-
Spastic Ataxia 8, Autosomal Recessive, With Hypomyelinating Leukodystrophy
Omim
Affected individuals initially have hypotonia and later develop ataxia, spasticity, and a pyramidal syndrome with weakness and loss of ambulation. ... Initial features included hypotonia, which developed into a pyramidal syndrome with weakness and hyperreflexia mainly involving the lower limbs, as well as truncal and limb ataxia, dysarthria, and head titubation.
-
Asphyxiating Thoracic Dystrophy
Medlineplus
Asphyxiating thoracic dystrophy, also known as Jeune syndrome, is an inherited disorder of bone growth characterized by a narrow chest, short ribs, shortened bones in the arms and legs, short stature, and extra fingers and toes (polydactyly). ... Several of these disorders, including asphyxiating thoracic dystrophy, are sometimes classified more specifically as short rib-polydactyly syndromes (SRPSs) based on their signs and symptoms.
-
Teratospermia
Wikipedia
External links [ edit ] teratozoospermia.net v t e Male diseases of the pelvis and genitals Internal Testicular Orchitis Hydrocele testis Testicular cancer Testicular torsion Male infertility Aspermia Asthenozoospermia Azoospermia Hyperspermia Hypospermia Oligospermia Necrospermia Teratospermia Epididymis Epididymitis Spermatocele Hematocele Prostate Prostatitis Acute prostatitis Chronic bacterial prostatitis Chronic prostatitis/chronic pelvic pain syndrome Asymptomatic inflammatory prostatitis Benign prostatic hyperplasia Prostate cancer Seminal vesicle Seminal vesiculitis External Penis Balanoposthitis / Balanitis Balanitis plasmacellularis Pseudoepitheliomatous keratotic and micaceous balanitis Phimosis Paraphimosis Priapism Sexual dysfunction Erectile dysfunction Peyronie's disease Penile cancer Penile fracture Balanitis xerotica obliterans Other Hematospermia Retrograde ejaculation Postorgasmic illness syndrome

-
Multisystem Proteinopathy
Wikipedia
However, IBMPFD and IBMPFD/ALS are now considered outdated classifications and are more properly referred to as MSP, [1] [2] as the disease is clinically heterogeneous and its phenotypic spectrum extends beyond IBM, PDB, FTD, and ALS to include motor neuron disease, Parkinson’s disease features, and ataxia features. [3] [4] Although MSP is rare, growing interest in this syndrome derives from the molecular insights the condition provides into the etiological relationship between common age-related degenerative diseases of muscle, bone, and brain. ... "Rare Inherited forms of Paget's Disease and Related Syndromes" . Calcif. Tissue Int . 104 (5): 501–516. doi : 10.1007/s00223-019-00520-5 .
-
Mitochondrial Complex I Deficiency, Nuclear Type 15
Omim
Brain imaging showed signal alterations in the basal ganglia consistent with Leigh syndrome. EEG showed generalized slowing with multifocal spikes. ... INHERITANCE - Autosomal recessive GROWTH Other - Intrauterine growth restriction (IUGR) - Failure to thrive HEAD & NECK Ears - Hearing impairment Eyes - Nystagmus - Optic atrophy - Poor eye contact CARDIOVASCULAR Heart - Hypertrophic cardiomyopathy (1 patient) SKELETAL - Limited joint movement - Joint contractures Spine - Kyphosis MUSCLE, SOFT TISSUES - Myopathy - Hypotonia NEUROLOGIC Central Nervous System - Encephalopathy - Poor or lack of developmental progress - Irritability - Dystonia - Spastic tetraplegia - Hyperreflexia - Poor spontaneous movements - Failure to interact with surroundings - Seizures, episodic (in some patients) - Brain imaging shows supratentorial and infratentorial atrophy - Demyelination - Basal ganglia changes consistent with Leigh syndrome (in some patients) METABOLIC FEATURES - Metabolic acidosis LABORATORY ABNORMALITIES - Increased serum and CSF lactate - Mitochondrial respiratory complex I deficiency in various tissues MISCELLANEOUS - Neonatal onset - Death in infancy may occur MOLECULAR BASIS - Caused by mutation in the NADH-ubiquinone oxidoreductase complex assembly factor 4 gene (NDUFAF4, 611776.0001 ) ▲ Close
