-
Tuberculous Meningitis
Wikipedia
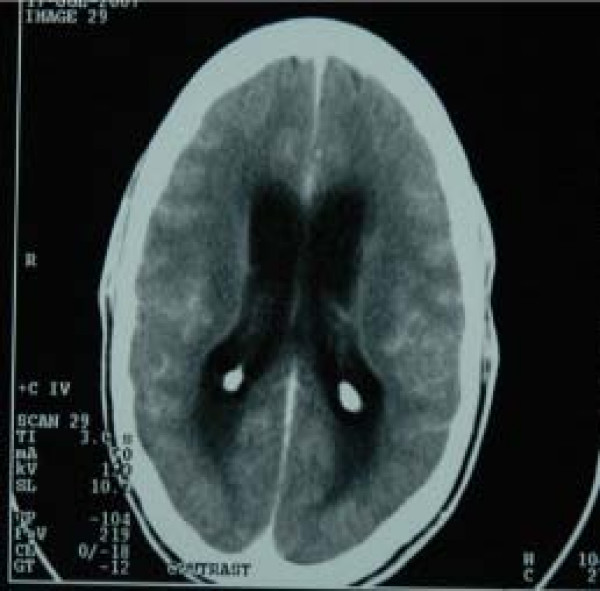
The two most common commercially available tests are the amplified mycobacterium tuberculosis direct test (MTD, Gen-Probe) and Amplicor. [14] In 2007, review concluded that for diagnosing tuberculous meningitis "Individually, the AMTD test appears to perform the best (sensitivity 74% and specificity 98%)", they found the pooled prevalence of TB meningitis to be 29%. [15] Treatment [ edit ] See also: Tuberculosis treatment The treatment of TB meningitis is isoniazid , rifampicin , pyrazinamide and ethambutol for two months, followed by isoniazid and rifampicin alone for a further ten months. [16] Steroids help reduce the risk of death in those without HIV . [17] Steroids can be used in the first six weeks of treatment, [18] A few people may require immunomodulatory agents such as thalidomide . [19] Hydrocephalus occurs as a complication in about a third of people with TB meningitis.BBS9, CSF2, LAMC2, ADA, LTA4H, MMP9, IFNG, RHOF, TLR2, RNF34, NCAPG2, MT1JP, TIRAP, IL10, CRP, TNF, IL1B, IL13, THEMIS, BECN1, ZNF410, VEGFA, CCN6, MIR29A, TTR, TRC-GCA24-1, VDR, GDF15, C1QTNF4, ARTN, SMUG1, AGO2, TIMP2, DLL1, CD274, RMC1, VSX1, TLR9, NAT2, SAA2, TIMP1, SPN, ADSL, AGRP, ALOX5, CAMP, CAT, CSF3, ESR1, GC, CFH, HPD, IL2, IL4, IL6, CXCL8, IL12B, IL17A, CXCL10, INS, MMP2, MUC5AC, NCAM1, SAA1, CCL1, CCL2, CCL3, SIGLEC14
-
Mitochondrial Complex Iii Deficiency, Nuclear Type 2
Omim
Morino et al. (2014) reported a 37-year-old Japanese woman, born of consanguineous parents, who presented clinically with adult-onset spinocerebellar ataxia. The patient first developed dysarthria at age 31 years.
-
Septic Arthritis
Mayo_clinic
Antibiotics are usually given through a vein in your arm at first. Later, you may be able to switch to oral antibiotics.
-
Dural Arteriovenous Fistulas
Mayo_clinic
What to expect from your doctor Your doctor is also likely to ask you a number of questions: When did you first begin experiencing symptoms (for example, hearing or vison problems, seizures, speech issues, palsies, or other symptoms)?CERNA3, PCYT1A, VEGFA, NDC1, TSPAN2, COIL, TGFBR2, PTEN, ACVRL1, CD38, SERPINE1, NFE2L2, MMP2, GABPA, F5, ENG, SERPINB2

-
High-Grade Prostatic Intraepithelial Neoplasia
Wikipedia
(Jan 2006). "Risk of prostate cancer on first re-biopsy within 1 year following a diagnosis of high grade prostatic intraepithelial neoplasia is related to the number of cores sampled".ERG, PTEN, LMNA, PCA3, GSTP1, DYNLL1, TMPRSS2, KLK3, TP53, ERBB2, PSCA, ESR2, MYC, DUSP1, SENP1, RICTOR, MMP9, BRCA2, BCL2, MAGI2, PTGS2, ANXA1, CD44, SPOP, UXT, KMT2D, CFLAR, TNFRSF1B, EZR, LONP1, TLR5, TIMP4, TFAP2A, ZEB1, STAT3, SPP1, SPINK1, SQSTM1, KHDRBS1, CYP7B1, GDF15, CREB3L4, MIB1, ACKR3, MMP26, PARD3, EAF2, TLR9, PTOV1, DCTN4, RMC1, PYCARD, HPGDS, NUP62, AMACR, SIRT1, TBC1D9, CBX3, RASSF1, SKP2, AGR2, RBX1, SLC2A5, ACTB, SFRP2, CTSH, FASN, F2RL2, ESR1, EPOR, EGFR, EDNRB, LPAR1, DSPP, DCN, CTNNB1, GDNF, CHEK1, CDKN3, CAV1, STS, AR, FAS, APRT, APOD, APC, FGF13, GLB1, RXRA, MUTYH, RBP1, PIK3CG, PIK3CD, ALDH1A1, PIK3CB, PIK3CA, ABCB1, NPY, NGF, MMP13, GSTA1, MKI67, MFAP1, MET, MCAM, IGFBP7, IGFBP3, FOXA1, HMOX1, GTF2H1, PIM1

-
Combined Small-Cell Lung Carcinoma
Wikipedia
TRT serves to increase the probability of total eradication of residual locoregional disease, while PCI aims to eliminate any micrometastases to the brain . [31] Surgery is not often considered as a treatment option in SCLC (including c-SCLC) due to the high probability of distant metastases at the time of diagnosis . [32] This paradigm was driven by early studies showing that the administration of systemic therapies resulted in improved survival as compared to patients undergoing surgical resection. [33] [34] [35] Recent studies, however, have suggested that surgery for highly selected, very early-stage c-SCLC patients may indeed improve outcomes. [36] Other experts recommend resection for residual masses of NSCLC components after complete local tumor response to chemotherapy and/or radiotherapy in c-SCLC. [37] Although other combinations of drugs have occasionally been shown to be noninferior at various endpoints and in some subgroups of patients, the combination of cisplatin or carboplatin plus etoposide or irinotecan are considered comparable first-line regimens for SCLC. [31] [38] For patients who do not respond to first line therapy, or who relapse after complete remission , topotecan is the only agent which has been definitively shown to offer increased survival over best supportive care (BSC), [31] [39] although in Japan amirubicin is considered effective as salvage therapy . [39] Importantly, c-SCLC is usually much more resistant to CT and RT than "pure" SCLC. [11] [17] [19] [40] [41] [42] While the mechanisms for this increased resistance of c-SCLC to conventional cytotoxic treatments highly active in "pure" SCLC remain mostly unknown, recent studies suggest that the earlier in its biological history that a c-SCLC is treated, the more likely it is to resemble "pure" SCLC in its response to CT and RT. [15] [16] [17] [18] Targeted agents [ edit ] In recent years, several new types of "molecularly targeted" agents have been developed and used to treat lung cancer. ... Some studies suggest it may, when combined with other agents, improve some measures of survival in SCLC patients [69] [70] and in some non-squamous cell variants of NSCLC. [7] [69] [57] Pemetrexed has been shown to improve survival in non-squamous cell NSCLC, and is the first drug to reveal differential survival benefit in large cell lung carcinoma. [7] [71] C-SCLC appear to express female hormone (i.e. estrogen and/or progesterone) receptors in a high (50–67%) proportion of cases, similar to breast carcinomas. [72] However, it is at present unknown whether blockade of these receptors affects the growth of c-SCLC. [ citation needed ] Prognosis [ edit ] Current consensus is that the long-term prognosis of c-SCLC patients is determined by the SCLC component of their tumor, given that "pure" SCLC seems to have the worst long-term prognosis of all forms of lung cancer. [8] Although data on c-SCLC is very sparse, [20] some studies suggest that survival rates in c-SCLC may be even worse than that of pure SCLC, [73] [74] likely