelizumab , a humanized anti- CD20 monoclonal antibody , as a treatment for RRMS, [92] [93] with requirements for several Phase IV clinical trials. [94] In RRMS they are modestly effective at decreasing the number of attacks. [77] The interferons [74] and glatiramer acetate are first-line treatments [4] and are roughly equivalent, reducing relapses by approximately 30%. [95] Early-initiated long-term therapy is safe and improves outcomes. [96] [97] Natalizumab reduces the relapse rate more than first-line agents; however, due to issues of adverse effects is a second-line agent reserved for those who do not respond to other treatments [4] or with severe disease. [95] [75] Mitoxantrone, whose use is limited by severe adverse effects, is a third-line option for those who do not respond to other medications. [4] Treatment of clinically isolated syndrome (CIS) with interferons decreases the chance of progressing to clinical MS. [5] [98] [99] Efficacy of interferons and glatiramer acetate in children has been estimated to be roughly equivalent to that of adults. [100] The role of some newer agents such as fingolimod, [76] teriflunomide, and dimethyl fumarate, [79] is not yet entirely clear. [101] It is difficult to make firm conclusions about the best treatment, especially regarding the long‐term benefit and safety of early treatment, given the lack of studies directly comparing disease modifying therapies or long-term monitoring of patient outcomes. [102] As of 2017, rituximab was widely used off-label to treat RRMS. [103] There is a lack of high quality randomised control trials examining rituximab versus placebo or other disease-modifying therapies, and as such the benefits of rituximab for relapsing remitting multiple sclerosis remain inconclusive. [104] The relative effectiveness of different treatments is unclear, as most have only been compared to placebo or a small number of other therapies. [105] Direct comparisons of interferons and glatiramer acetate indicate similar effects or only small differences in effects on relapse rate, disease progression and magnetic resonance imaging measures. [106] Alemtuzumab, natalizumab, and fingolimod may be more effective than other drugs in reducing relapses over the short term in people with RRMS. [107] Natalizumab and interferon beta-1a ( Rebif ) may reduce relapses compared to both placebo and interferon beta-1a ( Avonex ) while Interferon beta-1b ( Betaseron ), glatiramer acetate , and mitoxantrone may also prevent relapses. [105] Evidence on relative effectiveness in reducing disability progression is unclear. [105] [107] All medications are associated with adverse effects that may influence their risk to benefit profiles. [105] [107] Progressive multiple sclerosis As of 2013, review of 9 immunomodulators and immunosuppressants found no evidence of any being effective in preventing disability progression in people with progressive MS. [105] As of 2017, rituximab has been widely used off-label to treat progressive primary MS. [103] In March 2017 the FDA approved ocrelizumab as a treatment for primary progressive MS, the first drug to gain that approval, [92] [93] with requirements for several Phase IV clinical trials. [94] As of 2011 [update] , only one medication, mitoxantrone, had been approved for secondary progressive MS. [108] In this population tentative evidence supports mitoxantrone moderately slowing the progression of the disease and decreasing rates of relapses over two years. [109] [110] In 2017, ocrelizumab was approved in the United States for the treatment of primary progressive multiple sclerosis in adults. [84] [93] It is also used for the treatment of relapsing forms of multiple sclerosis, to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease in adults. [93] In 2019, siponimod and cladribine were approved in the United States for the treatment of secondary progressive multiple sclerosis. [84] Adverse effects Irritation zone after injection of glatiramer acetate.CD58, HLA-DRB1, IL2RA, CLEC16A, TNFRSF1A, CD40, IL7R, TYK2, KIF1B, HLA-DRA, CBLB, STAT4, TNFAIP3, CD6, TNFSF14, IL10, HLA-DPB1, IL7, APOE, ICAM1, IRF8, IL1RN, IL1B, IFNB1, HLA-DQB1, IFNG, IL17A, VDR, P2RX7, NLRP3, GC, CNR1, CASP1, SLC11A1, POMC, CLDN11, VCAM1, SELE, PDCD1, NECTIN2, IL12A, RBPJ, MCAM, BCHE, KCNJ10, TNF, PRF1, HLA-DQA1, STAT3, LRCH1, HLA-A, HLA-B, CYP27B1, IL23R, CD226, GPC5, NR1H3, MAPK1, IFIH1, ATG5, EVI5, ERG, TAP2, KIF21B, PTPN22, CCR6, MGAT5, CXCR5, ITGAM, RGS1, NOTCH4, FCRL3, CD86, TAGAP, CCR3, GFI1, PTPN2, HSPA1L, RPS6KB1, MERTK, TMEM39A, MMEL1, SP140, GALC, ANKRD55, ATXN2, GSDMB, ERBB3, PVT1, TSFM, TET2, IQGAP1, ZNF433, CTSH, AHI1, HLA-DMB, IFNGR2, BTNL2, VMP1, SLC2A4RG, ZMIZ1, ADAD1, METTL1, ZBTB46, IRGM, IGHA1, MPHOSPH9, TRAF3, VAV2, LRP2, IL2RB, CFB, ICOS, INS-IGF2, TNFSF15, ICOSLG, HLA-DRB4, BACH2, MALT1, MST1, IL13, HLA-DQA2, NCOA2, BATF, PRKRA, MLANA, SIRPG, MBTPS1, ITPR3, CSGALNACT2, ITLN1, INAVA, MYNN, ATG16L1, SLAMF7, DHX16, NEFL, ACE, NAA25, ZNF767P, TNIP1, SPEF2, RPAP2, AGBL2, DLEU1, CENPO, PRRC2A, IFI30, S1PR1, NELFE, CLSTN2, KCNMA1, IL21, EPS15L1, CDR3, MTHFR, NCOA5, PHRF1, ETS1, PITPNM2, GATD3A, HACE1, ARHGAP31, PLEKHG5, NFE2L2, SLC44A2, BANK1, ISG20, CDKAL1, LPP, SLC9A8, HLA-G, HLA-F, MANBA, HLA-DRB9, HLA-DRB6, SAE1, EHMT2, HLA-DRB5, LAMC2, HLA-DQB2, HCP5, HLA-DMA, HLA-C, IL18, PPT2, OTUD3, MAZ, IL6, SPATA2, ATXN2L, LEP, CDC37, IL1A, IQCB1, IFNA13, SBNO2, IFNA1, ARHGEF10, IL2, FGFR1OP, IL4, ELMO1, NPEPPS, DDAH1, PRKD2, PXK, MMP9, FOXP3, MOG, MPO, MS, FAM107A, TIMMDC1, IL23A, WWOX, TSBP1, GFAP, GEM, UBASH3A, KRT20, TNFSF10, RGS14, IL22, ERVW-1, PHGDH, STK19, AK5, MBP, SLC44A4, CXCL10, AFF3, SKAP2, FOXP1, MEFV, DKKL1, RASGRP1, CIITA, MMP2, CTNNA3, TNPO2, TNFSF13B, TSPAN31, BAG6, KIR3DL1, SLC15A2, CDH3, TH2LCRR, PXT1, CD69, PTPRC, GGNBP1, TLR4, CD40LG, HNRNPA1P68, HCG27, TLR2, CD28, PPT2-EGFL8, MS4A1, MIR326, JAZF1, IL12A-AS1, SPRED2, KIAA2026, SLC30A7, CISH, HORMAD2, CHI3L1, PUS10, LRRC34, CLECL1, PLP1, ZNF433-AS1, GLIS3, PSORS1C1, CD52, RNASEL, PLEK, BDNF, ZBTB38, SYT14, MCCD1, C1orf141, IL17REL, LINC01185, C2, LINC00243, TSPO, PCAT1, LINC02656, MIR146A, MIR155, SPP1, BRD2, ZFP36L1, STAT2, RNF5, LINC02649, IRF1-AS1, SUMF1, TIMP1, LINC01934, CHROMR, SNHG28, PKIA-AS1, POU5F1, PPARG, TCF19, HLA-F-AS1, IFNG-AS1, HCG22, NDFIP1, TEF, TRBV20OR9-2, ZFP90, CDSN, LRRK2-DT, ERVK-32, AQP4, TNXB, MACIR, FCRL1, MIR181A1HG, CD24, TOP3A, LINC02357, AGAP2, CCL5, RREB1, LRRK2, LINC02580, SKIV2L, NONOP2, CRYAB, USP8P1, RMI2, LINC02571, TRAF1, CCR5, CSF2, C1QTNF6, LINC01100, CTLA4, SNORA38, LINC01147, CCL2, LACC1, MROH3P, FAS, TTC34, LINC01620, WTAPP1, TSBP1-AS1, LINC01967, CYP21A2, KIAA1109, MIR3681HG, CASC19, EHMT2-AS1, SH3BP2, RBM45, ZGPAT, LINC02471, MPV17L2, LINC02605, ERVK-6, LTA, TGFB1, CD46, TGM2, HMGB1, CXCR3, CYP24A1, CXCL8, HAVCR2, ITGA4, IL27, CX3CR1, TNFRSF1B, IL17D, PLXNA2, NR3C1, CCR2, BCL2, IRF5, VEGFA, CD68, DPP4, HSPA4, ADIPOQ, SIRT1, NOS2, LILRA3, PRL, MYDGF, SOD1, SOAT1, CXCL12, NCAM1, CNTF, GABPA, TLR9, IL18R1, CXCL13, CRP, EBI3, IL12B, HNRNPA1, CXCR2, STAT1, MAG, IFNAR1, IGF1, RELA, MIR223, SMPD1, CX3CL1, IL4R, LIF, PPARGC1A, PDLIM7, AGER, SYT1, MX1, CNR2, SERPINA1, CYP2R1, ESR2, ESR1, EPO, ZNF410, TAM, PECAM1, CSF3, NOTCH3, SERPINE1, GORASP1, IL33, WNK1, SOCS1, PLAT, AGT, TIMP2, MAPT, S100B, IL9, THBS1, HPGDS, ALB, CBLIF, AHR, CD14, CD19, PON1, GJA1, LRPPRC, LOC102724971, ALCAM, LOC102723407, OPN1MW3, ERVK-18, IRF1, IL6ST, LINC01672, P2RX4, MOK, PADI4, MTR, CCR7, TNFSF13, C9orf72, OPN1MW, CD47, PADI2, NFKB1, CD274, RGCC, NGF, GSTM1, KIR2DS1, HFE, PIK3CG, NR4A2, HPRT1, MIR145, HLA-DRB3, IFNAR2, LINGO1, OPN1MW2, MIR21, HNRNPA1P10, KL, WAS, UCP2, PIK3CD, PIK3CB, KIR3DL2, TNFRSF11B, PIK3CA, RPL5, EOMES, TP53, NM, OAS1, NOTCH1, KLRC2, NR0B2, ARHGEF5, CCL20, MYD88, PLG, LGALS3, SELPLG, PTPN6, SDC1, PTHLH, KLK6, TAC1, MSC, LBR, ARHGEF2, PRKCA, TIMELESS, MGAT1, MICB, MIF, MMP1, MMP3, TLR3, LAG3, SH2D2A, HLA-DOA, HAVCR1, CP, NR4A1, CASP8, CAT, CFH, PRDX5, FCGRT, CD34, CD44, GSTT1, GSTP1, CCR4, IGHV3OR16-7, HSPA1B, IGHV3-69-1, OLIG1, GRN, CUX1, DBP, NQO1, P2RY12, SIL1, EDN1, FN1, RGMA, HSPA1A, PDXP, KIF5A, IL5, IL11, IL17F, TRIM22, RTN4R, YY1, OMG, LOC105379528, ROS1, AGTR1, CSF1R, CXCR4, ERVK-11, MAPK14, PDE7A, TNFRSF13C, IL22RA2, ERVK-22, CREB1, MTCO2P12, BMP4, ERVK-12, SYN3, FCGR3B, FCGR3A, FCGR1A, GJC2, AICDA, H3P28, F2RL1, AADAC, GPR183, EZH2, NHS, DMTN, NOS1, EIF2B1, SEMA4A, ASIC2, ERVK-20, ERVK-2, PSMD7, PTGS2, PRB1, B2M, TMEM119, MIR27A, ARMH1, GSTK1, MALAT1, SP3, COMT, LOC390714, MAPK8, SERPING1, TAP1, MIR150, MIR20A, PSMB6, CAV1, PPARA, CD1D, SLC1A1, SLCO6A1, CNP, PLA2G4A, APOA1, FBXW4, CDR2, CLDN5, PML, ERVH-3, ENTPD1, AR, RAB4A, CD80, CD27, C20orf181, LANCL1, ADAM17, HSPA2, TBX21, CD200, GAL, IL15, RPSA, MMP12, DNM1L, TNFSF11, GPR17, ALKBH1, EBNA1BP2, LCN2, MC1R, IGFALS, IDO1, DLL1, SPHK1, GZMB, EIF2B4, EIF2B2, GZMA, CXCL1, ACAD8, CXCL2, SART3, EIF2B5, IL37, HLA-E, EIF2S2, HMOX1, HPT, ACKR3, TP63, SEMA3A, RABEPK, AOC3, KLRB1, ANP32B, TNFRSF25, ND1, RIPK1, TOB1, TRPM4, HRES1, COX2, INS, HP, GAPDH, GAS6, LAIR1, MIR196A2, PARK7, PTGES, MIR142, VN1R17P, SSTR4, MIR23B, SOX10, SSRP1, P2RX2, MIR181C, MIR17, NFASC, STK11, STAT6, TPX2, NLRP1, KLRK1, MIR200A, CST7, GPR166P, MICA, CCL1, CCL3, SIRT1-AS, HTATIP2, CCL7, CXCR6, GJB6, CCL27, CCL21, CCL22, MIR548AC, P2RX5-TAX1BP3, KLRC4-KLRK1, OCLN, SNCB, SGK1, ST8SIA1, PMEL, EHD1, IMMT, NCF1, TALDO1, MIR20B, SLC16A1, BDNF-AS, MIR384, SNAP25, MIR328, SLC2A4, SLC9A9, MIR140, TYRO3, TRIM5, ASCC2, QTRT1, CD276, VIP, TRPV1, DHX40, FTO, ANGPTL4, ZIC1, MZB1, INPP4B, TLR7, GALR2, MMP25, TLR8, TNFRSF12A, COP1, GAS5, FGF23, LGR6, CXCL16, TUG1, SUGP1, ATF7IP, KCNK5, FZD4, ANO2, SPARCL1, KCNH7, CARD16, AIM2, TNFRSF4, NCR1, NTN1, LINC01193, STING1, S1PR2, TH, SEC14L2, LPAR3, GCA, IL32, MRGPRX1, LPAR2, P2RX6, CH25H, GPRC6A, RLS1, SND1, IDO2, OXER1, HT, GPR151, CD200R1, SGSM3, MRGPRX4, MRGPRX3, SGPL1, DEXI, TRAF6, HSP90B2P, CDCP1, A2M, GJB1, EDNRA, EGFR, P2RY2, P2RY1, P2RX5, P2RX3, P2RX1, IGH, IGHG3, C3, BRS3, OAS3, CXCR1, ATN1, IL10RA, NFKBIA, NFKB2, DLD, DHCR24, BTF3P11, SERPINB2, H2AX, NRG1, HBB, CCND1, BCL2L1, HCRT, PRKAR1A, BDKRB1, PTPA, FABP7, HIF1A, BRCA2, HLA-DRB2, PHEX, PHB, HSP90AA1, ERV3-1, BMP7, ICA1, EPHA4, CASP3, ITGAX, MYO1C, STMN1, CYP2D6, KLRC1, MC4R, GLA, LAD1, MBL2, MB, CYBB, CCR1, CD1A, SMAD7, ACKR2, CTNNB1, CST3, LEPR, LPA, LMNB1, CR2, MECP2, MAP3K5, CXCL9, MIP, DDT, DDIT3, ITGB2, MTRR, CD1E, CD4, ATP6, KCNA3, CD8A, CD38, CYP27A1, MST1R, CDKN2A, KIR2DL2, MMP7, NR3C2, KMT2A, AXL, IFNA17, FMR1, FASLG, PSEN1, AKT1, AHSG, APOC2, FOS, PSMD4, RORA, JAG1, ADA, ATF4, ADCYAP1, GATA3, ARG1, PARP1, ARG2, ADRB2, ADRA1A, PTH, ACHE, S100A1, MASP1, RELN, SERPINA3, GPR42, GAD1, ABCA1, ADRA2B, GAP43, RARA, RRN3, FAM167A, PGPEP1, GABRA3, DGCR8, DHCR7, FYN, SARS2, CAMKMT, DDIT4, GSDMD, TRAPPC9, DHODH, RIOK1, ITCH, CCDC134, ARHGAP24, PDCD1LG2, CYP17A1, DOCK8, XAF1, ELL3, COLEC12, DECR1, TRPM7, DAXX, DCN, DCTN1, DNAJC5, DLL4, KAT8, GAD2, SPG11, FOXC1, CYP7A1, CSN3, NEURL3, OPN4, GH1, PRRT2, HSD17B7, CSTF2, ISYNA1, C1QTNF3, NCAN, CSN2, HELB, CRYZ, GHSR, CRYGD, MOGAT1, SLC25A37, CRYGC, CRK, CRHR1, CPT1A, RASD1, INTS4, CYP3A4, CYP2C19, GAS8, GNG2, TREM2, ACKR1, CARD11, SYVN1, L3MBTL3, CYP2C9, IL17RC, CYP2B6, CTSE, CYP1B1, GBE1, GCG, TSLP, ERAP1, ATG16L2, GGTA1P, HSPB11, CTSZ, NLRX1, MTOR, RIC3, FLNA, FLNB, KIR2DL5A, FABP4, ABHD6, NDRG2, F10, ERMN, AHRR, MAVS, ASF1B, F9, F2R, EVI2A, ZFAT, EP400, ETFA, WDR11, SYBU, ERN1, HAMP, ERCC5, CEMIP, ADGRG6, OTUB1, CSGALNACT1, FH, DEFB103B, TWNK, RETN, FGFR1, ZC3HAV1, FOXC2, SPHK2, HMCES, FOXO3, FGF1, FAM20C, FES, RLFP1, FDXR, FANCG, CD177, RTN4, ACOT13, FANCD2, FANCC, AMBRA1, EPHB2, NOX5, EBF1, TOR1A, CSMD1, DSPP, DSG2, IL25, DARS2, SLC52A1, FXN, PINK1, DRD2, DPYSL2, GGCT, TRPM8, DPP6, DHX58, MMP28, DHRS11, KLHL7, DNTT, MARCHF1, DNASE1, RMDN3, SLC25A36, NLRC4, S1PR3, EPAS1, ENO1, PLXNA3, ACE2, OLFM3, TNFRSF19, FNTB, HRH4, ELAVL2, EIF4EBP2, EGR1, FOLR2, EGF, TBC1D2, TMEM74B, CRLF2, NOD2, EDNRB, ABCG4, OGFOD1, ROBO3, CPOX, S100A12, ANTXR2, CLDN3, POTEKP, CEACAM1, BGLAP, MIR148B, BCR, OPN1SW, MIR340, MIR342, MIR376C, TNFRSF17, BCL3, MIR422A, KIR2DL5B, MIR448, MIR409, MIR524, MIR499A, MIR455, POTEM, BAX, ATP2B2, ATM, MIR572, MIR590, MIR633, DEFB103A, TNFSF12-TNFSF13, MIR99B, BMP1, MIR191, DST, MIR19B1, BMPR2, BMP5, MIR210, MIR214, MIR219A1, MIR22, BMP2, MIR23A, MIR25, MIR96, MIR26A1, BLK, MIR27B, MIR29B1, MIR29B2, MIR301A, MIR30A, MIR30D, MIR31, MIR320A, MIR34A, MIR645, MIR648, ATF3, LOC102723971, AMT, AMH, ALOX15, LINC-ROR, ALOX5, AKR1B1, AIF1, AGA, AFP, MAFTRR, THRIL, ADM, ANPEP, ACTG2, ACTG1, GSTT1-AS1, ACTB, RN7SL263P, ACO2, ASIC1, ABO, ABL1, H3P13, H3P24, ANGPT2, SLC25A4, ASMT, APRT, ASCL2, CDKN2B-AS1, HOTAIR, MIR665, MIR922, ARSF, ARSA, ARNTL, HBD, AFA1, MEF2B, APP, ANXA1, ERVW-2, APOD, APOC1, HOTAIRM1, XIAP, BIRC3, BIRC2, AIRE, APC, ANXA5, ANXA2, BRCA1, MIR18A, MIR15B, CECR, BTLA, CHAT, CLEC12A, CEACAM7, FSIP1, ANKFN1, CEACAM3, IFNLR1, TMPRSS6, CETN1, ZNF596, CEACAM5, GPBAR1, CDX2, CDKN2D, CRTC2, CRYGEP, UNC13D, TIGIT, CDKN1C, TBATA, CDH17, CDH1, CD74, CHGA, PLB1, CERS6, NCOA7, CPB1, TPH2, NLRP5, HSPB6, TPRG1L, DUSP15, COX8A, COL17A1, COL11A2, COL2A1, CNTN1, DOCK11, CHGB, CNN3, ADAMTS14, CMKLR1, CCR8, PTGR2, CD300LF, APCDD1, CLIC1, CLU, PDIK1L, CHIT1, CD48, YTHDF3, MIR15A, LINC01194, DDR1, THEMIS, PSMG4, CA12, CA2, MYRF, TOB1-AS1, VPS51, C3AR1, C1QA, BUB1B, ERVFRD-1, SLC25A20, MIRLET7E, MIRLET7I, MIR106A, MIR125A, MIR126, MIR127, MIR132, BTK, BTG1, BST2, BSG, CA13, HCP5B, SFTA3, HCAR2, TAC4, GK5, COPD, SEC14L3, IFNL3, CD1B, KRIT1, RGMB, CASP9, FIRRE, CLEC4D, CAST, CALM1, C1QTNF9, CANX, NAT8L, CALM3, GLDN, TGM6, HSD17B13, CALM2, ACTBL2, H3P44, AMIGO2, RMDN2, GRIA2, RASL12, NTF3, OSM, VRK2, OLR1, WNT3, WT1, XBP1, XRCC1, XRCC5, OGG1, YWHAZ, SLC30A3, DNALI1, NT5E, GLI1, NPHS1, CCN3, DDX39B, NOTCH2, PLA2G7, AIMP2, NPY, NR4A3, NOS3, CDK2AP1, NINJ2, NINJ1, VIPR2, VCL, VAV1, KDM6A, CFP, TP53BP1, TP73, TPI1, TPMT, TPP2, TPSAB1, ENPP2, TRAF2, PDE4B, PCSK1, PCK1, TRPM2, TSTA3, TUBA4A, PCBP1, TXN, TXNRD1, PC, TYR, TYROBP, UBC, UBTF, P4HB, UQCRFS1, NFYA, DYSF, NFATC2, DLK1, TNFRSF10D, TNFRSF10C, TNFRSF10B, TNFRSF10A, MSN, MPZ, MPP1, HDAC3, MMP8, ASAP2, NR1I2, APLN, PER3, MFAP1, CACNA1H, BCL10, BSN, MBD2, MDK, HAP1, SLC25A14, SOCS3, MCC, CLDN12, SLC16A4, TNFRSF11A, TNFRSF6B, PLA2G6, RIPK2, NEFM, NAIP, MYT1, FKBP6, GPR65, SEMA7A, PIK3R3, CNTNAP1, ELP1, MYO9B, MYCN, USO1, MUC1, HSD17B6, OASL, TRNL1, MTNR1B, ND5, ND2, CYTB, ATP8, TNFSF12, MT2A, TNFSF9, TNFRSF14, ABCB1, PLA2G1B, PLA2G2A, REG1A, SELP, PLAAT4, SRSF1, SGCG, RAP1A, SH3GL2, RAF1, SHH, SHMT1, RAC2, RABGGTB, RABGGTA, PVR, SLC1A2, SLC1A3, SLC1A4, PVALB, SLC6A4, PTX3, PTPRN, PTPRM, SLC16A2, PTPRCAP, SIGLEC1, PTPN11, REL, RELB, SNCA, REN, SALL1, SARS1, S100A8, SORT1, ATXN7, ATXN8OS, CLEC11A, SCN8A, SCN10A, RPS6, RPS4X, CCL4, RPA1, CCL8, CCL11, CCL13, CCL15, CCL17, CCL18, CCL19, RNF6, RNASE2, RFX1, CXCL11, CXCL5, PTPN4, FSCN1, PLD1, PKN2, TRB, PRKCE, TDO2, PRDX2, PRKCB, TERC, TFPI, TGFA, TGFB2, TGFB3, TGFBR1, PRCP, PRCC, POU2AF1, PON2, TIMP3, TKT, ICAM5, TLN1, TLR1, POLG, PNMT, PMP22, TSPAN4, PLTP, TRA, ZEB1, PTN, EIF2AK2, SOD2, SORL1, SOX2, PTGER4, SP1, PTAFR, SPAST, PSMD12, PSMD10, PSMB9, PSG2, KLK10, STAT5A, STAT5B, STX1A, ABCC8, VAMP2, SYN1, PRSS3, PROC, TAC3, NAT1, MAP3K7, PRNP, PRLR, SLC16A3, ATG12, MATK, CUX2, ADNP, SIRT3, HMGCR, NNT, HLA-DPA1, DDX58, AMACR, BACE1, SLC7A11, IL17RA, PANX1, PRPF6, RAB3GAP2, HGF, HDAC1, TXN2, PART1, EEF1AKMT3, RNF19A, ADGRA2, CNTNAP2, POLDIP2, HCCS, CLEC4E, SACS, SYNE1, HNMT, OSTF1, HOXB4, IGFBP3, HRH3, IGFBP1, NRM, IGF1R, USP18, IFNGR1, ACOT7, IKZF3, IFNA2, IFN1@, MMRN1, RAB3GAP1, SIRT2, IFI16, SORCS3, IGSF9B, HTC2, HSPD1, HSPB1, CIC, GANAB, SYT11, HSPA5, HRH1, HSPB8, SH3YL1, IL3, PDZRN4, GPX4, SLC40A1, SOX8, GPR37, KCNIP1, PIK3R4, NOX4, IL21R, GPR3, MBL3P, TRAT1, IBD5, GPI, TMED5, DESI2, POLR1D, GNB3, RMDN1, GNA11, SDF4, EGFL7, HSPA14, CKLF, GLO1, TFDP3, CERS2, S100A9, GZMK, UHRF1, GTF2I, GTF2H4, GTF2B, B3GAT1, EIF2AK1, GSR, AGO2, GSN, IL17C, GRM8, GRM7, TOR2A, GRM5, IGHV4-39, GRM4, IGHV3-52, IGHV3-23, GRM3, TRBV20-1, TRBV5-2, TRIB2, GRM1, GRIN2B, GRIA4, GRIA3, POLG2, ADAMTS13, DLG5, GDF15, GOSR1, BAG4, BAG3, LGALS9, H6PD, CLOCK, CYTIP, CARTPT, LGALS8, CTR9, LGALS1, LDLR, LDHA, ARNT2, MFN2, LCN1, SH2B3, CHAF1A, LBP, LAMA4, IL18BP, TSPAN32, EDIL3, LALBA, KLC1, LIG4, ADAMTS1, KNG1, ADAMTS3, MAS1, NOG, MARK3, MAP2, STK17B, ADGRG1, SNORD27, CD83, B4GALT6, CD163, SMAD4, LY6E, LRP1, COX5A, NRXN1, GRAP2, CYP7B1, LPL, QKI, GSTO1, EIF2AK3, FHL5, LMNA, SLC25A27, ADAMTS4, BCAP31, KLRD1, ADRM1, CELF1, ITGA1, IRS1, IRF6, YME1L1, MASP2, CCR9, IRAK1, INSRR, HPSE, CYP46A1, LILRB1, TNFRSF9, IL16, IL12RB2, MMP24, IL10RB, RALBP1, PRDX3, RAB40B, RAB32, METAP2, IL6R, LILRB4, LILRA1, IL5RA, ITGAL, TXNIP, ATP6AP2, USP16, FLOT1, KLKB1, PRSS16, LILRB2, KIR3DS1, TCIRG1, KIR2DL4, KIR2DL3, IKZF1, CCL26, ABCA7, KIR2DL1, WFDC2, KDR, C1D, KCNK3, FST, NXF1, CRTAP, KAT5, JAK3, JAK2, JAK1, TXNRD2, AHSA1, H3P29

-
Transient Epileptic Amnesia
Wikipedia
Transient epileptic amnesia ( TEA ) is a rare but probably underdiagnosed neurological condition which manifests as relatively brief and generally recurring episodes of amnesia caused by underlying temporal lobe epilepsy . [1] Though descriptions of the condition are based on fewer than 100 cases published in the medical literature, [2] and the largest single study to date included 50 people with TEA, [3] [4] TEA offers considerable theoretical significance as competing theories of human memory attempt to reconcile its implications. [5] Contents 1 Symptoms 2 Diagnosis 3 Neuroimaging during events 4 Other transient amnestic syndromes 5 Epidemiology 6 Persistent memory effects 6.1 Accelerated long-term forgetting (ALF) 6.2 Remote memory loss 6.3 Topographical amnesia 7 Treatment 8 Implications for theories of memory 9 References 10 External links Symptoms [ edit ] A person experiencing a TEA episode has very little short-term memory, so that there is profound difficulty remembering events in the past few minutes ( anterograde amnesia ), or of events in the hours prior to the onset of the attack, and even memories of important events in recent years may not be accessible during the amnestic event ( retrograde amnesia ). [6] Some people report short-lived retrograde amnesia so deep that they do not recognize their home or family members, though personal identity is preserved. [7] The amnestic attack has a sudden onset. ... Those focal brain lesions that have been detected have involved the medial temporal lobes. [2] Typically, MRI and CT findings are not remarkable. [6] Other transient amnestic syndromes [ edit ] TEA is, at first, a challenge to distinguish its salient features during the event from transient global amnesia and psychogenic amnesia , though other forms of transient amnesia can include reactions to various medications, closed head injury, and migraine . [6] [13] (Other sources of amnestic symptoms include herpes encephalitis , hypoxia , vascular or basal forebrain lesions, deep midline tumors, early dementia , and Korsakoff syndrome which is secondary to thiamine deficiency , most often the result of alcohol abuse . [1] ) The anatomical and pathophysiological basis of TEA is presumed to be similar to transient global amnesia (TGA), that is, it is likely to be primarily hippocampal in origin, but with more variable involvement of limbic and adjacent temporal lobe neocortical structures. [7] Typical presentation [7] [13] TEA TGA Age at onset early 60s early 60s Gender 67% male 46% male Precipitating factors 70%:sleep/waking 80%: stress, exercise, cold water History epilepsy migraine Procedural memory intact intact Recognizes family, home usually yes Duration 1–60 minutes 2–8 hours EEG during: abnormal after: 40%+abnormal during: normal after: 7% develop epilepsy Other occasional symptoms brief unresponsiveness nausea, headache Autonomic actions Yes (40%) no Degree of amnesia of event 44% have partial recall no recall Personal identity intact intact Persistent memory loss 80%+: ALF autobiographical amnesia topographical amnesia 30%+: ALF autobiographical amnesia . ... CS1 maint: uses authors parameter ( link ) ^ a b c d e f g h Butler, C.R., & Zeman, A. (2006). "Syndromes of Transient Amnesia" (PDF) . ... CS1 maint: uses authors parameter ( link ) ^ a b c d e f g h i j k l m n o p q r Butler, CR., Graham, K.S., Hodges, J.R., Kapur, N., Wardlaw, J.M., and Zeman, A. (2007). "The Syndrome of Transient Epileptic Amnesia" (PDF) .
