A number of different disorders may cause polyneuropathy, including diabetes and some types of Guillain–Barré syndrome . [4] [5] [6] Contents 1 Classification 2 Signs and symptoms 3 Causes 4 Pathophysiology 5 Diagnosis 5.1 Differential diagnosis 6 Treatment 7 See also 8 References 9 Further reading 10 External links Classification [ edit ] Polyneuropathies may be classified in different ways, such as by cause , [2] by presentation , [1] or by classes of polyneuropathy, in terms of which part of the nerve cell is affected mainly: the axon , the myelin sheath, or the cell body . [7] [8] Action potential propagation in myelinated neurons is faster than in unmyelinated neurons(left) Distal axonopathy , is the result of interrupted function of the peripheral nerves. [9] It is the most common response of neurons to metabolic or toxic disturbances, and may be caused by metabolic diseases such as diabetes , kidney failure , connective tissue disease , deficiency syndromes such as malnutrition and alcoholism , or the effects of toxins or drugs such as chemotherapy . ... People with distal axonopathies usually present with sensorimotor disturbances such as amyotrophic lateral sclerosis [10] Myelinopathy , is due to a loss of myelin or of the Schwann cells . [11] This demyelination slows down or completely blocks the conduction of action potentials through the axon of the nerve cell ( neurapraxia ). [12] The most common cause is acute inflammatory demyelinating polyneuropathy AIDP, the most common form of Guillain–Barré syndrome [13] (although other causes include chronic inflammatory demyelinating polyneuropathy ) [14] Neuronopathy is the result of issues in the peripheral nervous system (PNS) neurons. ... Although diseases often are suggested by the physical examination and history alone, tests that may be employed include: electrodiagnostic testing, serum protein electrophoresis , nerve conduction studies , urinalysis , serum creatine kinase (CK) and antibody testing (nerve biopsy is sometimes done). [1] [3] Other tests may be used, especially tests for specific disorders associated with polyneuropathies, quality measures have been developed to diagnose patients with distal symmetrical polyneuropathy (DSP). [17] Differential diagnosis [ edit ] In terms of the differential diagnosis for polyneuropathy one must look at the following: Vitamin deficiency [18] Diabetes mellitus [18] Toxins [18] Guillain–Barré syndrome [18] Lyme disease [18] Hepatitis C [18] Amyloidosis [18] Acromegaly [18] Kidney failure [19] Friedreich's Ataxia [20] Treatment [ edit ] Methylprednisolone In the treatment of polyneuropathies one must ascertain and manage the cause, among management activities are: weight decrease, use of a walking aid, and occupational therapist assistance. ... External links [ edit ] Classification D ICD - 10 : G60 - G64 ICD - 9-CM : 356.4 , 357.1 - 357.7 MeSH : D011115 External resources Patient UK : Polyneuropathy Scholia has a topic profile for Polyneuropathy . v t e Diseases relating to the peripheral nervous system Mononeuropathy Arm median nerve Carpal tunnel syndrome Ape hand deformity ulnar nerve Ulnar nerve entrapment Froment's sign Ulnar tunnel syndrome Ulnar claw radial nerve Radial neuropathy Wrist drop Cheiralgia paresthetica long thoracic nerve Winged scapula Backpack palsy Leg lateral cutaneous nerve of thigh Meralgia paraesthetica tibial nerve Tarsal tunnel syndrome plantar nerve Morton's neuroma superior gluteal nerve Trendelenburg's sign sciatic nerve Piriformis syndrome Cranial nerves See Template:Cranial nerve disease Polyneuropathy and Polyradiculoneuropathy HMSN Charcot–Marie–Tooth disease Dejerine–Sottas disease Refsum's disease Hereditary spastic paraplegia Hereditary neuropathy with liability to pressure palsy Familial amyloid neuropathy