due to the lower rate of complete response to chemoradiation in c-SCLC, although not all studies have shown a significant difference in survival. [75] Untreated "pure" SCLC patients have a median survival time of between 4 weeks and 4 months, depending on stage and performance status at the time of diagnosis. [31] [35] Given proper multimodality treatment, SCLC patients with limited disease have median survival rates of between 16 and 24 months, and about 20% will be cured. [31] [35] [76] [77] In patients with extensive disease SCLC, although 60% to 70% will have good-to-complete responses to treatment, very few will be cured, with a median survival of only 6 to 10 months. [31] [77] Some evidence suggests that c-SCLC patients who continue to smoke may have much worse outcomes after treatment than those who quit. [78] Incidence [ edit ] Reliable comprehensive incidence statistics for c-SCLC are unavailable. ... External links [ edit ] Classification D ICD - 10 : C33 - C34 ICD - 9-CM : 162 ICD-O : 8045/3 MeSH : D018288 DiseasesDB : 7616 External resources MedlinePlus : 007194 Lung Cancer Home Page . The National Cancer Institute site containing further reading and resources about lung cancer. [1] .

-
2016 Munich Shooting
Wikipedia
At about 5:50pm, he went to the toilets on the first floor and took a handgun from his backpack. ... At 8:26pm he went outside and was confronted by police officers, whereupon he shot himself in the head. [9] [10] [11] Early reports and videos [ edit ] Map of shooting: (1) McDonald's, where the shooting started (2) Olympia shopping mall An early witness, identified only by her first name Lauretta, in talking to CNN correspondent Doug McConnell on the phone claimed that the gunman had shouted " Allahu Akbar !" ... A state of emergency was declared at the Rechts der Isar Hospital , where one of the injured victims died. [15] Investigation [ edit ] Munich police chief Hubertus Andrä said that the shooting appeared to be a "classic shooting rampage" and not terrorism. [11] Police said that the gunman was obsessed with mass shootings and that written material on such attacks was found in his room. [18] Prosecutor Steinkraus Koch said that the gunman had a book about school shootings called Why Kids Kill: Inside the Minds of School Shooters by Peter Langman. [11] No references to religion were found in documents in his home. [12] Andrä said that there was an "obvious" link between the shooting and the fifth anniversary of the 2011 Norway attacks committed by Anders Behring Breivik . [12] [18] [47] However, a police search of the shooter's residence did not find the manifesto written and distributed by Breivik. [45] According to Abendzeitung , the shooter's own manifesto was found on his computer's hard disk. [48] Police investigator Robert Heimberger said that the shooter appeared to have hacked a girl's Facebook account in an attempt to lure people to McDonald's with an offer of free food. [49] Authorities said that the gunman had been planning the shooting for a year and probably purchased his gun illegally on the darknet . [45] [50] It was said to be a "reactivated" Glock 17 9mm semi-automatic pistol that previously had been used as a theatre prop. [50] [51] [52] German police believe that the gun may have originated in Slovakia, and said that its serial number had been removed. [50] On 25 July 2016, Munich police announced the arrest of a 16-year-old Afghan friend of the perpetrator who was being investigated on suspicion of failing to report the gunman's plans. [45] [53] Nearly two years after the shooting, police opened an investigation into Sonboly's contact with William Atchison, perpetrator of the 2017 Aztec High School shooting , [54] [55] and with a boy in Gerlingen who planned a school shooting there. [56] Shortly after the Munich shooting, Atchison wrote an epitaph to Sonboly on Encyclopedia Dramatica , [57] calling him a "true Aryan" and "true German". [56] [58] Perpetrator [ edit ] David Sonboly Born Ali Sonboly [5] 20 April 1998 [59] Munich , Germany Died 22 July 2016 (aged 18) Moosach district , Munich, Germany Cause of death Self-inflicted gunshot wound Nationality Iranian–German Other names علی سنبلی [60] Occupation Newspaper delivery boy, student David Sonboly (born Ali Sonboly ; [5] 20 April 1998 – 22 July 2016) was an 18-year-old Iranian-German with dual nationality. [11] [61] The Munich Police Department said Sonboly was born and raised in Munich and had no criminal record. [28] [62] He lived in an apartment in the neighbourhood of Maxvorstadt with his parents and younger brother. [63] [64] [65] [66] He grew up in a secular household, according to his neighbours. [67] He had a part-time job distributing a local free newspaper. [68] Neighbours described him as a "polite boy". [67] [69] German Interior Minister Thomas de Maizière said that he was the son of Shiite Muslims from Iran who came to Germany as asylum seekers in the 1990s. [12] [70] Sonboly's parents told police that their son had possibly converted to Christianity, but that he was not religious. [71] [72] In May 2016, Sonboly had his first name changed in all official documents from Ali to David . [5] Possible motives [ edit ] The report by the Bavarian State Office of Criminal Investigation and public prosecutor's office in March 2017 concluded that the shooting was not political, [73] saying that Sonboly's main motive was "revenge" for bullying, and that his mental illness and obsession with other shooting rampages were also a factor. [9] The Federal Office for the Protection of the Constitution , Germany's security agency, also believed he was a "psychologically ill avenger" rather than a terrorist. [74] Sonboly had undergone psychiatric treatment [9] for depression, [18] anxiety and post-traumatic stress disorder . [73] In 2015, he had been treated for two months as an inpatient in a mental care facility. [45] He was largely isolated from his peers and suffered years of bullying by classmates, which included physical abuse. [9] A former classmate recalled, "We always mobbed [ sic ] him in school, and he always told us that he would kill us". [75] He developed a hatred for those of a similar age and background as those who bullied him, [9] mainly Turks and Albanians.