-
Gout
Wikipedia
When levels are between 415 and 530 μmol/l (7 and 8.9 mg/dl), the risk is 0.5% per year, while in those with a level greater than 535 μmol/l (9 mg/dL), the risk is 4.5% per year. [15] Lifestyle [ edit ] Dietary causes account for about 12% of gout, [19] and include a strong association with the consumption of alcohol, sugar-sweetened beverages, [20] meat, and seafood. [7] Among foods richest in purines yielding high amounts of uric acid are dried anchovies , shrimp, organ meat , dried mushrooms , seaweed , and beer yeast . [21] Chicken and potatoes also appear related. [22] Other triggers include physical trauma and surgery. [8] Studies in the early 2000s found that other dietary factors are not relevant. [23] [24] Specifically, a diet with moderate purine-rich vegetables (e.g., beans , peas , lentils , and spinach ) is not associated with gout. [25] Neither is total dietary protein . [24] [25] Alcohol consumption is strongly associated with increased risk, with wine presenting somewhat less of a risk than beer or spirits . [25] [26] Eating skim milk powder enriched with glycomacropeptide (GMP) and G600 milk fat extract may reduce pain but may result in diarrhea and nausea. [27] Physical fitness, healthy weight, low-fat dairy products, and to a lesser extent, coffee and taking vitamin C, appear to decrease the risk of gout; [28] [29] [30] [31] however, taking vitamin C supplements does not appear to have a significant effect in people who already have established gout. [4] Peanuts, brown bread, and fruit also appear protective. [22] This is believed to be partly due to their effect in reducing insulin resistance . [30] Genetics [ edit ] Gout is partly genetic, contributing to about 60% of variability in uric acid level. [8] The SLC2A9 , SLC22A12 , and ABCG2 genes have been found to be commonly associated with gout and variations in them can approximately double the risk. [32] [33] Loss-of-function mutations in SLC2A9 and SLC22A12 causes low blood uric acid levels by reducing urate absorption and unopposed urate secretion. [33] The rare genetic disorders familial juvenile hyperuricemic nephropathy , medullary cystic kidney disease , phosphoribosylpyrophosphate synthetase superactivity and hypoxanthine-guanine phosphoribosyltransferase deficiency as seen in Lesch–Nyhan syndrome , are complicated by gout. [8] Medical conditions [ edit ] Gout frequently occurs in combination with other medical problems . Metabolic syndrome , a combination of abdominal obesity , hypertension , insulin resistance , and abnormal lipid levels , occurs in nearly 75% of cases. [10] Other conditions commonly complicated by gout include lead poisoning , kidney failure , hemolytic anemia , psoriasis , solid organ transplants , and myeloproliferative disorders such as polycythemia . [8] [34] A body mass index greater than or equal to 35 increases male risk of gout threefold. [23] Chronic lead exposure and lead-contaminated alcohol are risk factors for gout due to the harmful effect of lead on kidney function. [35] Medication [ edit ] Diuretics have been associated with attacks of gout, but a low dose of hydrochlorothiazide does not seem to increase risk. [36] Other medications that increase the risk include niacin , aspirin (acetylsalicylic acid), ACE inhibitors , angiotensin receptor blockers , beta blockers , ritonavir , and pyrazinamide . [4] [16] The immunosuppressive drugs ciclosporin and tacrolimus are also associated with gout, [8] the former more so when used in combination with hydrochlorothiazide. [37] Pathophysiology [ edit ] Chemical structure of uric acid Gout is a disorder of purine metabolism , [8] and occurs when its final metabolite, uric acid , crystallizes in the form of monosodium urate, precipitating and forming deposits (tophi) in joints, on tendons, and in the surrounding tissues. [16] Microscopic tophi may be walled off by a ring of proteins, which blocks interaction of the crystals with cells and therefore avoids inflammation. [38] Naked crystals may break out of walled-off tophi due to minor physical damage to the joint, medical or surgical stress, or rapid changes in uric acid levels. [38] When they break through the tophi, they trigger a local immune -mediated inflammatory reaction in macrophages , which is initiated by the NLRP3 inflammasome protein complex . [4] [16] [38] Activation of the NLRP3 inflammasome recruits the enzyme caspase 1 , which converts pro-interleukin 1β into active interleukin 1β , one of the key proteins in the inflammatory cascade. [4] An evolutionary loss of urate oxidase (uricase), which breaks down uric acid, in humans and higher primates has made this condition common. [8] The triggers for precipitation of uric acid are not well understood. ... No specific agent is significantly more or less effective than any other. [19] Improvement may be seen within four hours and treatment is recommended for one to two weeks. [8] [19] They are not recommended for those with certain other health problems, such as gastrointestinal bleeding , kidney failure , or heart failure . [83] While indometacin has historically been the most commonly used NSAID, an alternative, such as ibuprofen , may be preferred due to its better side effect profile in the absence of superior effectiveness. [36] For those at risk of gastric side effects from NSAIDs, an additional proton pump inhibitor may be given. [84] There is some evidence that COX-2 inhibitors may work as well as nonselective NSAIDs for acute gout attack with fewer side effects. [85] [86] Colchicine [ edit ] Colchicine is an alternative for those unable to tolerate NSAIDs. [19] At high doses, side effects (primarily gastrointestinal upset) limit its usage. [87] At lower doses, which are still effective, it is well tolerated. [36] [88] Colchicine may interact with other commonly prescribed drugs, such as atorvastatin and erythromycin , among others. [87] Glucocorticoids [ edit ] Glucocorticoids have been found to be as effective as NSAIDs [89] [90] and may be used if contraindications exist for NSAIDs. [19] [91] They also lead to improvement when injected into the joint . [19] A joint infection must be excluded, however, as glucocorticoids worsen this condition. [19] There were no short-term adverse effects reported. [92] Others [ edit ] Interleukin-1 inhibitors, such as canakinumab , showed moderate effectiveness for pain relief and reduction of joint swelling, but have increased risk of adverse events , such as back pain, headache, and increased blood pressure. [93] They, however, may work less well than usual doses of NSAIDS. [93] The high cost of this class of drugs may also discourage their use for treating gout. [93] Prognosis [ edit ] Without treatment, an acute attack of gout usually resolves in five to seven days; however, 60% of people have a second attack within one year. [15] Those with gout are at increased risk of hypertension , diabetes mellitus , metabolic syndrome , and kidney and cardiovascular disease and thus are at increased risk of death. [8] [94] It is unclear whether medications that lower urate affect cardiovascular disease risks. [95] This may be partly due to its association with insulin resistance and obesity, but some of the increased risk appears to be independent. [94] Without treatment, episodes of acute gout may develop into chronic gout with destruction of joint surfaces, joint deformity, and painless tophi. [8] These tophi occur in 30% of those who are untreated for five years, often in the helix of the ear, over the olecranon processes, or on the Achilles tendons . [8] With aggressive treatment, they may dissolve. Kidney stones also frequently complicate gout, affecting between 10 and 40% of people and occur due to low urine pH promoting the precipitation of uric acid. [8] Other forms of chronic kidney dysfunction may occur. [8] Gouty tophi presenting as nodules on the finger and helix of the ear Tophus of the knee Tophii on the toe and ankle Gout complicated by ruptured tophi, the exudite of which tested positive for uric acid crystals Gout in the joint of the big toe Gross pathology of a large tophus Epidemiology [ edit ] Gout affects around 1–2% of the Western population at some point in their lifetimes and is becoming more common. [8] [19] Some 5.8 million people were affected in 2013. [96] Rates of gout approximately doubled between 1990 and 2010. [16] This rise is believed to be due to increasing life expectancy, changes in diet and an increase in diseases associated with gout, such as metabolic syndrome and high blood pressure . [23] Factors that influence rates of gout include age, race, and the season of the year. ... "[Levels of uric acid in serum in patients with metabolic syndrome]" [Levels of uric acid in serum in patients with metabolic syndrome].ABCG2, SLC2A9, CD14, IL1B, IL1RN, ALPK1, XDH, CARD8, ALDH16A1, HPRT1, ZNF518B, HNF1B, DARS2, BCAS3, ALX4, RNF115, MACROD1, SEC61A1, NRBP1, A1CF, MLXIPL, TRIM54, MEPE, PRKAG2, SFMBT1, CNTN5, SLC22A11, CARMIL1, RBFOX1, SHLD2, ABCA1, TBL2, FNDC4, SLC17A4, ABCC9, SLC17A2, H2AC5P, BAIAP2, TRIM38, KAT5, SCGN, POLR3C, SLC17A3, SLC22A7, CD160, NXPH4, GPN1, R3HDM2, MLXIP, SLC4A1AP, FSTL4, CUX2, IFT172, FBXO22, ZSCAN31, WNT5B, SLC13A3, TRIM46, LINC02537, RAF1P1, LHFPL3, KRT8P26, OR7E35P, CRIP3, FAM86MP, LINC01460, LINC01405, ALG1L3P, ADPGK-AS1, H2BC2P, MUC22, AADACL2-AS1, CT69, LINC01229, RFX3-AS1, B4GALT1-AS1, PPM1K-DT, RELA-DT, NRXN2-AS1, HNF1A-AS1, NALCN, H2BC1, CLNK, WDR1, INHBE, QRICH2, RNASEH2C, C2orf16, ZNF512, AP5B1, UBE2Q2, SLC22A12, ZNF513, CNIH2, NRG4, NIPAL1, FAM53A, LINC01010, NUDT17, KRTCAP3, SLC16A9, H2AC1, JAZF1, SH2B3, ABCG1, SNX17, ORC4, IGF1R, INHBC, INSR, KCNQ1, LRP6, MAP3K11, MPV17, MUC1, SLC22A18AS, HLF, OVOL1, PDE1C, PDZK1, PFKM, PKD2, ACVR2A, PPM1G, PRKCA, HNF4G, HGF, PRPS1, CYP2E1, ALDH2, ANK1, APOE, ATP1A4, BDKRB2, CFTR, CLCNKB, CYP2C8, EPB42, HFE, FGFR2, FRK, G6PC, SLC37A4, GCKR, GTF3C2, H1-2, H1-6, MAPK6, PPARD, H2BP5, ZMYM6, SPP1, SPTA1, SPTB, ABCC8, SLC5A6, ALDH1A2, PTPRD, HNF1A, TPST1, H4C2, H4C3, H3C2, H2BC4, UMOD, VDR, H2AC4, BAZ1B, BCL7B, NRXN2, PYGM, BABAM2, MAP4K2, RAB27B, RARB, MRPL33, RREB1, ATXN2, SLC22A1, SLC4A1, SLC12A3, SLC17A1, H2AC6, CXCL8, ADIPOQ, CRP, BCL2, CXCL16, NR2C2, MT1B, PRKG2, POMC, S100A9, CCL2, IL33, MTTP, SLC40A1, SIRT1, MAP3K7, IL18, IL6, TGFB1, TNF, HLA-B, IL4

-
Diabetic Neuropathy
Wikipedia
Therefore, diabetic neuropathy has the potential to affect essentially any organ system and can cause a range of symptoms. There are several distinct syndromes based on the organ systems affected. Sensorimotor polyneuropathy [ edit ] Longer nerve fibers are affected to a greater degree than shorter ones because nerve conduction velocity is slowed in proportion to a nerve's length. In this syndrome, decreased sensation and loss of reflexes occurs first in the toes on each foot, then extends upward. ... Damage to a specific nerve of the thoracic or lumbar spinal nerves can occur and may lead to painful syndromes that mimic a heart attack , gallbladder inflammation , or appendicitis . Diabetics have a higher incidence of entrapment neuropathies, such as carpal tunnel syndrome . Pathogenesis [ edit ] The following processes are thought to be involved in the development of diabetic neuropathy: Microvascular disease [ edit ] Main article: Microangiopathy Vascular and neural diseases are closely related. ... Normal results on vibration testing (LR range, 0.33–0.51) or monofilament (LR range, 0.09–0.54) make large fiber peripheral neuropathy from diabetes less likely. [5] Nerve conduction tests may show reduced functioning of the peripheral nerves, but seldom correlate with the severity of diabetic peripheral neuropathy and are not appropriate as routine tests for the condition. [6] Classification [ edit ] Diabetic neuropathy encompasses a series of different neuropathic syndromes which can be categorized as follows: [7] Focal and multifocal neuropathies: Mononeuropathy which affects one nerve Amyotrophy or radiculopathy such as proximal diabetic neuropathy , affecting a specific pattern of nerves Multiple lesions, affecting nerves that don't follow a specific pattern, also called "mononeuritis multiplex" Nerve damage from entrapment (e.g. median, ulnar, peroneal) Symmetrical neuropathies: Sensory Autonomic Distal symmetrical polyneuropathy (DSPN), the diabetic type of which is also known as diabetic peripheral neuropathy (DPN) (most common presentation) Prevention [ edit ] This section needs expansion .INSR, TLR4, CASP3, TGFB1, CAT, NTF3, HGF, GRM5, MME, CHRM2, MMP2, SGK1, AKR1B1, MMP9, LEPR, NGF, BDNF, IL1B, TNF, IGF1, NGFR, MPZ, TRPA1, NTRK1, BECN1, HHIP, PTGS2, MAPK14, SREBF1, BAD, TGFB2, BDKRB1, LRRK2, TGFB3, NRG1, MBP, CNR1, VEGFA, NFE2L2, GABPA, APOE, MTHFR, TNFSF11, PARP1, GSTT1, NPY, GSTM1, SIRT1, EPO, ST3GAL4, TRPV1, VDR, UCP3, TXN, TTR, TLR5, TKT, THBD, UCP2, HSPB3, SCG2, LOH19CR1, MIR25, MIR199A2, MIR199A1, MIR155, COL6A5, RPAIN, TMX1, FTO, SEMA6A, KIDINS220, STAP2, DUOX1, GAL, NOX4, DUOX2, ARIH1, DIANPH, NFASC, PNPLA6, PPARGC1A, TXNIP, DCAF1, SMPD1, NRP1, RIPK1, RNMT, IRS2, SOD2, PDE4A, SLC6A6, HMOX1, GRB2, GPX1, GLO1, GAP43, MTOR, FOXO3, ACSL1, EPOR, ENO2, DPYSL2, DECR1, ACE, CYBB, CSF3, COL11A2, CCR8, CAV1, C3, HCN2, ATP1A1, XIAP, ALOX15, ALB, GSTP1, AGFG1, SHH, HSPB1, CCL1, RPS19, ROS1, RELA, PTPN1, PSMD9, MAPK3, PRKCD, PMM2, PLAT, SERPINE2, PGF, AGER, TNFRSF11B, NOTCH1, MIF, MFAP4, LPO, IL10, IL6, IGFBP5, IGF1R, HSPB2, MIR499A