Autoimmune and demyelinating disease Guillain–Barré syndrome Chronic inflammatory demyelinating polyneuropathy Radiculopathy and plexopathy Brachial plexus injury Thoracic outlet syndrome Phantom limb Other Alcoholic polyneuropathy Other General Complex regional pain syndrome Mononeuritis multiplex Peripheral neuropathy Neuralgia Nerve compression syndrome v t e Medicine Specialties and subspecialties Surgery Cardiac surgery Cardiothoracic surgery Colorectal surgery Eye surgery General surgery Neurosurgery Oral and maxillofacial surgery Orthopedic surgery Hand surgery Otolaryngology ENT Pediatric surgery Plastic surgery Reproductive surgery Surgical oncology Transplant surgery Trauma surgery Urology Andrology Vascular surgery Internal medicine Allergy / Immunology Angiology Cardiology Endocrinology Gastroenterology Hepatology Geriatrics Hematology Hospital medicine Infectious disease Nephrology Oncology Pulmonology Rheumatology Obstetrics and gynaecology Gynaecology Gynecologic oncology Maternal–fetal medicine Obstetrics Reproductive endocrinology and infertility Urogynecology Diagnostic Radiology Interventional radiology Nuclear medicine Pathology Anatomical Clinical pathology Clinical chemistry Cytopathology Medical microbiology Transfusion medicine Other Addiction medicine Adolescent medicine Anesthesiology Dermatology Disaster medicine Diving medicine Emergency medicine Mass gathering medicine Family medicine General practice Hospital medicine Intensive care medicine Medical genetics Narcology Neurology Clinical neurophysiology Occupational medicine Ophthalmology Oral medicine Pain management Palliative care Pediatrics Neonatology Physical medicine and rehabilitation PM&R Preventive medicine Psychiatry Addiction psychiatry Radiation oncology Reproductive medicine Sexual medicine Sleep medicine Sports medicine Transplantation medicine Tropical medicine Travel medicine Venereology Medical education Medical school Bachelor of Medicine, Bachelor of Surgery Bachelor of Medical Sciences Master of Medicine Master of Surgery Doctor of Medicine Doctor of Osteopathic Medicine MD–PhD Related topics Alternative medicine Allied health Dentistry Podiatry Pharmacy Physiotherapy Molecular oncology Nanomedicine Personalized medicine Public health Rural health Therapy Traditional medicine Veterinary medicine Physician Chief physician History of medicine Book Category Commons Wikiproject Portal Outline
A number sign (#) is used with this entry because thiamine metabolism dysfunction syndrome-2 (THMD2), also known as biotin-responsive basal ganglia disease (BBGD) or thiamine-responsive encephalopathy, is caused by homozygous or compound heterozygous mutation in the SLC19A3 gene (606152), which encodes a thiamine transporter, on chromosome 2q36. Description Thiamine metabolism dysfunction syndrome-2 is an autosomal recessive metabolic disorder characterized by episodic encephalopathy, often triggered by febrile illness, presenting as confusion, seizures, external ophthalmoplegia, dysphagia, and sometimes coma and death. ... Brain imaging showed abnormal signal intensities in the basal ganglia, thalamus, brainstem, and cerebellum, consistent with a clinical diagnosis of Leigh syndrome (256000). All 5 patients died of respiratory insufficiency about 1 month after birth. ... Clinical Management Haack et al. (2014) reported 2 brothers, born of consanguineous Turkish parents, with genetically confirmed THMD2 presenting as infantile-onset encephalopathy with features of Leigh syndrome on brain imaging. The first infant died at age 2 months. ... Brain imaging shows abnormal intracranial lesions consistent with Leigh syndrome in humans. Vernau et al. (2013) determined that AHE is caused by a homozygous truncating mutation (c.624insTTGC, c.625C-A) in the Slc19a3.1 gene.