-
High-Pressure Nervous Syndrome
Wikipedia
The effects experienced, and the severity of those effects, depend on the rate of descent, the depth and percentage of helium. [1] "Helium tremors" were first widely described in 1965 by Royal Navy physiologist Peter B. ... However, these reports were not available in the West until 1967. [3] The term high-pressure nervous syndrome was first used by Brauer in 1968 to describe the combined symptoms of tremor, electroencephalography (EEG) changes, and somnolence that appeared during a 1,189-foot (362 m) chamber dive in Marseille . [4] Contents 1 Symptoms 2 Causes 3 Prevention 4 In popular culture 5 See also 6 References 7 External links Symptoms [ edit ] Symptoms of HPNS include tremors , myoclonic jerking , somnolence , EEG changes, [5] visual disturbance, nausea , dizziness , and decreased mental performance. [1] [2] Causes [ edit ] HPNS has two components, one resulting from the speed of compression and the other from the absolute pressure. ... Vandenberg HMS Ghurka Glen Strathallan SAS Good Hope Gothenburg Herzogin Cecilie Hilma Hooker Hispania HMS Hood HMAS Hobart Igara James Eagan Layne Captain Keith Tibbetts King Cruiser SMS Kronprinz Kyarra HMS Laforey USAT Liberty Louis Sheid USS LST-507 SMS Markgraf Mikhail Lermontov HMS M2 Maine Maloja HMS Maori Marguerite SS Mauna Loa USAT Meigs Mendi USCGC Mohawk Mohegan RMS Moldavia HMS Montagu MV RMS Mulheim Nagato Oceana USS Oriskany Oslofjord P29 P31 Pedernales Persier HMAS Perth SAS Pietermaritzburg Piłsudski Pool Fisher HMS Port Napier Preußen President Coolidge PS Queen Victoria Radaas Rainbow Warrior RMS Rhone Rondo Rosehill Rotorua Royal Adelaide Royal Charter Rozi HMS Safari Salem Express USS Saratoga USS Scuffle HMS Scylla HMS Sidon USS Spiegel Grove Stanegarth Stanwood Stella HMAS Swan USS Tarpon Thesis Thistlegorm Toa Maru Torrey Canyon SAS Transvaal U-40 U-352 U-1195 Um El Faroud Varvassi Walter L M Russ Washingtonian (1913) HMNZS Wellington USS Yancey Yongala Zenobia Zealandia Zingara Cave diving sites Blauhöhle Chinhoyi Caves Devil's Throat at Punta Sur Engelbrecht Cave Fossil Cave Jordbrugrotta Piccaninnie Ponds Pluragrotta Pollatoomary Sistema Ox Bel Ha Sistema Sac Actun Sistema Dos Ojos Sistema Nohoch Nah Chich Freshwater dives Dutch Springs Ewens Ponds Little Blue Lake Training sites Capernwray Dive Centre Deepspot National Diving and Activity Centre Stoney Cove Open ocean diving Blue-water diving Black-water diving Diving safety Human factors in diving equipment design Human factors in diving safety Life-support system Safety-critical system Scuba diving fatalities Diving hazards List of diving hazards and precautions Environmental Current Delta-P Entanglement hazard Overhead Silt out Wave action Equipment Freeflow Use of breathing equipment in an underwater environment Failure of diving equipment other than breathing apparatus Single point of failure Physiological Cold shock response Decompression Nitrogen narcosis Oxygen toxicity Seasickness Uncontrolled decompression Diver behaviour and competence Lack of competence Overconfidence effect Panic Task loading Trait anxiety Willful violation Consequences Barotrauma Decompression sickness Drowning Hypothermia Hypoxia Hypercapnia Hyperthermia Diving procedures Ascending and descending Emergency ascent Boat diving Canoe and kayak diving Buddy diving buddy check Decompression Decompression practice Pyle stop Ratio decompression Dive briefing Dive log Dive planning Scuba gas planning Diver communications Diving hand signals Diving line signals Diver voice communications Diver rescue Diver training Doing It Right Drift diving Gas blending for scuba diving Night diving Solo diving Water safety Risk management Checklist Hazard identification and risk assessment Hazard analysis Job safety analysis Risk assessment Risk control Hierarchy of hazard controls Incident pit Lockout–tagout Permit To Work Redundancy Safety data sheet Situation awareness Diving team Bellman Chamber operator Diver medical technician Diver's attendant Diving supervisor Diving systems technician Gas man Life support technician Stand-by diver Equipment safety Breathing gas quality Testing and inspection of diving cylinders Hydrostatic test Sustained load cracking Diving regulator Breathing performance of regulators Occupational safety and health Approaches to safety Job safety analysis Risk assessment Toolbox talk Housekeeping Association of Diving Contractors International Code of practice Contingency plan Diving regulations Emergency procedure Emergency response plan Evacuation plan Hazardous Materials Identification System Hierarchy of hazard controls Administrative controls Engineering controls Hazard elimination Hazard substitution Personal protective equipment International Marine Contractors Association Occupational hazard Biological hazard Chemical hazard Physical hazard Psychosocial hazard Occupational hygiene Exposure assessment Occupational exposure limit Workplace health surveillance Safety culture Code of practice Diving safety officer Diving superintendent Health and safety representative Operations manual Safety meeting Standard operating procedure Diving medicine Diving disorders List of signs and symptoms of diving disorders Cramp Motion sickness Surfer's ear Pressure related Alternobaric vertigo Barostriction Barotrauma Air embolism Aerosinusitis Barodontalgia Dental barotrauma Pulmonary barotrauma Compression arthralgia Decompression illness Dysbarism Oxygen Freediving blackout Hyperoxia Hypoxia Oxygen toxicity Inert gases Avascular necrosis Decompression sickness Isobaric counterdiffusion Taravana Dysbaric osteonecrosis High-pressure nervous syndrome Hydrogen narcosis Nitrogen narcosis Carbon dioxide Hypercapnia Hypocapnia Breathing gas contaminants Carbon monoxide poisoning Immersion related Asphyxia Drowning Hypothermia Immersion diuresis Instinctive drowning response Laryngospasm Salt water aspiration syndrome Swimming-induced pulmonary edema Treatment Demand valve oxygen therapy First aid Hyperbaric medicine Hyperbaric treatment schedules In-water recompression Oxygen therapy Therapeutic recompression Personnel Diving Medical Examiner Diving Medical Practitioner Diving Medical Technician Hyperbaric nursing Screening Atrial septal defect Effects of drugs on fitness to dive Fitness to dive Psychological fitness to dive Research Researchers in diving physiology and medicine Arthur J. ... Hernández John Herrington Paul Hill Akihiko Hoshide Mark Hulsbeck Emma Hwang Norishige Kanai Les Kaufman Scott Kelly Karen Kohanowich Timothy Kopra Dominic Landucci Jon Lindbergh Kjell N.