-
Hemothorax
Wikipedia
Rarely, a rupture of the thoracic aorta can result in a hemothorax, but the bleeding usually occurs in the pericardial space. [13] Spontaneous tearing of blood vessels is more likely to occur in those with disorders that weaken blood vessels such as some forms of Ehlers-Danlos syndrome , disorders that lead to malformed blood vessels as seen in Rendu-Osler-Weber syndrome , or in bleeding disorders such as hemophilia and Glanzmann thromboastenia . ... Catamenial [ edit ] Rarely, hemothoraces can arise due to extrapelvic endometriosis , a condition in which tissue similar to the lining that normally covers the inside of the uterus forms in unusual locations outside the pelvis. [14] Endometriotic tissue that implants on the pleural surface can bleed in response to the hormonal changes of the menstrual cycle, causing what is known as a catamenial hemothorax as part of the thoracic endometriosis syndrome along with catamenial pneumothorax , catamenial hemoptysis , and lung nodules of endometriosis. [15] Catamenial hemothorax represents 14% of cases of thoracic endometriosis syndrome [16] while catamenial pneumothorax is seen in 73%, catamenial hemoptysis in 7%, and pulmonary nodules in 6%. [14] Mechanism [ edit ] Autopsy specimen showing a large clotted hemothorax filling the entire pleural cavity When a hemothorax occurs, blood enters the pleural cavity. ... PMID 32642009 . ^ Rousset P, Rousset-Jablonski C, Alifano M, Mansuet-Lupo A, Buy JN, Revel MP (March 2014). "Thoracic endometriosis syndrome: CT and MRI features". Clin Radiol . 69 (3): 323–30. doi : 10.1016/j.crad.2013.10.014 . ... Classification D ICD - 10 : J94.2 , S27.1 ICD - 9-CM : 511.8 , 860 MeSH : D006491 DiseasesDB : 19762 External resources MedlinePlus : 000126 eMedicine : med/2915 ped/971 v t e Diseases of the respiratory system Upper RT (including URTIs , common cold ) Head sinuses Sinusitis nose Rhinitis Vasomotor rhinitis Atrophic rhinitis Hay fever Nasal polyp Rhinorrhea nasal septum Nasal septum deviation Nasal septum perforation Nasal septal hematoma tonsil Tonsillitis Adenoid hypertrophy Peritonsillar abscess Neck pharynx Pharyngitis Strep throat Laryngopharyngeal reflux (LPR) Retropharyngeal abscess larynx Croup Laryngomalacia Laryngeal cyst Laryngitis Laryngopharyngeal reflux (LPR) Laryngospasm vocal cords Laryngopharyngeal reflux (LPR) Vocal fold nodule Vocal fold paresis Vocal cord dysfunction epiglottis Epiglottitis trachea Tracheitis Laryngotracheal stenosis Lower RT / lung disease (including LRTIs ) Bronchial / obstructive acute Acute bronchitis chronic COPD Chronic bronchitis Acute exacerbation of COPD ) Asthma ( Status asthmaticus Aspirin-induced Exercise-induced Bronchiectasis Cystic fibrosis unspecified Bronchitis Bronchiolitis Bronchiolitis obliterans Diffuse panbronchiolitis Interstitial / restrictive ( fibrosis ) External agents/ occupational lung disease Pneumoconiosis Aluminosis Asbestosis Baritosis Bauxite fibrosis Berylliosis Caplan's syndrome Chalicosis Coalworker's pneumoconiosis Siderosis Silicosis Talcosis Byssinosis Hypersensitivity pneumonitis Bagassosis Bird fancier's lung Farmer's lung Lycoperdonosis Other ARDS Combined pulmonary fibrosis and emphysema Pulmonary edema Löffler's syndrome / Eosinophilic pneumonia Respiratory hypersensitivity Allergic bronchopulmonary aspergillosis Hamman-Rich syndrome Idiopathic pulmonary fibrosis Sarcoidosis Vaping-associated pulmonary injury Obstructive / Restrictive Pneumonia / pneumonitis By pathogen Viral Bacterial Pneumococcal Klebsiella Atypical bacterial Mycoplasma Legionnaires' disease Chlamydiae Fungal Pneumocystis Parasitic noninfectious Chemical / Mendelson's syndrome Aspiration / Lipid By vector/route Community-acquired Healthcare-associated Hospital-acquired By distribution Broncho- Lobar IIP UIP DIP BOOP-COP NSIP RB Other Atelectasis circulatory Pulmonary hypertension Pulmonary embolism Lung abscess Pleural cavity / mediastinum Pleural disease Pleuritis/pleurisy Pneumothorax / Hemopneumothorax Pleural effusion Hemothorax Hydrothorax Chylothorax Empyema/pyothorax Malignant Fibrothorax Mediastinal disease Mediastinitis Mediastinal emphysema Other/general Respiratory failure Influenza Common cold SARS Coronavirus disease 2019 Idiopathic pulmonary haemosiderosis Pulmonary alveolar proteinosis v t e Chest injury , excluding fractures Cardiac and circulatory system injuries vascular : Traumatic aortic rupture Thoracic aorta injury heart : Myocardial contusion / Commotio cordis Cardiac tamponade Hemopericardium Myocardial rupture Lung and lower respiratory tract injuries Pneumothorax Hemothorax Hemopneumothorax Pulmonary contusion Pulmonary laceration Tracheobronchial injury Diaphragmatic rupture v t e Disorders of bleeding and clotting Coagulation · coagulopathy · Bleeding diathesis Clotting By cause Clotting factors Antithrombin III deficiency Protein C deficiency Activated protein C resistance Protein S deficiency Factor V Leiden Prothrombin G20210A Platelets Sticky platelet syndrome Thrombocytosis Essential thrombocythemia DIC Purpura fulminans Antiphospholipid syndrome Clots Thrombophilia Thrombus Thrombosis Virchow's triad Trousseau sign of malignancy By site Deep vein thrombosis Bancroft's sign Homans sign Lisker's sign Louvel's sign Lowenberg's sign Peabody's sign Pratt's sign Rose's sign Pulmonary embolism Renal vein thrombosis Bleeding By cause Thrombocytopenia Thrombocytopenic purpura : ITP Evans syndrome TM TTP Upshaw–Schulman syndrome Heparin-induced thrombocytopenia May–Hegglin anomaly Platelet function adhesion Bernard–Soulier syndrome aggregation Glanzmann's thrombasthenia platelet storage pool deficiency Hermansky–Pudlak syndrome Gray platelet syndrome Clotting factor Hemophilia A/VIII B/IX C/XI von Willebrand disease Hypoprothrombinemia/II Factor VII deficiency Factor X deficiency Factor XII deficiency Factor XIII deficiency Dysfibrinogenemia Congenital afibrinogenemia Signs and symptoms Bleeding Bruise Hematoma Petechia Purpura Nonthrombocytopenic purpura By site head Epistaxis Hemoptysis Intracranial hemorrhage Hyphema Subconjunctival hemorrhage torso Hemothorax Hemopericardium Pulmonary hematoma abdomen Gastrointestinal bleeding Hemobilia Hemoperitoneum Hematocele Hematosalpinx joint Hemarthrosis v t e Trauma Principles Polytrauma Major trauma Traumatology Triage Resuscitation Trauma triad of death Assessment Clinical prediction rules Revised Trauma Score Injury Severity Score Abbreviated Injury Scale NACA score Investigations Diagnostic peritoneal lavage Focused assessment with sonography for trauma Management Principles Advanced trauma life support Trauma surgery Trauma center Trauma team Damage control surgery Early appropriate care Procedures Resuscitative thoracotomy Pathophysiology Injury MSK Bone fracture Joint dislocation Degloving Soft tissue injury Resp Flail chest Pneumothorax Hemothorax Diaphragmatic rupture Pulmonary contusion Cardio Internal bleeding Thoracic aorta injury Cardiac tamponade GI Blunt kidney trauma Ruptured spleen Neuro Penetrating head injury Traumatic brain injury Intracranial hemorrhage Mechanism Blast injury Blunt trauma Burn Penetrating trauma Crush injury Stab wound Ballistic trauma Electrocution Region Abdominal trauma Chest trauma Facial trauma Head injury Spinal cord injury Demographic Geriatric trauma Pediatric trauma Complications Posttraumatic stress disorder Wound healing Acute lung injury Crush syndrome Rhabdomyolysis Compartment syndrome Contracture Volkmann's contracture Embolism air fat Chronic traumatic encephalopathy Subcutaneous emphysema
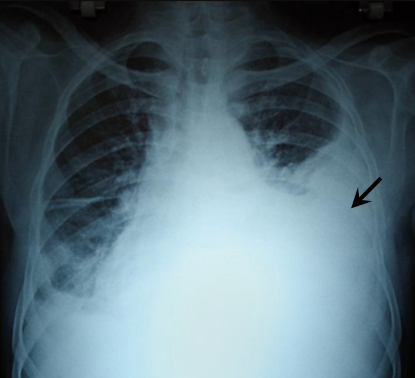
-
Tularemia
Wikipedia
Army Biological Warfare Labs Building 101 Building 257 Building 470 Deseret Test Center Dugway Proving Ground Fort Detrick Fort Douglas Fort Terry Granite Peak Installation Horn Island Testing Station One-Million-Liter Test Sphere Pine Bluff Arsenal Plum Island Animal Disease Center Vigo Ordnance Plant Related topics Biological agent Biological warfare Entomological warfare Soviet biological weapons program Korean War bio-warfare allegations List of topics U.S. biological weapons program U.S. biological defense program U.S. bio-weapons ban War Bureau of Consultants War Research Service v t e Proteobacteria -associated Gram-negative bacterial infections α Rickettsiales Rickettsiaceae / ( Rickettsioses ) Typhus Rickettsia typhi Murine typhus Rickettsia prowazekii Epidemic typhus , Brill–Zinsser disease , Flying squirrel typhus Spotted fever Tick-borne Rickettsia rickettsii Rocky Mountain spotted fever Rickettsia conorii Boutonneuse fever Rickettsia japonica Japanese spotted fever Rickettsia sibirica North Asian tick typhus Rickettsia australis Queensland tick typhus Rickettsia honei Flinders Island spotted fever Rickettsia africae African tick bite fever Rickettsia parkeri American tick bite fever Rickettsia aeschlimannii Rickettsia aeschlimannii infection Mite-borne Rickettsia akari Rickettsialpox Orientia tsutsugamushi Scrub typhus Flea-borne Rickettsia felis Flea-borne spotted fever Anaplasmataceae Ehrlichiosis : Anaplasma phagocytophilum Human granulocytic anaplasmosis , Anaplasmosis Ehrlichia chaffeensis Human monocytotropic ehrlichiosis Ehrlichia ewingii Ehrlichiosis ewingii infection Rhizobiales Brucellaceae Brucella abortus Brucellosis Bartonellaceae Bartonellosis : Bartonella henselae Cat-scratch disease Bartonella quintana Trench fever Either B. henselae or B. quintana Bacillary angiomatosis Bartonella bacilliformis Carrion's disease , Verruga peruana β Neisseriales M+ Neisseria meningitidis/meningococcus Meningococcal disease , Waterhouse–Friderichsen syndrome , Meningococcal septicaemia M− Neisseria gonorrhoeae/gonococcus Gonorrhea ungrouped: Eikenella corrodens / Kingella kingae HACEK Chromobacterium violaceum Chromobacteriosis infection Burkholderiales Burkholderia pseudomallei Melioidosis Burkholderia mallei Glanders Burkholderia cepacia complex Bordetella pertussis / Bordetella parapertussis Pertussis γ Enterobacteriales ( OX− ) Lac+ Klebsiella pneumoniae Rhinoscleroma , Pneumonia Klebsiella granulomatis Granuloma inguinale Klebsiella oxytoca Escherichia coli : Enterotoxigenic Enteroinvasive Enterohemorrhagic O157:H7 O104:H4 Hemolytic-uremic syndrome Enterobacter aerogenes / Enterobacter cloacae Slow/weak Serratia marcescens Serratia infection Citrobacter koseri / Citrobacter freundii Lac− H2S+ Salmonella enterica Typhoid fever , Paratyphoid fever , Salmonellosis H2S− Shigella dysenteriae / sonnei / flexneri / boydii Shigellosis , Bacillary dysentery Proteus mirabilis / Proteus vulgaris Yersinia pestis Plague / Bubonic plague Yersinia enterocolitica Yersiniosis Yersinia pseudotuberculosis Far East scarlet-like fever Pasteurellales Haemophilus : H. influenzae Haemophilus meningitis Brazilian purpuric fever H. ducreyi Chancroid H. parainfluenzae HACEK Pasteurella multocida Pasteurellosis Actinobacillus Actinobacillosis Aggregatibacter actinomycetemcomitans HACEK Legionellales Legionella pneumophila / Legionella longbeachae Legionnaires' disease Coxiella burnetii Q fever Thiotrichales Francisella tularensis Tularemia Vibrionaceae Vibrio cholerae Cholera Vibrio vulnificus Vibrio parahaemolyticus Vibrio alginolyticus Plesiomonas shigelloides Pseudomonadales Pseudomonas aeruginosa Pseudomonas infection Moraxella catarrhalis Acinetobacter baumannii Xanthomonadaceae Stenotrophomonas maltophilia Cardiobacteriaceae Cardiobacterium hominis HACEK Aeromonadales Aeromonas hydrophila / Aeromonas veronii Aeromonas infection ε Campylobacterales Campylobacter jejuni Campylobacteriosis , Guillain–Barré syndrome Helicobacter pylori Peptic ulcer , MALT lymphoma , Gastric cancer Helicobacter cinaedi Helicobacter cellulitis v t e Tick-borne diseases and infestations Diseases Bacterial infections Rickettsiales Anaplasmosis Boutonneuse fever Ehrlichiosis ( Human granulocytic , Human monocytotropic , Human E. ewingii infection ) Scrub typhus Spotted fever rickettsiosis Pacific Coast tick fever American tick bite fever rickettsialpox Rocky Mountain spotted fever ) Spirochaete Baggio–Yoshinari syndrome Lyme disease Relapsing fever borreliosis Thiotrichales Tularemia Viral infections Bhanja virus Bourbon virus Colorado tick fever Crimean–Congo hemorrhagic fever Heartland bandavirus Kemerovo tickborne viral fever Kyasanur Forest disease Omsk hemorrhagic fever Powassan encephalitis Severe fever with thrombocytopenia syndrome Tete orthobunyavirus Tick-borne encephalitis Protozoan infections Babesiosis Other diseases Tick paralysis Alpha-gal allergy Southern tick-associated rash illness Infestations Tick infestation Species and bites Amblyomma Amblyomma americanum Amblyomma cajennense Amblyomma triguttatum Dermacentor Dermacentor andersoni Dermacentor variabilis Ixodes Ixodes cornuatus Ixodes holocyclus Ixodes pacificus Ixodes ricinus Ixodes scapularis Ornithodoros Ornithodoros gurneyi Ornithodoros hermsi Ornithodoros moubata Other Rhipicephalus sanguineus Authority control GND : 4186421-9 NDL : 00576246