Simple partial or generalized seizures are easily controlled with antiepileptic drugs. An early-infantile Leigh-like syndrome / atypical infantile spasms presentation occurs in the first three months of life with poor feeding, vomiting, acute encephalopathy, and severe lactic acidosis. ... Treatment initiated later in the disease course or lack of treatment may result in death or chronic neurologic sequelae including dystonia, quadriparesis, epilepsy, or mild intellectual disability. The early-infantile Leigh-like syndrome / atypical infantile spasms presentation is characterized by the occurrence in the first three months of life of poor feeding, vomiting, acute encephalopathy, and severe lactic acidosis. ... Mitochondrial disorders (incl Leigh syndrome) 4 AR AD Mat HTT Juvenile Huntington disease AD ATP7B Wilson disease AR TH Tyrosine hydroxylase deficient dopa-responsive dystonia (See Tyrosine Hydroxylase Deficiency.) ... See also Nuclear Gene-Encoded Leigh Syndrome Overview. 5. Byrne et al [2019] Note: Dopa-responsive dystonia and Wilson disease are important to consider because they are treatable. ... See Thiamine-responsive dysfunction syndrome: OMIM Phenotypic Series to view genes associated with this phenotype in OMIM.
A rare genetic neurological disorder characterized by subacute encephalopathy with confusion, seizures, and movement disorder, often following a history of febrile illness. Imaging may reveal bilateral lesions in the basal ganglia. The disease usually becomes symptomatic in childhood and is life-threatening if left untreated, but symptoms can be reversed and progression prevented by treatment with high doses of biotin and thiamine.
Biotin-thiamine-responsive basal ganglia disease is a rare condition that affects the brain and other parts of the nervous system. The severity of the condition and the associated signs and symptoms vary from person to person, even within the same family. Without early diagnosis and treatment, most affected people develop features of the condition between ages 3 and 10 years. Signs and symptoms may include recurrent episodes of confusion, seizures, ataxia (problems coordinating movements), dystonia, facial palsy (weakness of the facial muscles), external ophthalmoplegia (paralysis of the muscles surrounding the eye), and dysphagia. Eventually, these episodes can lead to coma or even death. Biotin-thiamine-responsive basal ganglia disease is caused by changes (mutations) in the SLC19A3 gene and is inherited in an autosomal recessive manner.
Biotin-thiamine-responsive basal ganglia disease is a disorder that affects the nervous system, including a group of structures in the brain called the basal ganglia, which help control movement. As its name suggests, the condition may improve if the vitamins biotin and thiamine are given as treatment. Without early and lifelong vitamin treatment, people with biotin-thiamine-responsive basal ganglia disease experience a variety of neurological problems that gradually get worse. The occurrence of specific neurological problems and their severity vary even among affected individuals within the same family. The signs and symptoms of biotin-thiamine-responsive basal ganglia disease usually begin between the ages of 3 and 10, but the disorder can appear at any age.
Thiamine-responsive encephalopathy is a Wernicke-like encephalopathy (see this term) characterized by seizures responsive to high doses of thiamine. Epidemiology Two cases have been described so far. Clinical description Clinical features include epilepsy, nystagmus, ophthalmoplegia and ataxia. Etiology The disease results from mutations in the SLC19A3 gene, encoding a thiamine transporter. Genetic counseling Transmission is autosomal recessive.