-
Periapical Cyst
Wikipedia
F. nucleatum P. gingivalis P. intermedia T. forsythia T. denticola Pathologic entities Calculus Edentulism Fremitus Furcation defect Gingival enlargement Gingival pocket Gingivitis Horizontal bony defect Linear gingival erythema Occlusal trauma Periodontal pocket Periodontal disease Periodontitis Plaque Recession Vertical bony defect v t e Cystic diseases Respiratory system Langerhans cell histiocytosis Lymphangioleiomyomatosis Cystic bronchiectasis Skin stratified squamous: follicular infundibulum Epidermoid cyst and Proliferating epidermoid cyst Milia Eruptive vellus hair cyst outer root sheath Trichilemmal cyst and Pilar cyst and Proliferating trichilemmal cyst and Malignant trichilemmal cyst sebaceous duct Steatocystoma multiplex and Steatocystoma simplex Keratocyst nonstratified squamous: Cutaneous ciliated cyst Hidrocystoma no epithelium: Pseudocyst of the auricle Mucocele other and ungrouped: Cutaneous columnar cyst Keratin implantation cyst Verrucous cyst Adenoid cystic carcinoma Breast cyst Human musculoskeletal system Cystic hygroma Human digestive system oral cavity: Cysts of the jaws Odontogenic cyst Periapical cyst Dentigerous cyst Odontogenic keratocyst Nasopalatine duct cyst liver: Polycystic liver disease Congenital hepatic fibrosis Peliosis hepatis bile duct: Biliary hamartomas Caroli disease Choledochal cysts Bile duct hamartoma Nervous system Cystic leukoencephalopathy Genitourinary system Polycystic kidney disease Autosomal dominant polycystic kidney Autosomal recessive polycystic kidney Medullary cystic kidney disease Nephronophthisis Congenital cystic dysplasia Other conditions Hydatid cyst Von Hippel–Lindau disease Tuberous sclerosisTNF, TGFB1, MMP9, TP53, FN1, IL6, TIMP1, CXCL8, IFNG, HSPB2, HSPB1, HSPB3, BCL2, PTGS2, MMP1, CD68, MMP2, PTCH1, IL1B, SPP1, SMO, TIMP2, VEGFA, VDR, NME1, TP63, TNFRSF11A, CD83, CD163, PDPN, B3GAT1, HSPA14, IL17D, MYDGF, IL27, LGALS7B, TNFRSF11B, MME, COX2, HSPD1, CASP3, CD8A, CD14, CDH1, EDA, FGF2, FHIT, GLI1, HIF1A, HSPA4, HSPG2, MMP13, ICAM1, IL1A, IL10, IL17A, KRT13, LGALS1, LGALS3, LGALS7, MDM2, BTF3P11, MTCO2P12

-
Comedo
Wikipedia
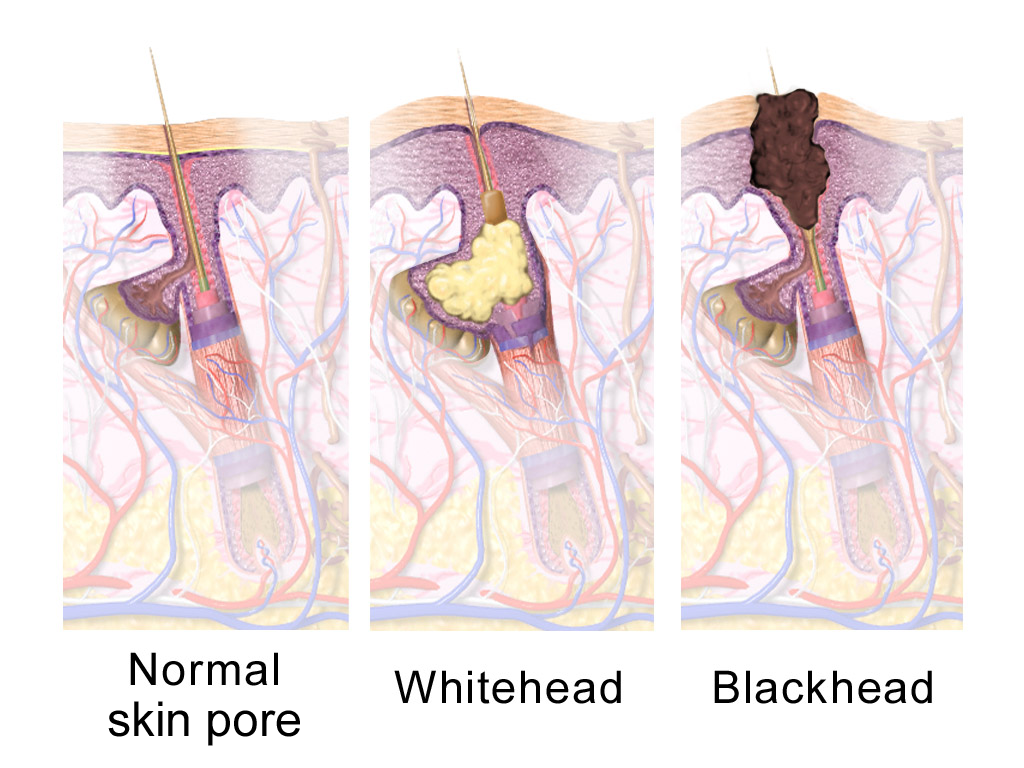
Rare conditions [ edit ] Favre–Racouchot syndrome occurs in sun-damaged skin and includes open and closed comedones. [18] Nevus comedonicus or comedo nevus is a benign hamartoma (birthmark) of the pilosebaceous unit around the oil-producing gland in the skin. [19] It has widened open hair follicles with dark keratin plugs that resemble comedones, but they are not actually comedones. [19] [20] Dowling-Degos disease is a genetic pigment disorder that includes comedo-like lesions and scars. [21] [22] Familial dyskeratotic comedones is a rare autosomal dominant genetic condition, with keratotic (tough) papules and comedo-like lesions . [23] [24] References [ edit ] ^ a b "Comedo" .LIPH, NEK9, LRP1, LPAR6, ERBB2, TP53, ESR1, PGR, S100A7, HSPB3, SET, UVRAG, VWF, TP63, DYNLL1, P4HA2, PARP1, THOC1, TXNIP, HPSE, CKAP4, RASSF1, BRMS1, CD274, PSENEN, INTS2, LOC102723407, S100B, LGMN, S100A1, RPE65, BCL2, BRCA1, CD79A, CISH, COL11A2, CTSV, CYC1, DEFB1, EGF, EGFR, ERBB3, FGF3, HSPB1, HSPB2, IL1B, KRT5, KRT10, LGALS3, NME1, OTC, CCND1, LOC102724971
-
Hay Fever
Mayo_clinic
Risk factors The following can increase your risk of developing hay fever: Having other allergies or asthma Having a condition called atopic dermatitis or eczema, which makes your skin irritated and itchy Having a blood relative, such as a parent or sibling, with allergies or asthma Living or working in an environment that constantly exposes you to allergens — such as animal dander or dust mites Being exposed to smoke and strong odors that irritate the lining of the nose Having a mother who smoked during your first year of life Complications Problems that may go along with hay fever include: Reduced quality of life. ... For many people, nasal sprays are the most effective hay fever medications, and they're often the first type of medication