-
Listeriosis
Wikipedia
In the EU , it has stabilized at around 5 cases per annum per million population, although the rate in each country contributing data to EFSA / ECDC varies greatly. [11] There are four distinct clinical syndromes: [ citation needed ] Infection in pregnancy: Listeria can proliferate asymptomatically in the vagina and uterus . ... External links [ edit ] Media related to Listeriosis at Wikimedia Commons CDC Listeriosis site Classification D ICD - 10 : A32 ICD - 9-CM : 027.0 MeSH : D008088 DiseasesDB : 7503 External resources MedlinePlus : 001380 eMedicine : med/1312 ped/1319 Patient UK : Listeriosis Orphanet : 533 v t e Firmicutes (low- G+C ) Infectious diseases Bacterial diseases : G+ Bacilli Lactobacillales ( Cat- ) Streptococcus α optochin susceptible S. pneumoniae Pneumococcal infection optochin resistant Viridans streptococci : S. mitis S. mutans S. oralis S. sanguinis S. sobrinus S. anginosus group β A bacitracin susceptible: S. pyogenes Group A streptococcal infection Streptococcal pharyngitis Scarlet fever Erysipelas Rheumatic fever B bacitracin resistant, CAMP test +: S. agalactiae Group B streptococcal infection ungrouped Streptococcus iniae Cutaneous Streptococcus iniae infection γ D BEA +: Streptococcus bovis Enterococcus BEA +: Enterococcus faecalis Urinary tract infection Enterococcus faecium Bacillales ( Cat+ ) Staphylococcus Cg+ S. aureus Staphylococcal scalded skin syndrome Toxic shock syndrome MRSA Cg- novobiocin susceptible S. epidermidis novobiocin resistant S. saprophyticus Bacillus Bacillus anthracis Anthrax Bacillus cereus Food poisoning Listeria Listeria monocytogenes Listeriosis Clostridia Clostridium ( spore -forming) motile: Clostridium difficile Pseudomembranous colitis Clostridium botulinum Botulism Clostridium tetani Tetanus nonmotile: Clostridium perfringens Gas gangrene Clostridial necrotizing enteritis Finegoldia (non-spore forming) Finegoldia magna Mollicutes Mycoplasmataceae Ureaplasma urealyticum Ureaplasma infection Mycoplasma genitalium Mycoplasma pneumoniae Mycoplasma pneumonia Anaeroplasmatales Erysipelothrix rhusiopathiae Erysipeloid v t e Vertically transmitted infections Gestational Viruses Congenital rubella syndrome Congenital cytomegalovirus infection Neonatal herpes simplex Hepatitis B Congenital varicella syndrome HIV Fifth disease Bacteria Congenital syphilis Other Toxoplasmosis transplacental TORCH complex During birth transcervical Candidiasis Gonorrhea Listeriosis Late pregnancy Listeriosis Congenital cytomegalovirus infection By breastfeeding Breastfeeding Tuberculosis HIVTNF, CYLD, IL15, IFNG, HSP90B1, NOD2, SUMF2, DECR1, IL10, IL37, ISG15, STIP1, BAHD1, FAF1, ABCG2, CPQ, SIRT2, LGI1, SQSTM1, SOCS2, BECN1, PTP4A2, ARHGEF5, CARD8, ACTA1, NT5C2, CLEC5A, TP53, SENP1, NOP53, DUOX2, HSPA14, LGI2, LXN, BCL11B, CASD1, TNIP3, HAVCR2, ZNRF4, MIR146A, EIF2AK1, ADAM17, TNFRSF1A, GRIN1, IL6, IL4, IFNB1, IFIT3, HSPG2, HSPD1, GRN, ACTB, XCR1, GFAP, CCR5, CD44, CAT, CASP1, IL12A, ISG20, ITGAM, ITGB2, LIPE, MET, MYH9, NEDD4, NFATC1, OCRL, PML, PPIA, S100A1, S100B, SELE, SLC5A1, SPP1, H3P7

-
Air Embolism
Wikipedia
External links [ edit ] Arterial Gas Embolism Classification D ICD - 10 : O88.0 , T79.0 ICD - 9-CM : 673.0 , 999.1 MeSH : D004618 DiseasesDB : 313 SNOMED CT : 271376002 External resources eMedicine : emerg/787 v t e Pathology of pregnancy , childbirth and the puerperium Pregnancy Pregnancy with abortive outcome Abortion Ectopic pregnancy Abdominal Cervical Interstitial Ovarian Heterotopic Embryo loss Fetal resorption Molar pregnancy Miscarriage Stillbirth Oedema , proteinuria and hypertensive disorders Gestational hypertension Pre-eclampsia HELLP syndrome Eclampsia Other, predominantly related to pregnancy Digestive system Acute fatty liver of pregnancy Gestational diabetes Hepatitis E Hyperemesis gravidarum Intrahepatic cholestasis of pregnancy Integumentary system / dermatoses of pregnancy Gestational pemphigoid Impetigo herpetiformis Intrahepatic cholestasis of pregnancy Linea nigra Prurigo gestationis Pruritic folliculitis of pregnancy Pruritic urticarial papules and plaques of pregnancy (PUPPP) Striae gravidarum Nervous system Chorea gravidarum Blood Gestational thrombocytopenia Pregnancy-induced hypercoagulability Maternal care related to the fetus and amniotic cavity amniotic fluid Oligohydramnios Polyhydramnios Braxton Hicks contractions chorion / amnion Amniotic band syndrome Chorioamnionitis Chorionic hematoma Monoamniotic twins Premature rupture of membranes Obstetrical bleeding Antepartum placenta Circumvallate placenta Monochorionic twins Placenta accreta Placenta praevia Placental abruption Twin-to-twin transfusion syndrome Labor Amniotic fluid embolism Cephalopelvic disproportion Dystocia Shoulder dystocia Fetal distress Locked twins Nuchal cord Obstetrical bleeding Postpartum Pain management during childbirth placenta Placenta accreta Preterm birth Postmature birth Umbilical cord prolapse Uterine inversion Uterine rupture Vasa praevia Puerperal Breastfeeding difficulties Low milk supply Cracked nipples Breast engorgement Childbirth-related posttraumatic stress disorder Diastasis symphysis pubis Postpartum bleeding Peripartum cardiomyopathy Postpartum depression Postpartum psychosis Postpartum thyroiditis Puerperal fever Puerperal mastitis Other Concomitant conditions Diabetes mellitus Systemic lupus erythematosus Thyroid disorders Maternal death Sexual activity during pregnancy Category v t e Trauma Principles Polytrauma Major trauma Traumatology Triage Resuscitation Trauma triad of death Assessment Clinical prediction rules Revised Trauma Score Injury Severity Score Abbreviated Injury Scale NACA score Investigations Diagnostic peritoneal lavage Focused assessment with sonography for trauma Management Principles Advanced trauma life support Trauma surgery Trauma center Trauma team Damage control surgery Early appropriate care Procedures Resuscitative thoracotomy Pathophysiology Injury MSK Bone fracture Joint dislocation Degloving Soft tissue injury Resp Flail chest Pneumothorax Hemothorax Diaphragmatic rupture Pulmonary contusion Cardio Internal bleeding Thoracic aorta injury Cardiac tamponade GI Blunt kidney trauma Ruptured spleen Neuro Penetrating head injury Traumatic brain injury Intracranial hemorrhage Mechanism Blast injury Blunt trauma Burn Penetrating trauma Crush injury Stab wound Ballistic trauma Electrocution Region Abdominal trauma Chest trauma Facial trauma Head injury Spinal cord injury Demographic Geriatric trauma Pediatric trauma Complications Posttraumatic stress disorder Wound healing Acute lung injury Crush syndrome Rhabdomyolysis Compartment syndrome Contracture Volkmann's contracture Embolism air fat Chronic traumatic encephalopathy Subcutaneous emphysema v t e Underwater diving Diving modes Atmospheric pressure diving Freediving Saturation diving Scuba diving Snorkeling Surface oriented diving Surface-supplied diving Unmanned diving Diving equipment Cleaning and disinfection of personal diving equipment Human factors in diving equipment design Basic equipment Diving mask Snorkel Swimfin Breathing gas Bailout gas Bottom gas Breathing air Decompression gas Emergency gas supply Heliox Nitrox Oxygen Travel gas Trimix Buoyancy and trim equipment Buoyancy compensator Power inflator Dump valve Diving weighting system Ankle weights Integrated weights Trim weights Weight belt Decompression equipment Decompression buoy Decompression cylinder Decompression trapeze Dive computer Diving shot Jersey upline Jonline Diving suit Atmospheric diving suit Dry suit Sladen suit Standard diving suit Rash vest Wetsuit Dive skins Hot-water suit Helmets and masks Anti-fog Diving helmet Free-flow helmet Lightweight demand helmet Orinasal mask Reclaim helmet Shallow water helmet Standard diving helmet Diving mask Band mask Full-face mask Half mask Instrumentation Bottom timer Depth gauge Dive computer Dive timer Diving watch Helium release valve Pneumofathometer Submersible pressure gauge Mobility equipment Diving bell Closed bell Wet bell Diving stage Swimfin Monofin PowerSwim Towboard Diver propulsion vehicle Advanced SEAL Delivery System Cosmos CE2F series Dry Combat Submersible Human torpedo Motorised Submersible Canoe Necker Nymph R-2 Mala-class swimmer delivery vehicle SEAL Delivery Vehicle Shallow Water Combat Submersible Siluro San Bartolomeo Wet Nellie Wet sub Safety equipment Alternative air source Octopus regulator Pony bottle Bolt snap Buddy line Dive light Diver's cutting tool Diver's knife Diver's telephone Through-water communications Diving bell Diving safety harness Emergency gas supply Bailout block Bailout bottle Lifeline Screw gate carabiner Emergency locator beacon Rescue tether Safety helmet Shark-proof cage Snoopy loop Navigation equipment Distance line Diving compass Dive reel Line marker Surface marker buoy Silt screw Underwater breathing apparatus Atmospheric diving suit Diving cylinder Burst disc Diving cylinder valve Diving helmet Reclaim helmet Diving regulator Mechanism of diving regulators Regulator malfunction Regulator freeze Single-hose regulator Twin-hose regulator Full face diving mask Open-circuit scuba Scuba set Bailout bottle Decompression cylinder Independent doubles Manifolded twin set Scuba manifold Pony bottle Scuba configuration Sidemount Sling cylinder Diving rebreathers Carbon dioxide scrubber Carleton CDBA CDLSE Cryogenic rebreather CUMA DSEA Dolphin Electro-galvanic oxygen sensor FROGS Halcyon PVR-BASC Halcyon RB80 IDA71 Interspiro DCSC KISS LAR-5 LAR-6 LAR-V LARU Porpoise Ray Siebe Gorman CDBA Siva Viper Surface-supplied diving equipment Air line Diver's umbilical Diving air compressor Gas panel Hookah Scuba replacement Sea Trek Snuba Standard diving dress Escape set Davis Submerged Escape Apparatus Momsen lung Steinke hood Submarine Escape Immersion Equipment Diving equipment manufacturers AP Diving Apeks Aqua Lung America Aqua Lung/La Spirotechnique Beuchat René Cavalero Cis-Lunar Cressi-Sub Dacor DESCO Dive Xtras Divex Diving Unlimited International Drägerwerk Fenzy Maurice Fernez Technisub Oscar Gugen Heinke HeinrichsWeikamp Johnson Outdoors Mares Morse Diving Nemrod Oceanic Worldwide Porpoise Sub Sea Systems Shearwater Research Siebe Gorman Submarine Products Suunto Diving support equipment Access equipment Boarding stirrup Diver lift Diving bell Diving ladder Diving platform (scuba) Diving stage Downline Jackstay Launch and recovery system Messenger line Moon pool Breathing gas handling Air filtration Activated carbon Hopcalite Molecular sieve Silica gel Booster pump Carbon dioxide scrubber Cascade filling system Diver's pump Diving air compressor