Uncommonly, Niemann-Pick disease Type C (NPC) and Gaucher disease type 2 can present with hydrops fetalis. Turner syndrome Tumors , [7] the most common type of fetal tumor being teratoma , particularly a sacrococcygeal teratoma . Twin-twin transfusion syndrome (TTTS) in pregnancies in which twins share a single placenta (hydrops affects the recipient twin) Twin anemia-polycythemia sequence (TAPS) Twin reversed arterial perfusion sequence (TRAPS) Maternal hyperthyroidism Fetal cardiac defects and skeletal defects Noonan syndrome Mirror syndrome , in which fetal and placental hydrops develops in association with maternal preeclampsia , edema and hypertension Down syndrome Diagnosis [ edit ] Hydrops fetalis can be diagnosed and monitored by ultrasound scans. ... This procedure can be performed prior to delivery if gestational age is advanced. [12] Hydrops Fetalis resulting from fetal CPAM can be treated using either a fetal needle drainage of effusion or placement of thoracoamniotic shunt or a maternal administration of corticosteroids, betamethasone 12.5 mg IM q24 h × 2 doses or dexamethasone 6.25 mg IM q12 h × 4 doses. [13] Therapy for hydrops fetalis derived from TTTS or TAPS requires laser ablation of placental anastomoses or selective termination. [14] Therapy for hydrops fetalis derived from TRAPS requires percutaneous radio frequency ablation. [15] See also [ edit ] Mirror syndrome References [ edit ] ^ "Hydrops Fetalis: eMedicine Pediatrics: Cardiac Disease and Critical Care Medicine" . ... (January 2013). "Twin-twin transfusion syndrome". American Journal of Obstetrics and Gynecology . 208 (1): 3–18. doi : 10.1016/j.ajog.2012.10.880 . ... External links [ edit ] Classification D ICD - 10 : P56 , P83.2 ICD - 9-CM : 773.3 , 778.0 MeSH : D015160 DiseasesDB : 29715 External resources MedlinePlus : 007308 eMedicine : ped/1042 Patient UK : Hydrops fetalis v t e Conditions originating in the perinatal period / fetal disease Maternal factors complicating pregnancy, labour or delivery placenta Placenta praevia Placental insufficiency Twin-to-twin transfusion syndrome chorion / amnion Chorioamnionitis umbilical cord Umbilical cord prolapse Nuchal cord Single umbilical artery presentation Breech birth Asynclitism Shoulder presentation Growth Small for gestational age / Large for gestational age Preterm birth / Postterm pregnancy Intrauterine growth restriction Birth trauma scalp Cephalohematoma Chignon Caput succedaneum Subgaleal hemorrhage Brachial plexus injury Erb's palsy Klumpke paralysis Affected systems Respiratory Intrauterine hypoxia Infant respiratory distress syndrome Transient tachypnea of the newborn Meconium aspiration syndrome Pleural disease Pneumothorax Pneumomediastinum Wilson–Mikity syndrome Bronchopulmonary dysplasia Cardiovascular Pneumopericardium Persistent fetal circulation Bleeding and hematologic disease Vitamin K deficiency bleeding HDN ABO Anti-Kell Rh c Rh D Rh E Hydrops fetalis Hyperbilirubinemia Kernicterus Neonatal jaundice Velamentous cord insertion Intraventricular hemorrhage Germinal matrix hemorrhage Anemia of prematurity Gastrointestinal Ileus Necrotizing enterocolitis Meconium peritonitis Integument and thermoregulation Erythema toxicum Sclerema neonatorum Nervous system Perinatal asphyxia Periventricular leukomalacia Musculoskeletal Gray baby syndrome muscle tone Congenital hypertonia Congenital hypotonia Infections Vertically transmitted infection Neonatal infection rubella herpes simplex mycoplasma hominis ureaplasma urealyticum Omphalitis Neonatal sepsis Group B streptococcal infection Neonatal conjunctivitis Other Miscarriage Perinatal mortality Stillbirth Infant mortality Neonatal withdrawal
Hydrops fetalis is a severe and challenging fetal condition usually defined as the excessive accumulation of fetal fluid within the fetal extravascular compartments and body cavities that manifests as edema, pleural and pericardial effusion and ascites. It is the end-stage of a wide variety of disorders. The cause may be immunologic (immune hydrops fetalis, IHF) or non immunologic (non-immune hydrops fetalis, NIHF), depending on the presence or absence of maternal antibodies against fetal red cell antigens (ABO incompatibility or rhesus (Rh) incompatibility).
There are three main causes for this type: heart or lung problems, severe anemia ( thalassemia ), and genetic defects, including Turner syndrome . The exact cause depends on which form a baby has.