recommended.CST1, IL2, TNS1, SMAD3, IL1RL1, TLR1, CACNA1A, XKR6, GSDMA, CLEC16A, IL18R1, IKZF3, VAV3, IL13, HRH1, IL5, IL33, IL10, IL6, IFNG, JUN, CCL11, FLG, NR1I2, IL4, EPX, IL17RB, ADAM33, TLR4, IL4R, SOCS3, HACD1, KLF4, CD163, MZF1, YWHAZ, VEGFA, SCGB1A1, TNF, ABCA1, CLOCK, PCLAF, MIR17, PLB1, IFTAP, GLCCI1, CPEB4, IL25, CYSLTR2, MYDGF, SDAD1, SLC52A1, KRT20, FOXP3, DEXI, GPR162, TES, IL17RA, BRD4, PTGDR2, CYSLTR1, SORBS1, TRBV20OR9-2, CAP1, SERPINB6, CXCL11, GYPB, GSTP1, GSTM1, NR3C1, XCR1, LRRC32, FLNA, F2RL1, EGFR, EDN1, DUSP1, SLC26A3, SARDH, CCN2, CTAA1, CSF2RB, CREB1, CCR3, CEBPD, CD69, MS4A1, ADH1B, GYPA, GYPE, CCL4, HDC, SRL, PRTN3, PPIA, PLA2G1B, ABO, ENPP3, MUC5AC, MMP9, CXCL9, SMAD7, SMAD6, LYZ, LNPEP, CXCL10, IL18, IL2RA, HLA-G, HLA-DRB4, HLA-C, HLA-B, HLA-A, CCR2
-
Aortic Aneurysm
Wikipedia
Unfortunately, however, rupture may be the first hint of AAA. Once an aneurysm has ruptured, it presents with classic symptoms of abdominal pain which is severe, constant, and radiating to the back. ... The risk of the repair procedure is two-fold. First, there is consideration of the risk of problems occurring during and immediately after the procedure itself ("peri-procedural" complications).EFEMP2, TGFBR2, AGT, MMP9, LOX, SMAD3, SKI, SERPINE1, KLF15, ATP7A, FBN1, ELN, ACTA2, AOC3, MYH11, FBLN5, COX2, SMAD6, RIN2, ND6, ND5, ND4, ND1, COX3, COX1, BCR, TRNH, APOE, ERMARD, NOD2, IFIH1, RNASEH2B, RNASEH2C, HGD, TRNF, TRNQ, TRNL1, TMTC3, TGFBR1, RNASEH2A, ARFGEF2, ADAR, TREX1, TAB2, ALDH18A1, NEDD4L, PTEN, MAPK1, SAMHD1, SLC25A24, MYLK, MYH3, TRNW, TRNS2, TRNS1, C12orf57, ARF1, MAP1B, FLNB, FBN2, CHRNG, CRKL, COL1A1, FLNA, MMP2, ACE, NOTCH1, SPP1, ACTB, COL3A1, ALOX5, IL10, HIF1A-AS1, IL6, TLR4, F10, HIF1A, TGFB2, TGFB1, AGTR1, MMP3, THBS1, CAT, MIR143, ANGPT2, EGF, MIR145, HBEGF, CDKN2B, STAT3, CTSK, CD38, REN, MIR29B1, MIR29B2, CCL4, TP53COR1, TSHZ1, GPT, MIR126, TNC, VEGFA, KLF4, MSC, ATG5, LGALS3, FN1, SMAD2, MIR483, NTN1, MIR574, TRIP13, RNASE13, MBD2, ADIPOQ, MBD4, PDPN, PTENP1, AIM2, ADAMTS7, CCL4L2, ADAMTS5, RGS6, RBM8A, LYVE1, HDAC5, CERNA3, PTENP1-AS, KHDRBS1, LOC100506472, CDKN2B-AS1, MIR30C2, ANGPTL2, BTBD8, SMUG1, NUP62, CCL4L1, RETN, TBX20, RTN4, TSPYL2, RNU6-2, FSD1, COQ8B, PDGFD, SLC2A10, MAP1LC3B, FSD1L, PPP1R42, SPATC1L, SPZ1, ARHGAP18, OSR1, PRSS55, AAT1, SQSTM1, CHDH, KRTDAP, MIR21, ARIH1, PRPF31, MIR222HG, PYCARD, UHRF1, IS1, MIR221, MIR22, MIR195, MED18, MIR155, MIR148A, NOX4, SOST, DCTN4, SLC25A37, IL23A, MIR122, MIR29A, RASA1, ZIC3, EGR1, ESR1, EZH2, FCGRT, MTOR, GAA, GAPDH, GCG, GLI2, GTF2H1, HDAC1, HLA-DRB1, HP, HSPD1, IFNA1, IFNA13, IFNG, IL1B, IL1RN, IL2, IL4, IL6R, ERBB2, EDN1, CXCR1, DNMT3A, ACVRL1, AKT1, AQP1, AR, BICD1, BMP2, VPS51, CASP4, CD68, CDH5, CDKN2A, CGA, LTB4R, COMP, CRP, MAPK14, CST3, CTNNB1, CTSL, CTSS, DECR1, CXCL8, IL13, XIST, RBBP8, S100A9, S100A12, CCL2, CCL20, SLPI, ADAM17, TAGLN, TRBV20OR9-2, TGFB3, TIMP3, TNF, TP53, CRISP2, TSC2, TYMS, TYRP1, UCP2, UMOD, VIM, TRPV1, XBP1, RGS1, PTGS2, IL17A, MAPK8, KLK1, KRAS, LEP, LOXL1, SMAD4, MAS1, FOXO4, MMP1, MMP14, MMP17, MPO, MYH10, NFKB1, NOS3, NRAS, TNFRSF11B, PCYT1A, PECAM1, PLG, PPARG, CTSA, MTCO2P12

-
Acrophobia
Wikipedia
Some proponents of the alternative view of acrophobia warn that it may be ill-advised to encourage acrophobics to expose themselves to height without first resolving the vestibular issues. ... However, avoidance behaviour is reinforced through negative reinforcement . [5] [25] Wolpe developed a technique called systematic desensitization to help participants avoid "avoidance". [26] Research results have suggested that even with a decrease in therapeutic contact densensitization is still very effective. [27] However, other studies have shown that therapists play an essential role in acrophobia treatment. [28] Treatments like reinforced practice and self-efficacy treatments also emerged. [5] There have been a number of studies into using virtual reality therapy for acrophobia. [29] [30] Botella and colleagues [31] and Schneider [31] were the first to use VR in treatment. [5] Specifically, Schneider utilised inverted lenses in binoculars to "alter" the reality.