Diving air filter Water separator High pressure breathing air compressor Low pressure breathing air compressor Gas blending Gas blending for scuba diving Gas panel Gas reclaim system Gas storage bank Gas storage quad Gas storage tube Helium analyzer Nitrox production Membrane gas separation Pressure swing adsorption Oxygen analyser Oxygen compatibility Decompression equipment Built-in breathing system Decompression tables Diving bell Bell cursor Closed bell Clump weight Launch and recovery system Wet bell Diving chamber Diving stage Recreational Dive Planner Saturation system Platforms Dive boat Canoe and kayak diving Combat Rubber Raiding Craft Liveaboard Subskimmer Diving support vessel HMS Challenger (K07) Underwater habitat Aquarius Reef Base Continental Shelf Station Two Helgoland Habitat Jules' Undersea Lodge Scott Carpenter Space Analog Station SEALAB Tektite habitat Remotely operated underwater vehicles 8A4-class ROUV ABISMO Atlantis ROV Team CURV Deep Drone Épaulard Global Explorer ROV Goldfish-class ROUV Kaikō ROV Kaşif ROUV Long-Term Mine Reconnaissance System Mini Rover ROV OpenROV ROV KIEL 6000 ROV PHOCA Scorpio ROV Sea Dragon-class ROV Seabed tractor Seafox drone Seahorse ROUV SeaPerch SJT-class ROUV T1200 Trenching Unit VideoRay UROVs Safety equipment Diver down flag Diving shot Hyperbaric lifeboat Hyperbaric stretcher Jackstay Jonline Reserve gas supply General Diving spread Air spread Saturation spread Hot water system Sonar Underwater acoustic positioning system Underwater acoustic communication Freediving Activities Aquathlon Apnoea finswimming Freediving Haenyeo Pearl hunting Ama Snorkeling Spearfishing Underwater football Underwater hockey Underwater ice hockey Underwater rugby Underwater target shooting Competitions Nordic Deep Vertical Blue Disciplines Constant weight (CWT) Constant weight without fins (CNF) Dynamic apnea (DYN) Dynamic apnea without fins (DNF) Free immersion (FIM) No-limits apnea (NLT) Static apnea (STA) Skandalopetra diving Variable weight apnea (VWT) Variable weight apnea without fins Equipment Diving mask Diving suit Hawaiian sling Polespear Snorkel (swimming) Speargun Swimfins Monofin Water polo cap Freedivers Deborah Andollo Peppo Biscarini Sara Campbell Derya Can Göçen Goran Čolak Carlos Coste Robert Croft Mandy-Rae Cruickshank Yasemin Dalkılıç Leonardo D'Imporzano Flavia Eberhard Şahika Ercümen Emma Farrell Francisco Ferreras Pierre Frolla Flavia Eberhard Mehgan Heaney-Grier Elisabeth Kristoffersen Loïc Leferme Enzo Maiorca Jacques Mayol Audrey Mestre Karol Meyer Stéphane Mifsud Alexey Molchanov Natalia Molchanova Dave Mullins Patrick Musimu Guillaume Néry Herbert Nitsch Umberto Pelizzari Annelie Pompe Michal Risian Stig Severinsen Tom Sietas Aharon Solomons Martin Štěpánek Walter Steyn Tanya Streeter William Trubridge Devrim Cenk Ulusoy Danai Varveri Alessia Zecchini Nataliia Zharkova Hazards Barotrauma Drowning Freediving blackout Deep-water blackout Shallow-water blackout Hypercapnia Hypothermia Historical Ama Octopus wrestling Swimming at the 1900 Summer Olympics – Men's underwater swimming Organisations AIDA International Scuba Schools International Australian Underwater Federation British Freediving Association Confédération Mondiale des Activités Subaquatiques Fédération Française d'Études et de Sports Sous-Marins Performance Freediving International Professional diving Occupations Ama Commercial diver Commercial offshore diver Hazmat diver Divemaster Diving instructor Diving safety officer Diving superintendent Diving supervisor Haenyeo Media diver Police diver Public safety diver Scientific diver Underwater archaeologist Military diving Army engineer diver Clearance diver Frogman List of military diving units Royal Navy ships diver Special Boat Service United States military divers U.S. ... Vandenberg HMS Ghurka Glen Strathallan SAS Good Hope Gothenburg Herzogin Cecilie Hilma Hooker Hispania HMS Hood HMAS Hobart Igara James Eagan Layne Captain Keith Tibbetts King Cruiser SMS Kronprinz Kyarra HMS Laforey USAT Liberty Louis Sheid USS LST-507 SMS Markgraf Mikhail Lermontov HMS M2 Maine Maloja HMS Maori Marguerite SS Mauna Loa USAT Meigs Mendi USCGC Mohawk Mohegan RMS Moldavia HMS Montagu MV RMS Mulheim Nagato Oceana USS Oriskany Oslofjord P29 P31 Pedernales Persier HMAS Perth SAS Pietermaritzburg Piłsudski Pool Fisher HMS Port Napier Preußen President Coolidge PS Queen Victoria Radaas Rainbow Warrior RMS Rhone Rondo Rosehill Rotorua Royal Adelaide Royal Charter Rozi HMS Safari Salem Express USS Saratoga USS Scuffle HMS Scylla HMS Sidon USS Spiegel Grove Stanegarth Stanwood Stella HMAS Swan USS Tarpon Thesis Thistlegorm Toa Maru Torrey Canyon SAS Transvaal U-40 U-352 U-1195 Um El Faroud Varvassi Walter L M Russ Washingtonian (1913) HMNZS Wellington USS Yancey Yongala Zenobia Zealandia Zingara Cave diving sites Blauhöhle Chinhoyi Caves Devil's Throat at Punta Sur Engelbrecht Cave Fossil Cave Jordbrugrotta Piccaninnie Ponds Pluragrotta Pollatoomary Sistema Ox Bel Ha Sistema Sac Actun Sistema Dos Ojos Sistema Nohoch Nah Chich Freshwater dives Dutch Springs Ewens Ponds Little Blue Lake Training sites Capernwray Dive Centre Deepspot National Diving and Activity Centre Stoney Cove Open ocean diving Blue-water diving Black-water diving Diving safety Human factors in diving equipment design Human factors in diving safety Life-support system Safety-critical system Scuba diving fatalities Diving hazards List of diving hazards and precautions Environmental Current Delta-P Entanglement hazard Overhead Silt out Wave action Equipment Freeflow Use of breathing equipment in an underwater environment Failure of diving equipment other than breathing apparatus Single point of failure Physiological Cold shock response Decompression Nitrogen narcosis Oxygen toxicity Seasickness Uncontrolled decompression Diver behaviour and competence Lack of competence Overconfidence effect Panic Task loading Trait anxiety Willful violation Consequences Barotrauma Decompression sickness Drowning Hypothermia Hypoxia Hypercapnia Hyperthermia Diving procedures Ascending and descending Emergency ascent Boat diving Canoe and kayak diving Buddy diving buddy check Decompression Decompression practice Pyle stop Ratio decompression Dive briefing Dive log Dive planning Scuba gas planning Diver communications Diving hand signals Diving line signals Diver voice communications Diver rescue Diver training Doing It Right Drift diving Gas blending for scuba diving Night diving Solo diving Water safety Risk management Checklist Hazard identification and risk assessment Hazard analysis Job safety analysis Risk assessment Risk control Hierarchy of hazard controls Incident pit Lockout–tagout Permit To Work Redundancy Safety data sheet Situation awareness Diving team Bellman Chamber operator Diver medical technician Diver's attendant Diving supervisor Diving systems technician Gas man Life support technician Stand-by diver Equipment safety Breathing gas quality Testing and inspection of diving cylinders Hydrostatic test Sustained load cracking Diving regulator Breathing performance of regulators Occupational safety and health Approaches to safety Job safety analysis Risk assessment Toolbox talk Housekeeping Association of Diving Contractors International Code of practice Contingency plan Diving regulations Emergency procedure Emergency response plan Evacuation plan Hazardous Materials Identification System Hierarchy of hazard controls Administrative controls Engineering controls Hazard elimination Hazard substitution Personal protective equipment International Marine Contractors Association Occupational hazard Biological hazard Chemical hazard Physical hazard Psychosocial hazard Occupational hygiene Exposure assessment Occupational exposure limit Workplace health surveillance Safety culture Code of practice Diving safety officer Diving superintendent Health and safety representative Operations manual Safety meeting Standard operating procedure Diving medicine Diving disorders List of signs and symptoms of diving disorders Cramp Motion sickness Surfer's ear Pressure related Alternobaric vertigo Barostriction Barotrauma Air embolism Aerosinusitis Barodontalgia Dental barotrauma Pulmonary barotrauma Compression arthralgia Decompression illness Dysbarism Oxygen Freediving blackout Hyperoxia Hypoxia Oxygen toxicity Inert gases Avascular necrosis Decompression sickness Isobaric counterdiffusion Taravana Dysbaric osteonecrosis High-pressure nervous syndrome Hydrogen narcosis Nitrogen narcosis Carbon dioxide Hypercapnia Hypocapnia Breathing gas contaminants Carbon monoxide poisoning Immersion related Asphyxia Drowning Hypothermia Immersion diuresis Instinctive drowning response Laryngospasm Salt water aspiration syndrome Swimming-induced pulmonary edema Treatment Demand valve oxygen therapy First aid Hyperbaric medicine Hyperbaric treatment schedules In-water recompression Oxygen therapy Therapeutic recompression Personnel Diving Medical Examiner Diving Medical Practitioner Diving Medical Technician Hyperbaric nursing Screening Atrial septal defect Effects of drugs on fitness to dive Fitness to dive Psychological fitness to dive Research Researchers in diving physiology and medicine Arthur J.

-
Tuberous Sclerosis 1
Omim
Cardiac rhythm disturbances were found in 13. Wolff-Parkinson-White syndrome (WPW; 194200) was documented in 6, 4 of whom presented paroxysmal arrhythmias. ... O'Callaghan et al. (1998) identified 10 patients with concurrent diagnoses of WPW syndrome and tuberous sclerosis. WPW presented early in life, 9 cases being diagnosed in the first year. Eight of 10 cases were male. In 8 cases, the syndrome was associated with supraventricular tachycardias, and in 9 with cardiac rhabdomyomas. ... Contrary to the findings with other dominant disorders such as achondroplasia (ACH; 100800), Apert syndrome (101200), and fibrodysplasia ossificans (FOP; 135100), no increase in parental age has been found in sporadic (presumably new mutation) cases of tuberous sclerosis (Gunther and Penrose, 1935; Borberg, 1951; Nevin and Pearce, 1968; Bundey and Evans, 1969). ... Hall and Byers (1987) suggested that gonadal mosaicism may be responsible for recurrence of tuberous sclerosis in sibs in the same manner as has been reported for osteogenesis imperfecta congenita, pseudoachondroplasia, achondroplasia, and Apert syndrome. Rott and Fahsold (1991) described affected brother and sister whose parents were normal by extensive examinations that included x-ray computerized tomography of brain, liver, and kidneys, echocardiography, and MR imaging of the brain.TSC2, TSC1, IFNG, EIF4EBP1, PKD1, PIK3CB, TESC, SLC12A3, PIK3CD, PIK3CG, MTOR, PIK3CA, PTEN, AKT1, TP53, STK11, IGF1, RPS6KB1, DDIT4, TYMS, RASA1, OGG1, BRAF, IL1B, CCL26, VDR, IL6, PRKAA1, PRKAA2, PRKAB1, RHEB, MAPK1, GH1, PRKD1, MIR21, ABCB1, TBC1D7, PTGS2, BCL2L11, GRM5, COX2, MFAP1, MEN1, RGS6, NF1, FMR1, VIM, TERF2IP, PCNA, RABGEF1, CRTC1, VEGFA, VEGFC, PTPN4, MIR147B, MIR146A, MIR132, RPS6, C20orf181, TNF, RAP1A, FLCN, MTCO2P12, EGF, ABO, EPHB2, MAPK3, EGFR, APRT, DCX, LRPPRC, ST14, SPP1, AKT3, DEPDC5, STIM1, SPINT1, GRAP2, ADIPOQ, LILRB2, KLF4, STAT3, IRS2, CDK5R1, RIPK2, ELOC, TCOF1, GLRX3, CASK, IKBKG, SLC7A5, HMGA2, AIMP2, YWHAZ, YWHAB, TFRC, TRPC4, TYR, ZNRD2, ABCA4, AHSA1, WNT3A, ARID1B, RPTOR, CIP2A, GRHL3, IL21, NEUROG2, DHDDS, FUZ, COL18A1, CCDC8, BEX2, ORAI1, LINGO1, UBASH3B, CDCA5, DCTN6, PLB1, RMDN2, MARCHF10, HEXD, TICAM2, MIR142, MIR223, PIM3, OPN1MW2, IH, TMED7-TICAM2, FECD3, OPN1MW3, UPK3B, SLC12A5, RALGAPB, CHPT1, WDR45B, TNFSF13B, OGA, NES, UTS2, TRIM31, WDR45, PARK7, DKK1, TBC1D9, PHLPP1, RPGRIP1L, MLYCD, AMACR, PPP1R15A, RNF19A, POLDIP2, BEX3, LAT, SGSM3, NOX4, IL21R, IL22, TMED7, RMDN1, TLR7, TNFRSF12A, IL23A, RMDN3, SYBU, SOX9, PSMD9, SLC12A2, CTLA4, DBH, DECR1, NQO1, EIF4G1, EREG, PTK2B, FCN2, FLNA, FLT1, FLT4, GABPA, GC, GCHFR, OPN1MW, GFAP, GJA1, GCLC, GNA11, GNA12, GPT, GRN, GRIN2C, GSK3B, HCRT, HGF, HMBS, HRAS, CTNNB1, CCN2, SLC2A1, CSF2, ACTB, AGER, AKT2, AMELX, AMH, ANXA1, ANXA6, AQP4, ARNTL, ATM, KIF1A, CCND1, BCL2, OPN1SW, BDNF, BMP4, C1QBP, CANX, CBR1, CD8A, CDK7, CDKN2A, CDX2, CLN3, CMM, CRK, MAPK14, HTR2C, ICAM1, IFI27, IKBKB, TNFRSF11B, PRDX1, PAH, PAK2, PAM, PDCD1, PDGFRB, PEX13, PIK3C3, PITX1, PLA2G1B, PLCD1, PLG, PRRX1, POMC, ABL1, PTGS1, PVALB, RAP1GAP, RBBP4, S100A1, S100B, CCL2, CCL24, SDC2, SDHB, SHOX, NTF4, NTF3, NPC1, MME, IL4, IL6ST, CXCL8, IL12A, IL17A, ING2, INHA, IRF7, IRS1, KRAS, LAMC2, LIG4, MMP2, NOTCH1, MNAT1, MPP2, ABCC1, MYO1B, COX1, MTTP, MUC1, MYC, NFE2L2, NFKB1, NGF, NM, H3P23