The main clinical features are chaotic rapid conjugate ocular movements, ataxia, somatic myoclonus, and irritability. The syndrome is not progressive. It runs a protracted course with exacerbations and remissions. It has been called the 'dancing eyes, dancing feet syndrome.' Misc - Protracted course with exacerbations and remissions Neuro - Infantile polymyoclonus - Chaotic rapid conjugate ocular movements - Ataxia - Somatic myoclonus - Irritability - Dancing eyes - Dancing feet Inheritance - Autosomal recessive ▲ Close
It can be sub-classified as primary (congenital glaucoma, juvenile glaucoma) or secondary according to the presence or absence of systemic or other ocular anomalies (iridogoniodysgenesis, Stickler syndrome, Coats syndrome). The clinical presentation is variable and is based on age, severity of glaucoma, presence of ocular abnormalities and development of secondary IOP related abnormalities.
A rare, hereditary nonpolyposis colon cancer defined in individuals meeting the Amsterdam criteria for Lynch syndrome, but lacking germline mutations in the mismatch repair genes. It is characterized by a later onset, preferential involvement of distal colon and rectum, lower risk of developing extracolonic cancer, a higher adenoma/carcinoma ratio, a higher differentiation of tumor cells, a more heterogeneous tumor architecture and an infiltrative growth pattern, when compared to Lynch syndrome cases.
Goldstein's toe sign Differential diagnosis Down syndrome or cretinism "Goldstein's Toe Sign" is a feature identified by Dr. ... A greater distance separates the largest two toes of some people exhibiting Down syndrome or cretinism ." [1] References [ edit ] ^ "Who Named It Website Wide distance between the great toe and the adjoining toe; associated with cretinism and trisomy 21.
It is the most common cause of nephrotic syndrome in children. Nephrotic syndrome is comprised of a group of symptoms including protein in the urine (proteinuria), low protein levels in the blood, high cholesterol and triglycerides, an increased risk for blood clots, and swelling.
Epidemiology It has been described in four males from one family. Etiology The syndrome is mapped to the Xq25-q26 region of the X-chromosome. Genetic counseling The syndrome was transmitted in an X-linked recessive manner.
Congenital bowing of the long bones occurs in a number of bone dysplasias, including campomelic dysplasia (114290), kyphomelic dysplasia (211350), hypophosphatasia (241500), Grant syndrome (138930), and osteogenesis imperfecta congenita (166210); however, Moore et al. (1993) were unable to identify a syndrome that fitted the condition found in these sibs.
Long bone bowing can share characteristics of the following disorders: campomelic dysplasia, kyphomelic dysplasia, hypophosphatasia, osteogenesis imperfecta, Stuve-Wiedemann syndrome, and several very rare disorders.
Uncomplicated prenatal bowing of the long bones with dimpling has been described in sibs (Conway, 1958; Mahloudji et al., 1974). Prenatal bowing also occurs with osteogenesis imperfecta, hypophosphatasia, and camptomelic dysplasia. Hall and Spranger (1980) gave a review of congenital bowing of the long bones and identified 3 groups of cases among the 'bewildering variety of bone changes and associated clinical abnormalities which only rarely seem to fall into a recognizable pattern.' Kapur and Van Vloten (1986) observed congenital bowing in a child whose mother had bowing in infancy. Her adult height was 159.5 cm and x-rays showed minimal bowing of the femur.
Association with colobomata in other parts of the eye (incl. ciliary body, zonule, choroid, retina, optic nerve) and complex malformation syndromes (such as CHARGE syndrome) may be observed.