-
Dental Fear
Wikipedia
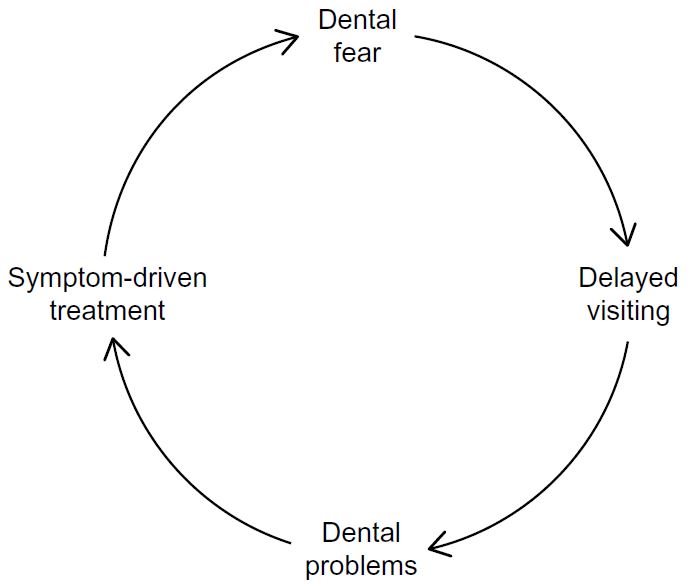
As, expected dental fear is associated with previous traumatic experiences, especially their first one. [1] It is believed to be the most commonly used pathway for patients to develop dental fear and anxiety. [6] Informative This indirect pathway relates to fear acquisition through gaining information and becoming bias to the dental environment from dental phobic elders, negative connotations advertised by media ( e.g . television, movies), and friends with personal negative experiences. [6] Vicarious The vicarious pathway suggests that fear is acquired through imagination of the feelings, experience or actions of another person. ... This scale has a ranking system and the second section with 26 questions has 1–4 options ranging from 'low' to 'don't know' which is used to assess dental concern. The first section with 1–4 questions has 5 Likert scale options which are worth 1–5 points with the possible amount of maximum points is 20.
-
Postpartum Blues
Wikipedia
Postpartum depression Postpartum depression and postpartum blues may be indistinguishable when symptoms first begin. However, symptoms of postpartum blues are less severe, resolve on their own, and last fewer than two weeks. ... "The pattern of mental change and body weight change in the first post-partum week". Journal of Psychosomatic Research . 24 (3–4): 165–71. doi : 10.1016/0022-3999(80)90038-0 .
-
Asbestos-Related Diseases
Wikipedia
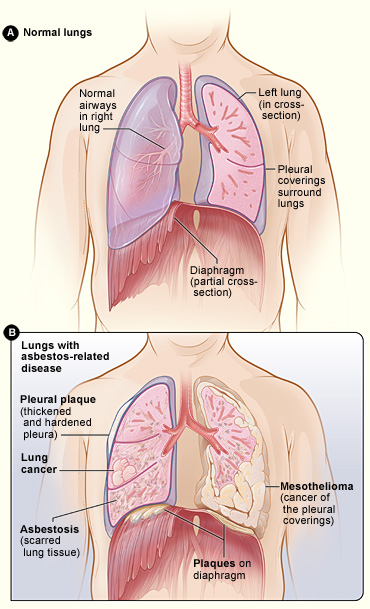
The prevalence among the general population exposed environmentally ranges from 0.53 to 8%. [4] Pleural plaques are discrete circumscribed areas of hyaline fibrosis (patches of thickening) of the parietal pleura and rarely the visceral pleura that develop 20 to 40 years after first exposure. Over time, usually more than 30 years, they often become partly calcified. ... Diffuse pleural thickening develops 20 to 40 years after first exposure. [11] All types of asbestos can cause diffuse pleural thickening and a dose-related relationship has been described. [6] It is thought that asbestos fibres that reach the pleura induce subpleural fibroblasts and mesothelial cells to produce scar tissue and collagen deposition, resulting in subpleural thickening. [6] Pleural plaques often coexist with DPT although the latter is rare compared with pleural plaques.
-
Radiophobia
Wikipedia
When atomic testing began in the early 1950s, these hazards were grossly exaggerated, producing a new psychological disorder which has been called "radiophobia" or "nuclear neurosis". [13] Castle Bravo and its influence on public perception [ edit ] March 1, 1954, the operation Castle Bravo testing of a then, first of its kind, experimental thermonuclear Shrimp device, overshot its predicted yield of 4–6 megatons and instead produced 15 megatons ; this resulted in an unanticipated amount of Bikini snow or visible particles of nuclear fallout being produced, fallout which caught the Japanese fishing boat the Daigo Fukuryū Maru or Lucky Dragon in its plume, even though it was fishing outside the initially predicted ~5 megaton fallout area which had been cordoned off for the Castle Bravo test. ... PMID 2284594 . ^ Alvin M. Weinberg (1 January 1994). The First Nuclear Era: The Life and Times of a Technological Fixer .