-
Acute Liver Failure
Wikipedia
Thrombocytopenia with or without DIC increases risk of intracerebral bleeding. [6] Kidney failure [ edit ] Kidney failure is common, present in more than 50% of ALF patients, either due to original insult such as paracetamol resulting in acute tubular necrosis or from hyperdynamic circulation leading to hepatorenal syndrome or functional kidney failure. Because of impaired production of urea, blood urea does not represent the degree of kidney impairment. Inflammation and infection [ edit ] About 60% of all ALF patients fulfil the criteria for systemic inflammatory syndrome irrespective of presence or absence of infection. [7] This often contributes towards multi organ failure . ... "Acute liver failure: redefining the syndromes". Lancet . 342 (8866): 273–5. doi : 10.1016/0140-6736(93)91818-7 . ... "Prognostic implications of hyperlactatemia, multiple organ failure, and systemic inflammatory response syndrome in patients with acetaminophen-induced acute liver failure" . ... External links [ edit ] Fulminant Hepatic Failure at eMedicine Classification D ICD - 10 : K72 ICD - 9-CM : 570 MeSH : D017114 External resources eMedicine : article/177354 v t e Diseases of the digestive system Upper GI tract Esophagus Esophagitis Candidal Eosinophilic Herpetiform Rupture Boerhaave syndrome Mallory–Weiss syndrome UES Zenker's diverticulum LES Barrett's esophagus Esophageal motility disorder Nutcracker esophagus Achalasia Diffuse esophageal spasm Gastroesophageal reflux disease (GERD) Laryngopharyngeal reflux (LPR) Esophageal stricture Megaesophagus Esophageal intramural pseudodiverticulosis Stomach Gastritis Atrophic Ménétrier's disease Gastroenteritis Peptic (gastric) ulcer Cushing ulcer Dieulafoy's lesion Dyspepsia Pyloric stenosis Achlorhydria Gastroparesis Gastroptosis Portal hypertensive gastropathy Gastric antral vascular ectasia Gastric dumping syndrome Gastric volvulus Buried bumper syndrome Gastrinoma Zollinger–Ellison syndrome Lower GI tract Enteropathy Small intestine ( Duodenum / Jejunum / Ileum ) Enteritis Duodenitis Jejunitis Ileitis Peptic (duodenal) ulcer Curling's ulcer Malabsorption : Coeliac Tropical sprue Blind loop syndrome Small bowel bacterial overgrowth syndrome Whipple's Short bowel syndrome Steatorrhea Milroy disease Bile acid malabsorption Large intestine ( Appendix / Colon ) Appendicitis Colitis Pseudomembranous Ulcerative Ischemic Microscopic Collagenous Lymphocytic Functional colonic disease IBS Intestinal pseudoobstruction / Ogilvie syndrome Megacolon / Toxic megacolon Diverticulitis / Diverticulosis / SCAD Large and/or small Enterocolitis Necrotizing Gastroenterocolitis IBD Crohn's disease Vascular : Abdominal angina Mesenteric ischemia Angiodysplasia Bowel obstruction : Ileus Intussusception Volvulus Fecal impaction Constipation Diarrhea Infectious Intestinal adhesions Rectum Proctitis Radiation proctitis Proctalgia fugax Rectal prolapse Anismus Anal canal Anal fissure / Anal fistula Anal abscess Hemorrhoid Anal dysplasia Pruritus ani GI bleeding Blood in stool Upper Hematemesis Melena Lower Hematochezia Accessory Liver Hepatitis Viral hepatitis Autoimmune hepatitis Alcoholic hepatitis Cirrhosis PBC Fatty liver NASH Vascular Budd–Chiari syndrome Hepatic veno-occlusive disease Portal hypertension Nutmeg liver Alcoholic liver disease Liver failure Hepatic encephalopathy Acute liver failure Liver abscess Pyogenic Amoebic Hepatorenal syndrome Peliosis hepatis Metabolic disorders Wilson's disease Hemochromatosis Gallbladder Cholecystitis Gallstone / Cholelithiasis Cholesterolosis Adenomyomatosis Postcholecystectomy syndrome Porcelain gallbladder Bile duct / Other biliary tree Cholangitis Primary sclerosing cholangitis Secondary sclerosing cholangitis Ascending Cholestasis / Mirizzi's syndrome Biliary fistula Haemobilia Common bile duct Choledocholithiasis Biliary dyskinesia Sphincter of Oddi dysfunction Pancreatic Pancreatitis Acute Chronic Hereditary Pancreatic abscess Pancreatic pseudocyst Exocrine pancreatic insufficiency Pancreatic fistula Other Hernia Diaphragmatic Congenital Hiatus Inguinal Indirect Direct Umbilical Femoral Obturator Spigelian Lumbar Petit's Grynfeltt-Lesshaft Undefined location Incisional Internal hernia Richter's Peritoneal Peritonitis Spontaneous bacterial peritonitis Hemoperitoneum Pneumoperitoneum v t e Intensive care medicine Health science Medicine Medical specialities Respiratory therapy General terms Intensive care unit (ICU) Neonatal intensive care unit (NICU) Pediatric intensive care unit (PICU) Coronary care unit (CCU) Critical illness insurance Conditions Organ system failure Shock sequence SIRS Sepsis Severe sepsis Septic shock Multiple organ dysfunction syndrome Other shock Cardiogenic shock Distributive shock Anaphylaxis Obstructive shock Neurogenic shock Spinal shock Vasodilatory shock Organ failure Acute renal failure Acute respiratory distress syndrome Acute liver failure Respiratory failure Multiple organ dysfunction syndrome Neonatal infection Polytrauma Coma Complications Critical illness polyneuropathy / myopathy Critical illness–related corticosteroid insufficiency Decubitus ulcers Fungemia Stress hyperglycemia Stress ulcer Iatrogenesis Methicillin-resistant Staphylococcus aureus Oxygen toxicity Refeeding syndrome Ventilator-associated lung injury Ventilator-associated pneumonia Dialytrauma Diagnosis Arterial blood gas Catheter Arterial line Central venous catheter Pulmonary artery catheter Blood cultures Screening cultures Life-supporting treatments Airway management Chest tube Dialysis Enteral feeding Goal-directed therapy Induced coma Mechanical ventilation Therapeutic hypothermia Total parenteral nutrition Tracheal intubation Drugs Analgesics Antibiotics Antithrombotics Inotropes Intravenous fluids Neuromuscular-blocking drugs Recombinant activated protein C Sedatives Stress ulcer prevention drugs Vasopressors ICU scoring systems APACHE II Glasgow Coma Scale PIM2 SAPS II SAPS III SOFA Physiology Hemodynamics Hypotension Level of consciousness Acid–base imbalance Water-electrolyte imbalance Organisations Society of Critical Care Medicine Surviving Sepsis Campaign European Society of Paediatric and Neonatal Intensive Care Related specialties Anesthesiology Cardiology Internal medicine Neurology Pediatrics Pulmonology Surgery Traumatology v t e Organ failure General Heart failure Respiratory failure Liver failure Acute Chronic Renal failure Acute Chronic Encephalopathy Multiple Multiple organ dysfunction syndromeTNF, ATP7B, HGF, FAS, ALB, IL1RN, GC, MAPK8, KRT8, KRT18, GFER, FASLG, CSF3, SERPINC1, CAST, GPNMB, PANX1, CD74, FST, POMC, SCO1, ALDOB, INHBA, INS, IL6, TLR4, CASP3, NOS3, PTGS2, ABCC2, NOS2, MET, CD14, CASP9, ATM, KCNJ10, PTAFR, CASP12, UCP2, COL1A2, HSPA8, FGA, BRIP1, THBD, INS-IGF2, LTC4S, NBAS, POLG, RINT1, TRMU, FAH, POLG2, JAK2, SCYL1, MST1, PORCN, HADH, GPT, GPR35, VPS13A, MPV17, ITCH, F5, CYC1, RYR1, GFM1, ACAD9, IKZF1, MEFV, CACNA1S, EIF2AK3, LARS1, TCF4, HLA-B, HMGB1, IL1B, F2, CCL4, IL10, MIR122, HMOX1, PPARA, STON1, AFM, GTF2A1L, MIR223, NLRP3, SLC1A2, HDAC2, STON1-GTF2A1L, HDAC6, MSC, IL1A, UGT1A, TP53, SLC17A5, ABCG2, SYT1, CXCL12, PEBP1, OTC, PRKAA1, RELA, WNK1, BCHE, AFP, IFNG, AHSG, GORASP1, GSK3B, PIM3, DDIT3, DGUOK, EXOSC3, BCL2L11, MIR17, MFN2, MIR155, ABCB6, AIM2, BTBD8, YAP1, IFNL3, PPARGC1B, APOA5, PIK3IP1, LMLN, MIR19A, LONP1, MIR210, ATG7, PPIG, MIR214, RGN, TIMELESS, SQSTM1, MIR375, MIR1224, TNFRSF10B, RIPK1, OCLN, BECN1, SOCS1, ARHGEF5, SHANK3, KHDRBS1, TXNIP, KCTD9, HAMP, ACKR3, NAT10, HAVCR1, SIGLEC9, PDLIM3, IGHV1-3, ATRNL1, TLR9, STX18, ERO1A, SCLC1, RRM2B, SLC25A37, CXCL16, NUP62, SERAC1, SLC27A5, DCTN4, CYSLTR1, CCL27, SLA2, EVA1A, TMPRSS13, SESN2, SIRT1, PARP9, ASRGL1, DHDDS, GSDMD, SIRT2, TBC1D9, TFEB, ACADM, VWF, GABPA, CYP2E1, CYP3A4, ESR1, FABP1, FABP7, FBP1, FCGR3A, FCGR3B, FOXO3, G6PD, GFAP, VIP, CXCR3, GTF2H1, HIF1A, HNF4A, HSPA5, HSPG2, ID1, IFNA1, IFNA13, IFNB1, CYP1A2, CX3CR1, CTNNB1, CTLA4, AHR, AKT1, ALAS1, ALPP, AMCN, AQP4, AR, ATHS, BCL2, OPN1SW, BID, BST2, CASP8, CD86, ENTPD1, CD40LG, CEL, CGA, CCR5, KLF6, CRP, IL1R1, IL2, CXCL8, S100A10, CCL2, SDC1, SLC6A12, SLC12A2, SLPI, SOAT1, STAR, STAT1, STAT3, MAP3K7, PPP1R11, TGFB1, TGFBR2, THBS1, THPO, TLR2, TLR3, TNFAIP3, TNFAIP6, TXN, UGT2B7, S100A12, RHD, IL18, ACP3, ITGAM, MARS1, KMT2A, MPO, MSMB, COX2, MYD88, NFE2L2, NT5E, SERPINE1, ABCB1, PIK3CA, PIK3CB, PIM1, PIK3CD, PIK3CG, SERPINF2, PPP2R5A, PRKAA2, PRKAB1, RBP4, MTCO2P12

-
Diffuse Panbronchiolitis
Wikipedia
In addition, diseases caused by identified HLA genes in the DPB-susceptibility region have been investigated. One of these, bare lymphocyte syndrome I (BLS I), exhibits a number of similarities with DPB in those affected, including chronic sinusitis, bronchiolar inflammation and nodules, and the presence of H. influenzae . ... External links [ edit ] Classification D ICD - 10 : J21.9 ICD - 9-CM : 466.1 OMIM : 604809 MeSH : C536174 DiseasesDB : 3804 SNOMED CT : 430476004 External resources Orphanet : 171700 v t e Diseases of the respiratory system Upper RT (including URTIs , common cold ) Head sinuses Sinusitis nose Rhinitis Vasomotor rhinitis Atrophic rhinitis Hay fever Nasal polyp Rhinorrhea nasal septum Nasal septum deviation Nasal septum perforation Nasal septal hematoma tonsil Tonsillitis Adenoid hypertrophy Peritonsillar abscess Neck pharynx Pharyngitis Strep throat Laryngopharyngeal reflux (LPR) Retropharyngeal abscess larynx Croup Laryngomalacia Laryngeal cyst Laryngitis Laryngopharyngeal reflux (LPR) Laryngospasm vocal cords Laryngopharyngeal reflux (LPR) Vocal fold nodule Vocal fold paresis Vocal cord dysfunction epiglottis Epiglottitis trachea Tracheitis Laryngotracheal stenosis Lower RT / lung disease (including LRTIs ) Bronchial / obstructive acute Acute bronchitis chronic COPD Chronic bronchitis Acute exacerbation of COPD ) Asthma ( Status asthmaticus Aspirin-induced Exercise-induced Bronchiectasis Cystic fibrosis unspecified Bronchitis Bronchiolitis Bronchiolitis obliterans Diffuse panbronchiolitis Interstitial / restrictive ( fibrosis ) External agents/ occupational lung disease Pneumoconiosis Aluminosis Asbestosis Baritosis Bauxite fibrosis Berylliosis Caplan's syndrome Chalicosis Coalworker's pneumoconiosis Siderosis Silicosis Talcosis Byssinosis Hypersensitivity pneumonitis Bagassosis Bird fancier's lung Farmer's lung Lycoperdonosis Other ARDS Combined pulmonary fibrosis and emphysema Pulmonary edema Löffler's syndrome / Eosinophilic pneumonia Respiratory hypersensitivity Allergic bronchopulmonary aspergillosis Hamman-Rich syndrome Idiopathic pulmonary fibrosis Sarcoidosis Vaping-associated pulmonary injury Obstructive / Restrictive Pneumonia / pneumonitis By pathogen Viral Bacterial Pneumococcal Klebsiella Atypical bacterial Mycoplasma Legionnaires' disease Chlamydiae Fungal Pneumocystis Parasitic noninfectious Chemical / Mendelson's syndrome Aspiration / Lipid By vector/route Community-acquired Healthcare-associated Hospital-acquired By distribution Broncho- Lobar IIP UIP DIP BOOP-COP NSIP RB Other Atelectasis circulatory Pulmonary hypertension Pulmonary embolism Lung abscess Pleural cavity / mediastinum Pleural disease Pleuritis/pleurisy Pneumothorax / Hemopneumothorax Pleural effusion Hemothorax Hydrothorax Chylothorax Empyema/pyothorax Malignant Fibrothorax Mediastinal disease Mediastinitis Mediastinal emphysema Other/general Respiratory failure Influenza Common cold SARS Coronavirus disease 2019 Idiopathic pulmonary haemosiderosis Pulmonary alveolar proteinosisMUCL3, MUC5B, HLA-B, HLA-A, ERCC2, ITGB2, GTF2H5, TENT5A, FEV, SEC14L2, NXF1, USO1, MLN, MBL2, ITGAL, ERCC3, ITGA4, IL17A, CXCL8, GTF2H4, GTF2H3, GTF2H2, GTF2H1, GC, FLNB, MUC22

-
Testicular Germ Cell Tumor
Omim