In addition, the high frequency of iris heterochromia-iris coloboma with microphthalmia suggests that an increased density of pigmented cells within the iris stroma may be a contributing factor. Pigment-dispersion syndrome (600510) and pigmentary glaucoma result from iridozonular friction causing disruption of the iris epithelium and deposition of iris pigment on the anterior segment structures. ... Iris colobomas occur as part of complex malformation syndromes, e.g., iris coloboma with ptosis, hypertelorism, and mental retardation (243310), craniofacial dysmorphism with ocular coloboma, absent corpus callosum, and aortic dilatation (218340), and Hirschsprung disease, microcephaly, and iris coloboma (235730). Yuksel et al. (1999) described 2 female sibs with an MCA/MR syndrome consisting of pre- and postnatal growth retardation, iris colobomata, spasticity, facial dysmorphism, and dilated cerebral ventricles. ... Gregory-Evans et al. (2004) provided a detailed review of the molecular genetics of ocular coloboma, including a list of inherited disorders and syndromes in which coloboma is a feature.
Contents 1 Signs and symptoms 2 Pathogenesis 2.1 Genetics 3 Nevoid basal-cell carcinoma syndrome 4 Diagnosis 4.1 Differential diagnosis 4.2 Histology 5 Treatment 5.1 Follow-up 5.2 Recurrence and neoplastic nature 6 See also 7 References 8 External links Signs and symptoms [ edit ] Peak incidence during second and third decades of life. ... They are mainly thought to arise from rests of Serres. [6] Genetics [ edit ] Sporadic (non-syndromic) and syndromic OKCs are associated with mutations in the gene PTCH found on chromosome 9q , which is part of the Hedgehog signaling pathway . [4] [9] PTCH is a tumour suppressor gene . ... This leads to growth of the cyst wall and when removed favours recurrence if following incomplete removal of the epithelium. [6] Nevoid basal-cell carcinoma syndrome [ edit ] Multiple odontogenic keratocysts are a feature, and major diagnostic criteria, of nevoid basal cell carcinoma syndrome (NBCCS, also known as Gorlin-Goltz Syndrome) . Almost all individuals with NBCCS have odontogenic keratocysts which require numerous treatments. Consideration of the syndrome needs to be taken into account if found in children or if multiple OKCs are present; diagnosis of multiple OKCs in a child necessitates referral for genetic evaluation. Histologically, the cysts are indistinguishable to non-syndromic cysts and over 80% will have PTCH mutations. [6] Diagnosis [ edit ] Classic look of an odontogenic keratocyst of the right mandible in the place of a former wisdom tooth.
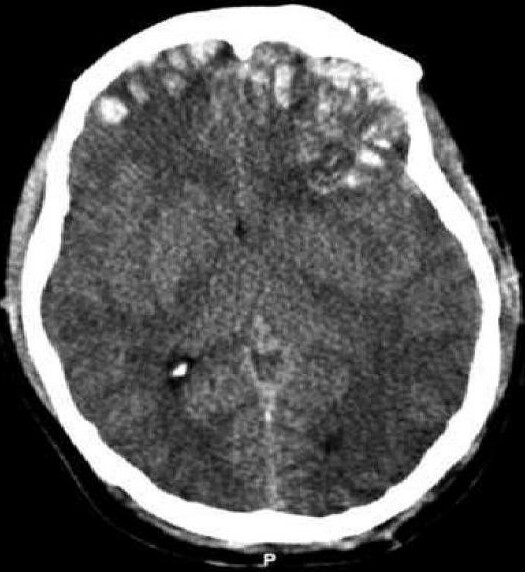
The brain may be contused when it collides with bony protuberances on the inside surface of the skull. [8] The protuberances are located on the inside of the skull under the frontal and temporal lobes and on the roof of the ocular orbit . [9] Thus, the tips of the frontal and temporal lobes located near the bony ridges in the skull are areas where contusions frequently occur and are most severe. [10] For this reason, attention, emotional and memory problems, which are associated with damage to frontal and temporal lobes, are much more common in head trauma survivors than are syndromes associated with damage to other areas of the brain. [11] Features [ edit ] Contusions, which are frequently associated with edema , are especially likely to cause increases in intracranial pressure (ICP) and concomitant crushing of delicate brain tissue. ... Retrieved May 8, 2008 External links [ edit ] Classification D ICD - 10 : S06.2 , S06.3 ICD - 9-CM : 851 MeSH : D000070624 v t e Nonmusculoskeletal injuries of head ( head injury ) and neck Intracranial see neurotrauma