-
Spasticity
Wikipedia
Alternatively, rehabilitation robotics can be used to provide high volumes of passive or assisted movement, depending on the individual's requirements; [11] this form of therapy can be useful if therapists are at a premium, and has been found effective at reducing spasticity in patients suffering from stroke . [12] For muscles that lack any volitional control, such as after complete spinal cord injury , exercise may be assisted, and may require equipment, such as using a standing frame to sustain a standing position. [ citation needed ] A general treatment guideline can be followed that involves: The initial focus on first activating contraction of antagonist muscles to provide reciprocal inhibition and lengthen spastic muscles Reciprocal actions are attempted. Agonist contractions are performed first in small ranges progressing to larger arcs of movement Highly stressful activities be minimized early in training Functional skills are targeted for training Patients and family/caregivers should be educated about the importance of maintaining range of motion and doing daily exercises [13] Medical interventions may include such medications as baclofen , diazepam , dantrolene , or clonazepam .SPAST, ACTL6B, PQBP1, EIF2B5, CNR1, ADRA2A, MECP2, SACS, L1CAM, SOD1, ATXN3, ALS2, SLC2A1, ALDH3A2, OPA3, BSCL2, SPG7, CTNNB1, C19orf12, TIMM8A, SIGMAR1, CIT, DDX3X, TBP, FXN, AARS1, ATXN2, FA2H, RARS1, GRIK2, UCHL1, HLA-DRB1, ATP13A2, KCNA1, POLR3B, VPS13D, DARS2, ND1, SLC17A5, RAB18, PGAP1, ARX, CACNA1A, TSEN54, CAPN1, KIF1A, SLC6A5, SIK1, SLC39A14, RAB3GAP2, FRRS1L, NUP62, AMACR, PIGQ, PIGN, ATP6V0A2, KAT6B, MATR3, SUZ12, BAZ1B, MACF1, TARDBP, VAPB, SZT2, WASHC4, RAB11B, RPGRIP1L, DENND5A, PLCB1, MLC1, AIMP1, FBXO7, TXN2, CACNA1G, ABHD12, PYCR2, TBK1, DCPS, PCLO, HTRA2, TPK1, CYFIP2, SUCLA2, TBL2, SYNGAP1, ACAT1, SQSTM1, AUTS2, MAPK8IP3, CNTNAP2, SETBP1, EIF2B4, CHMP2B, NECAP1, EIF2B3, EIF2B2, PARS2, SAMHD1, NDUFAF3, RTTN, AP1S2, PMPCA, RPIA, TNIK, OPTN, ERLIN1, MTHFS, NPC2, RNASEH2A, PMPCB, TUBB4A, TUBB3, TECR, WARS2, GABBR2, GPHN, RAD50, UNC13A, GTF2IRD1, SCO2, ZNF592, PUM1, KMT2B, ARNT2, FIG4, TELO2, RUSC2, ZEB2, DNAJC6, AP4B1, KIF1C, ITM2B, KDM5B, FRMPD4, COPB2, RAB3GAP1, TRAK1, CNKSR2, NTNG1, PARK7, PEX16, PNKP, TREX1, CHP1, MAN1B1, ERLIN2, AP4S1, POLR3A, MED23, B4GAT1, CLP1, PNPLA8, AFG3L2, PPARGC1A, MED17, WDR4, UBQLN2, INPP5K, SLC45A1, TPRKB, TOE1, NACC1, TP53RK, MARS2, TIMM50, RFT1, TMEM67, GFM1, REPS1, SERAC1, WDR73, PPP1R15B, ATAD1, GPT2, NKX6-2, GFM2, FAR1, RNASEH2C, JAM3, TRAPPC9, MED25, ISCA1, TRIM8, CLPB, LMAN2L, NUBPL, SPG11, CTC1, EDC3, NUS1, LRRK2, ISCA2, SUMF1, NPHP3-ACAD11, OCLN, RNU4ATAC, SNORD118, ATXN8, SDHAF1, GTF2H5, CHCHD10, BOLA3, NHLRC1, KIF7, HCN1, NEXMIF, UNC80, MTFMT, SLC13A5, HEPACAM, C9orf72, SPATA5, TMTC3, C11orf65, CKAP2L, B3GALNT2, BEAN1, MPLKIP, NADK2, TBC1D20, METTL23, PANK2, STN1, DHDDS, RETREG1, VPS11, PEX26, OSGEP, POMGNT1, ACER3, ATAD3A, LINS1, NSUN2, CC2D1A, GDAP2, VPS13C, TRIT1, GTPBP2, TREM2, ZC4H2, ADAM22, CRADD, WWOX, UFM1, UFC1, HIKESHI, SPG21, RSRC1, PIGP, CRBN, RLIM, TRAPPC12, EXOSC3, GLT8D1, KLHL7, ZC3H14, SIL1, UBA5, TCTN2, FBXO31, SLC25A22, NARS2, ROGDI, TMEM231, MBOAT7, NDUFAF5, MRPS34, PINK1, BCL11B, ARV1, NSD1, FMN2, IRF2BPL, MCCC2, ZNF335, GUF1, KCNT1, TRMT5, CC2D2A, AARS2, SCYL1, SNX14, C12orf4, MFF, MCCC1, PEX11B, SYNJ1, GPAA1, GRIN2D, KCNB1, KCNA2, IREB2, NDST1, HPRT1, HNRNPA1, HNMT, HMGCL, HLA-DQB1, HTT, GTF2I, GTF2E2, GRIN2B, KRAS, GRIN1, GRIA3, GNAO1, GLRB, GLRA1, GLE1, GJA1, GFAP, GCDH, GBE1, GBA, GABRG2, KIF11, LIMK1, OPHN1, TRNW, NPC1, NOTCH3, NEUROD2, NEK1, NEFH, NDUFV2, NDUFS4, NDUFS2, NDUFB8, NDUFA6, NAGA, MYO5A, TRNV, LMNB1, TRNP, TRNL1, TRNK, TRNI, EED, ND6, ND5, ND4, ND3, ND2, ATP6, MAN2B1, GABRB2, FUS, FTL, BCS1L, CSF1R, CREBBP, COX15, COX10, COL4A2, COL4A1, CLTC, ENTPD1, CCNF, CAMK2A, CACNA1B, CFAP410, ATRX, FOXG1, ATP7A, ATP6V1E1, ATP6V1A, ATM, ASPA, ARSA, ARF1, ANXA11, ANK3, ANG, AMPD2, AGA, CTSD, CYP27A1, DAO, DARS1, FGFR1, FGF12, EZH2, ERCC6, ERCC5, ERCC4, ERCC3, ERCC2, ERBB4, EPRS1, EPHA4, EML1, ELN, EIF2B1, EEF1A2, ECHS1, DNMT1, DYNC1I2, DNM1, DLD, DHPS, DHCR24, DDB2, DCX, DCTN1, NTRK2, TRNF, ALDH18A1, SDHD, SCN8A, SCN3A, RNF113A, SCN2A, EPM2A, SCN1B, ATXN8OS, ATXN7, ATXN1, SARS1, TUSC3, CLIP1, KAT6A, NUP214, AP3B2, RFC2, RAB27A, GAN, TAF15, PEX5, PEX2, PEX19, PTH2R, SDHA, YWHAG, LAGE3, ST3GAL3, TYROBP, TTR, VCP, TPI1, TCF20, TAF2, EZR, SURF1, ABCC8, STXBP1, CDKL5, SPTBN2, SPR, SOX10, SON, SNCA, SMPD1, CLIP2, XPA, SLC6A8, SLC2A3, XPC, SLC1A2, KDM5C, UBTF, SLC25A12, PRPH, PRNP, PPT1, PEX13, PEX14, PPP3CA, DEGS1, PFN1, PON3, PON2, PON1, PIGA, CASK, PLA2G6, PODXL, PIGC, PMM2, PEX12, PEX10, HTRA1, PRKN, CHMP1A, PSAP, PRSS12, PEX3, CNTNAP1, PDCD1, PEX1, PEX6, IKBKG, PEX7, EXOSC9, OPN1MW2, SLC12A5, OPN1MW, OPN1MW3, WAS, ATL1, GBA2, PLP1, IGFALS, GJC2, LEP, DDHD2, SPNS1, GRIA1, REEP1, NARS1, ROM1, MS, PSEN1, PHGDH, SLC35A2, SFXN1, IS1, ACP5, ARG1, RNASET2, BDNF, NAXE, PPT2, NIPA1, AHSG, RCC1, AR, CANDF1, ALB, CRP, MED20, TBX4, TP63, OPRM1, TBL1XR1, TTN, LY6E, PDXP, PTHLH, IGF1, IL10, IFT122, KCNA5, KCNA6, KCNC3, KIF5A, MAS1, HSP90B2P, POMC, POLG, PKM, PRDX5, PART1, FOXP3, PSAT1, NEFL, PNP, GATAD2B, HLA-C, RAC2, SPG16, ABCB6, ATP6AP2, SLC16A2, SLC12A2, DDHD1, FGF14, SLC1A4, GAST, SGCG, GALNS, GARS1, PAEP, WDR45, PAGR1, GRIA2, GRIK3, EXOSC8, GRM2, GRM7, SIK1B