Gustavson et al. (1975) reported bilateral testicular teratoma in 2 infant brothers with XXY Klinefelter syndrome. One of them also had hydrocephalus due to stenosis of the aqueduct of Sylvius. Familial occurrence of the Klinefelter syndrome is rare. The association of the Klinefelter syndrome and testicular teratoma may be more than coincidental because they have been observed together in other cases and many testicular teratoma are both X-chromatin and Y-chromatin positive suggesting that they are XXY. ... Huddart et al. (1996) noted that none of these families had any features indicative of the Li-Fraumeni syndrome (151623) or any other cancer family syndrome. ... INHERITANCE - Somatic mutation GENITOURINARY Internal Genitalia (Male) - Painless testicular mass NEOPLASIA - Male germ cell tumors (GCT), 2 subtypes - - Seminoma - Nonseminoma (embryonal carcinoma, teratoma, choriocarcinoma, endodermal sinus tumor) LABORATORY ABNORMALITIES - Isochromosome 12p (i(12p)) - Elevated hCG (choriocarcinoma) - Elevated AFP (endodermal sinus tumor) - Elevated hCG or AFP or both (embryonal carcinoma) - Azoospermia/oligospermia (present at diagnosis) MISCELLANEOUS - Two subtypes - seminoma and nonseminoma - Occasionally germ cell tumor arise from extra gonadal site (e.g., mediastinum, retroperitoneum, pineal gland) - Most common cancer in men aged 15-40 years - Highest incidence in men of European descent - Risk factors for development of TGCT - family history, cryptorchidism ( 219050 ), testicular feminization ( 300068 ), Klinefelter syndrome, previous TGCT, gonadal dysgenesis ▲ Close
-
Mania
Wikipedia
State of abnormally elevated or irritable mood, arousal, and/or energy levels Mania Other names Manic syndrome, manic episode Graphical representation of mania and hypomania Specialty Psychiatry Mania , also known as manic syndrome , is a state of abnormally elevated arousal, affect , and energy level, or "a state of heightened overall activation with enhanced affective expression together with lability of affect." [1] During a manic episode, an individual will experience rapidly changing emotions and moods, highly influenced by surrounding stimuli. ... However, in full-blown mania, they undergo progressively severe exacerbations and become more and more obscured by other signs and symptoms, such as delusions and fragmentation of behavior. [3] Contents 1 Causes and diagnosis 2 Classification 2.1 Mixed states 2.2 Hypomania 2.3 Associated disorders 3 Signs and symptoms 4 Cause 5 Mechanism 6 Diagnosis 7 Treatment 8 Society and culture 9 Etymology 10 See also 11 References 12 Further reading 13 External links Causes and diagnosis [ edit ] Mania is a syndrome with multiple causes. Although the vast majority of cases occur in the context of bipolar disorder , it is a key component of other psychiatric disorders (such as schizoaffective disorder , bipolar type) and may also occur secondary to various general medical conditions, such as multiple sclerosis ; certain medications may perpetuate a manic state, for example prednisone ; or substances prone to abuse, especially stimulants, such as caffeine and cocaine . ... Lifestyle triggers include irregular sleep-wake schedules and sleep deprivation, as well as extremely emotional or stressful stimuli. [23] Various genes that have been implicated in genetic studies of bipolar have been manipulated in preclinical animal models to produce syndromes reflecting different aspects of mania. ... The latter finding was interpreted in the context of either elevated baseline activity (resulting in a null finding of reward hypersensitivity), or reduced ability to discriminate between reward and punishment, still supporting reward hyperactivity in mania. [39] Punishment hyposensitivity , as reflected in a number of neuroimaging studies as reduced lateral orbitofrontal response to punishment, has been proposed as a mechanism of reward hypersensitivity in mania. [40] Diagnosis [ edit ] In the ICD-10 there are several disorders with the manic syndrome: organic manic disorder ( F06.30 ), mania without psychotic symptoms ( F30.1 ), mania with psychotic symptoms ( F30.2 ), other manic episodes ( F30.8 ), unspecified manic episode ( F30.9 ), manic type of schizoaffective disorder ( F25.0 ), bipolar affective disorder , current episode manic without psychotic symptoms ( F31.1 ), bipolar affective disorder, current episode manic with psychotic symptoms ( F31.2 ). ... Goodwin Kay Redfield Jamison Symptoms Hallucination Delusion Emotional dysregulation Anhedonia Dysphoria Suicidal ideation Mood swing Sleep disorder Hypersomnia Insomnia Psychosis Racing thoughts Reduced affect display Depression (differential diagnoses) Spectrum Bipolar disorder Bipolar I Bipolar II Cyclothymia Bipolar NOS Depression Major depressive disorder Dysthymia Seasonal affective disorder Atypical depression Melancholic depression Schizoaffective disorder Mania Mixed affective state Hypomania Major depressive episode Rapid cycling Treatment Anticonvulsants Carbamazepine Lamotrigine Oxcarbazepine Valproate Sodium valproate Valproate semisodium Sympathomimetics , SSRIs and similar Dextroamphetamine Methylphenidate Bupropion Sertraline Fluoxetine Escitalopram Other mood stabilizers Antipsychotics Lithium Lithium carbonate Lithium citrate Lithium sulfate Lithium toxicity Atypical antipsychotics Non-pharmaceutical Clinical psychology Electroconvulsive therapy Involuntary commitment Light therapy Psychotherapy Transcranial magnetic stimulation Cognitive behavioral therapy Dialectical behavior therapy v t e Mental and behavioral disorders Adult personality and behavior Gender dysphoria Ego-dystonic sexual orientation Paraphilia Fetishism Voyeurism Sexual maturation disorder Sexual relationship disorder Other Factitious disorder Munchausen syndrome Intermittent explosive disorder Dermatillomania Kleptomania Pyromania Trichotillomania Personality disorder Childhood and learning Emotional and behavioral ADHD Conduct disorder ODD Emotional and behavioral disorders Separation anxiety disorder Movement disorders Stereotypic Social functioning DAD RAD Selective mutism Speech Stuttering Cluttering Tic disorder Tourette syndrome Intellectual disability X-linked intellectual disability Lujan–Fryns syndrome Psychological development ( developmental disabilities ) Pervasive Specific Mood (affective) Bipolar Bipolar I Bipolar II Bipolar NOS Cyclothymia Depression Atypical depression Dysthymia Major depressive disorder Melancholic depression Seasonal affective disorder Mania Neurological and symptomatic Autism spectrum Autism Asperger syndrome High-functioning autism PDD-NOS Savant syndrome Dementia AIDS dementia complex Alzheimer's disease Creutzfeldt–Jakob disease Frontotemporal dementia Huntington's disease Mild cognitive impairment Parkinson's disease Pick's disease Sundowning Vascular dementia Wandering Other Delirium Organic brain syndrome Post-concussion syndrome Neurotic , stress -related and somatoform Adjustment Adjustment disorder with depressed mood Anxiety Phobia Agoraphobia Social anxiety Social phobia Anthropophobia Specific social phobia Specific phobia Claustrophobia Other Generalized anxiety disorder OCD Panic attack Panic disorder Stress Acute stress reaction PTSD Dissociative Depersonalization disorder Dissociative identity disorder Fugue state Psychogenic amnesia Somatic symptom Body dysmorphic disorder Conversion disorder Ganser syndrome Globus pharyngis Psychogenic non-epileptic seizures False pregnancy Hypochondriasis Mass psychogenic illness Nosophobia Psychogenic pain Somatization disorder Physiological and physical behavior Eating Anorexia nervosa Bulimia nervosa Rumination syndrome Other specified feeding or eating disorder Nonorganic sleep Hypersomnia Insomnia Parasomnia Night terror Nightmare REM sleep behavior disorder Postnatal Postpartum depression Postpartum psychosis Sexual dysfunction Arousal Erectile dysfunction Female sexual arousal disorder Desire Hypersexuality Hypoactive sexual desire disorder Orgasm Anorgasmia Delayed ejaculation Premature ejaculation Sexual anhedonia Pain Nonorganic dyspareunia Nonorganic vaginismus Psychoactive substances, substance abuse and substance-related Drug overdose Intoxication Physical dependence Rebound effect Stimulant psychosis Substance dependence Withdrawal Schizophrenia , schizotypal and delusional Delusional Delusional disorder Folie à deux Psychosis and schizophrenia-like Brief reactive psychosis Schizoaffective disorder Schizophreniform disorder Schizophrenia Childhood schizophrenia Disorganized (hebephrenic) schizophrenia Paranoid schizophrenia Pseudoneurotic schizophrenia Simple-type schizophrenia Other Catatonia Symptoms and uncategorized Impulse control disorder Klüver–Bucy syndrome Psychomotor agitation StereotypyBDNF, SLC6A4, GSK3B, SHANK3, COMT, AKR1C4, NR3C1, PREP, MMP9, CCK, STAB1, ME2, NCAN, SHANK2, HSPA4, ABCB1, GRK3, SRD5A1, GRIK2, STK4, NDUFV2, NTRK1, TENM4, MTHFR, RIMS1, TAC1, SSBP2, TACR1, TRANK1, ITIH1, NTRK2, NTNG1, PC, PDE4B, SNAP25, SLC5A3, CCL2, SCN2A, S100B, HDAC5, RPS6KA2, PVALB, RELN, SRPK2, POU3F2, ADCY2, POMC, CPLX2, CPLX1, PLEKHO1, SERPINA1, INS, ZCCHC2, ZNF592, CD47, DRD5, DRD1, DNAH8, LMAN2L, TRPM2, TSHB, NTNG2, DIXDC1, FSTL5, CACNA1D, CACNA1C, FADS2, THSD7A, ANK3, BHLHE40, ADD3, STARD9, TRPC3, GAD1, GRIN2A, MRPS33, HTR2A, PACS1, GSK3A, GAD2, SP4, SLC25A13, SLC6A3, IL6, EIF4EBP1, DLX4, NRG1, HSD3B2, JAG1, DISC1, TNF, GATA3, NOS2, NOS1, GRIA1, CRP, CLOCK, NR1H4, KL, NR1D1, ACHE, CAMKK2, ZC4H2, DAOA, ANKK1, PRRT2, DTNBP1, PARP9, BICC1, ATF7IP, TBC1D9, MOCOS, BFAR, FGF21, PER2, CD2AP, SIRT1, TIMELESS, PON1, PER3, EGF, IGFBP2, IGF1, IFNG, HINT1, H1-0, GRM2, GDNF, MTOR, FGF9, CYP19A1, IL1RN, CYP2D6, CEACAM5, CDS1, CD28, CALCA, BPI, ARNTL, AGRP, ADRB2, IGFBP3, MAFD2, KMO, PRKCA, BAS, FXR1, TP53, TLR4, TLR2, TERT, SULT2A1, S100A10, PRKCB, PIK3CG, MAOA, PIK3CD, PIK3CB, PIK3CA, P2RX7, NOTCH1, NGF, NFIX, MMP2, SMCP, C20orf181

-
Transmissible Spongiform Encephalopathy
Wikipedia
TSEs of humans include Creutzfeldt–Jakob disease —which has four main forms, the sporadic (sCJD), the hereditary/familial (fCJD), the iatrogenic (iCJD) and the variant form (vCJD)— Gerstmann–Sträussler–Scheinker syndrome , fatal familial insomnia , kuru , and the recently discovered variably protease-sensitive prionopathy and familial spongiform encephalopathy. ... Creutzfeldt–Jakob disease (CJD) CJD prion PrP sCJD No Variant Creutzfeldt–Jakob disease (vCJD, nvCJD) vCJD prion [9] PrP vCJD 90.001.0.01.009. Gerstmann-Sträussler-Scheinker syndrome (GSS) GSS prion PrP GSS No 90.001.0.01.010. ... The first case was identified as a fatal wasting syndrome in the 1960s. It was then recognized as a transmissible spongiform encephalopathy in 1978. ... "Gerstmann-Straussler-Scheinker syndrome, fatal familial insomnia, and kuru: a review of these less common human transmissible spongiform encephalopathies". ... Transmissible spongiform encephalopathy at Curlie Classification D ICD - 10 : A81 ICD - 9-CM : 046 MeSH : D017096 DiseasesDB : 25165 External resources eMedicine : neuro/662 v t e Prion diseases and transmissible spongiform encephalopathy Prion diseases in humans inherited/ PRNP : fCJD Gerstmann–Sträussler–Scheinker syndrome Fatal familial insomnia sporadic: sCJD Sporadic fatal insomnia Variably protease-sensitive prionopathy acquired/ transmissible: iCJD vCJD Kuru Prion diseases in other animals Bovine spongiform encephalopathy Camel spongiform encephalopathy Scrapie Chronic wasting disease Transmissible mink encephalopathy Feline spongiform encephalopathy Exotic ungulate encephalopathyPRNP, CX3CL1, CX3CR1, SNCA, CLU, MARK4, LINC02210-CRHR1, TOMM40, CARD14, MS4A4A, CHN2, ABCB6, ABCA7, RPS4XP2, PRDX2, PPP1R12B, CCDC62, CD2AP, SLC2A13, C4BPA, BST1, LINC02210, MS4A4E, BLOC1S3, C9orf72, ANK3, EPHA1-AS1, GH1, MAPT, CSF2, LAMC2, PRKN, APP, APOE, SOD1, HECTD2, CBLL2, MUL1, PDIK1L, NEFL, LINC01672, IGFALS, HSPA4, TNF, SPRN, MGRN1, GSS, AHSP, IL6, IL1B, IAPP, SERPINA3, GPI, ADAM10, FXN, SMUG1, MMRN1, SARM1, CHN1, SIRT3, CABIN1, CFH, CHI3L1, PRND, SEC61A1, CFL1, CD44, GDE1, TPPP, STMN2, XAF1, YWHAQ, STIP1, HPSE, CHRM1, PLK3, RABEPK, EDIL3, DNM1L, CR1, CST7, BAG6, CR2, EGLN1, FKBP10, CD40LG, CXCR5, ACHE, SNORD3A, ACTB, MIR342, MIR21, AKT1, PLCXD3, APCS, NEGR1, CALHM1, AQP1, AQP4, BRCA2, THY1, LRFN5, CPNE8, C5AR1, SIRPA, NLRP3, CASP1, CD9, CD14, AKT1S1, MINDY4, CD28, CD40, TLR2, TGFB2, TGFB3, HIF1A, P4HB, OGG1, NGF, NFKB1, NFE2L2, EGFR, ERBB2, MTR, MKLN1, MFGE8, MBP, FANCD2, LGALS1, LAMA3, LAG3, KARS1, IRF3, CXCL8, GFAP, GLS, IL1A, IFNAR1, IFN1@, PDIA3, HSPD1, HSPA5, GSN, DECR1, PDCD1, PDK1, RARB, CRYAB, ADAM17, HSPA13, SP1, SOD2, CSF1R, SNCG, CTSD, SNCB, SLC1A3, CYBB, RYR2, PVALB, PIK3CA, PTGS2, PSEN1, RELN, DAB1, PRKAB1, PRKAA2, PRKAA1, PPIA, PIN1, PIK3CG, PIK3CD, ABCA1, PIK3CB