Extracranial/ facial trauma eye : Black eye Eye injury Corneal abrasion ear : Perforated eardrum Either/both Penetrating head injury v t e Neurotrauma Traumatic brain injury Intracranial hemorrhage Intra-axial Intraparenchymal hemorrhage Intraventricular hemorrhage Extra-axial Subdural hematoma Epidural hematoma Subarachnoid hemorrhage Brain herniation Cerebral contusion Cerebral laceration Concussion Post-concussion syndrome Second-impact syndrome Dementia pugilistica Chronic traumatic encephalopathy Diffuse axonal injury Abusive head trauma Penetrating head injury Spinal cord injury Anterior spinal artery syndrome Brown-Séquard syndrome Cauda equina syndrome Central cord syndrome Paraplegia Posterior cord syndrome Spinal cord injury without radiographic abnormality Tetraplegia (Quadriplegia) Peripheral nerves Nerve injury Peripheral nerve injury classification Wallerian degeneration Injury of accessory nerve Brachial plexus injury Traumatic neuroma
Furthermore, some others who fit the criteria for PDD-NOS come to professional attention at a later age, compared to those diagnosed with autism. [10] [11] Subgroups [ edit ] Studies suggest that persons with PDD-NOS belong to one of three very different subgroups: [12] A high-functioning group (around 25 percent) whose symptoms largely overlap with that of Asperger syndrome , while also not meeting the criteria for autistic disorder , but who differ from those with Asperger syndrome in terms of having a lag in language development and/or mild cognitive impairment. [12] (The criteria for Asperger syndrome excludes a speech delay or a cognitive delay in early life. [13] ) Another group (around 25 percent) whose symptoms more closely resemble those of autistic disorder, but do not fully meet all its diagnostic signs and symptoms. ... "Specifying PDD-NOS: a comparison of PDD-NOS, Asperger syndrome, and autism". J Am Acad Child Adolesc Psychiatry . 43 (2): 172–80. doi : 10.1097/00004583-200402000-00012 . ... ISBN 1585623415 External links [ edit ] Classification D ICD - 10 : F84.9 ICD - 9-CM : 299.9 299.80 v t e Pervasive developmental disorders and autism spectrum Main Causes Comorbid conditions Epidemiology Heritability Societal and cultural aspects Medical model Therapies Diagnoses Autism spectrum ( High-functioning autism Classic autism Asperger syndrome Pervasive developmental disorder not otherwise specified Childhood disintegrative disorder Rett syndrome ) Related conditions Alexithymia Attention deficit hyperactivity disorder Anxiety disorder ( obsessive–compulsive disorder ) Late talker Epilepsy Fragile X syndrome Hyperlexia Savant syndrome Sensory processing disorder Intellectual disability Developmental coordination disorder Multiple complex developmental disorder Controversies Autism rights movement Autistic enterocolitis Facilitated communication MMR vaccine Rapid prompting method Thiomersal ( Chelation ) Diagnostic scales Gilliam Asperger's disorder scale Autism Diagnostic Observation Schedule Autism Diagnostic Interview Autism-spectrum quotient Childhood Autism Rating Scale Lists Autism-related topics Fictional characters Schools
A rare disorder of the anterior segment of the eye characterized by ocular infection by human-pathogenic fungi, most commonly Aspergillus , Candida , or Fusarium species, which gain access into the corneal stroma through a defect in the corneal epithelium. Risk factors include trauma, ocular surface disease, contact lenses, or immunocompromised state. Patients present with pain, foreign body sensation, redness, photophobia, tearing, secretion, or blurred vision. The condition may be complicated by corneal destruction and perforation, endophthalmitis, scleritis, and panophthalmitis.