-
Peripartum Cardiomyopathy
Wikipedia
However, in view of reversible cardiomyopathy, sometimes Implantable cardioverter-defibrillator (ICD) or Cardiac resynchronization therapy (CRT) are not routinely used and reserved for severe LV dysfunction or high risk cases. [17] Prognosis [ edit ] The most recent studies indicate that with newer conventional heart failure treatment consisting of diuretics , ACE inhibitors and beta blockers , the survival rate is very high at 98% or better, and almost all PPCM patients improve with treatment. [15] [18] [19] In the United States, over 50% of PPCM patients experience complete recovery of heart function (EF 55% or greater). [5] [8] Almost all recovered patients are eventually able to discontinue medications with no resulting relapse and have normal life expectancy. [18] It is a misconception that hope for recovery depends upon improvement or recovery within the first six to 12 months of diagnosis. Many women continue to improve or recover even years after diagnosis with continued medicinal treatment. [4] [20] Once fully recovered, if there is no subsequent pregnancy, the possibility of relapse or recurrence of heart failure is minimal. [15] [19] Subsequent pregnancy should be avoided when left ventricular function has not recovered and the EF is lower than 55%. [2] [21] However, many women who have fully recovered from PPCM have gone on to have successful subsequent pregnancies. [8] A significant study reports that the risk for recurrence of heart failure in recovered PPCM patients as a result of subsequent pregnancy is approximately 21% or better. [21] The chance of relapse may be even smaller for those with normal contractile reserve as demonstrated by stress echocardiography. [22] [23] In any subsequent pregnancy, careful monitoring is necessary. ... Epidemiology [ edit ] It is estimated that the incidence of PPCM in the United States is between 1 in 1300 to 4000 live births. [2] [20] [24] While it can affect women of all races, it is more prevalent in some countries; for example, estimates suggest that PPCM occurs at rates of one in 1000 live births in South African Bantus, and as high as one in 300 in Haiti. [9] [20] Some studies assert that PPCM may be slightly more prevalent among older women who have had higher numbers of liveborn children and among women of older and younger extremes of childbearing age. [9] [24] However, a quarter to a third of PPCM patients are young women who have given birth for the first time. [3] [4] [9] [20] [25] [26] While the use of tocolytic agents or the development of preeclampsia (toxemia of pregnancy) and pregnancy-induced hypertension (PIH) may contribute to the worsening of heart failure, they do not cause PPCM; the majority of women have developed PPCM who neither received tocolytics nor had preeclampsia nor PIH. [20] [25] In short, PPCM can occur in any woman of any racial background, at any age during reproductive years, and in any pregnancy. [21] References [ edit ] ^ RESERVED, INSERM US14-- ALL RIGHTS.
-
Delusional Parasitosis
Wikipedia
The highest incidence occurs in people in their 60s, but there is also a higher occurrence in people in their 30s, associated with substance use. [1] It occurs most often in "socially isolated" women with an average age of 57. [4] Since the early 2000s, a strong internet presence has led to increasing self-diagnosis. [1] History [ edit ] Karl-Axel Ekbom , a Swedish neurologist, first described delusional parasitosis as "pre-senile delusion of infestation" in 1937. [1] The common name has changed many times since then. ... Other names that referenced "phobia" were rejected because anxiety disorder was not typical of the symptoms. [12] The eponymous Ekbom's disease was changed to "delusions of parasitosis" in 1946 in the English literature, when researchers J Wilson and H Miller described a series of cases, and to "delusional infestation" in 2009. [1] [13] The most common name since 2015 has been "delusional parasitosis". [2] Ekbom's original was translated to English in 2003; the authors hypothesized that James Harrington (1611–1677) may have been the "first recorded person to suffer from such delusions when he 'began to imagine that his sweat turned to flies, and sometimes to bees and other insects'. [14] Morgellons [ edit ] Main article: Morgellons Mary Leitao, the founder of the Morgellons Research Foundation, [15] coined the name Morgellons in 2002, reviving it from a letter written by a physician in the mid-1600s. [16] [17] Leitao and others involved in her foundation (who self-identified as having Morgellons) successfully lobbied members of the U.S.