-
Odynophagia
Wikipedia
External links [ edit ] Quotations related to Odynophagia at Wikiquote Classification D ICD - 10 : R13 ICD - 9-CM : 787.20 DiseasesDB : 17942 v t e Symptoms and signs relating to the human digestive system or abdomen Gastrointestinal tract Nausea Vomiting Heartburn Aerophagia Pagophagia Dysphagia oropharyngeal esophageal Odynophagia Bad breath Xerostomia Hypersalivation Burping Wet burp Goodsall's rule Chilaiditi syndrome Dance's sign Aaron's sign Arapov's sign Markle sign McBurney's point Sherren's triangle Radiologic signs : Hampton's line Klemm's sign Accessory liver : Councilman body Mallory body biliary: Boas' sign Courvoisier's law Charcot's cholangitis triad / Reynolds' pentad cholecystitis ( Murphy's sign Lépine's sign Mirizzi's syndrome ) Nardi test Defecation Flatulence Fecal incontinence Encopresis Fecal occult blood Rectal tenesmus Constipation Obstructed defecation Diarrhea Rectal discharge Psoas sign Obturator sign Rovsing's sign Hamburger sign Heel tap sign Aure-Rozanova's sign Dunphy sign Alder's sign Lockwood's sign Rosenstein's sign Abdomen Pain Abdominal pain Acute abdomen Colic Baby colic Abdominal guarding Blumberg sign Distension Abdominal distension Bloating Ascites Tympanites Shifting dullness Ascites Fluid wave test Masses Abdominal mass Hepatosplenomegaly Hepatomegaly Splenomegaly Other Jaundice Mallet-Guy sign Puddle sign Ballance's sign Aortic insufficiency Castell's sign Kehr's sign Cullen's sign Grey Turner's sign Hernia Howship–Romberg sign Hannington-Kiff sign Other Cupola sign Fothergill's sign Carnett's sign Sister Mary Joseph nodule This medical symptom article is a stub .
-
Vaso-Occlusive Crisis
Wikipedia
The most common complaint is of pain, and recurrent episodes may cause irreversible organ damage. [2] One of the most severe forms is the acute chest syndrome which occurs as a result of infarction of the lung parenchyma. ... Other types of vaso-occlusive crisis in sickle cell anemia include dactylitis , priapism , abdominal pain , and jaundice . 1) Full blood count to check for Hemoglobin levels and 2) Rapid diagnostic test (RDT) for Malaria to be able to rule out malaria in the patient Contents 1 Diagnosis 2 Management 3 References 4 External links Diagnosis [ edit ] Diagnosis of vaso-occlusive crisis is based on clinical manifestations, complete blood count with white blood cell differential , platelet count, reticulocyte count, and comprehensive metabolic panel with liver and kidney function tests . [3] Typical lab findings include acute drop in hemoglobin concentration, increased platelet count, increased reticulocyte count, and elevated serum urea . [4] Management [ edit ] The management of an acute event of vaso-occlusive crisis is the use of potent analgesics ( opioids ), [5] rehydration with normal saline or Ringer's lactate , treatment of malaria (whether symptomatic or not) using artemisinin combination therapy, and the use of oxygen via face mask, especially for acute chest syndrome. Hyperbaric oxygen has also been shown to be a useful adjunct in pain reduction. [6] Antibiotics may be utilized because patients usually have occult infection due to a "functional asplenia ".
-
Foreign Body Granuloma
Wikipedia
External links [ edit ] Classification D ICD - 10 : L92.3 ( ILDS L92.300) MeSH : D015745 v t e Cutaneous keratosis, ulcer, atrophy, and necrobiosis Epidermal thickening keratoderma : Keratoderma climactericum Paraneoplastic keratoderma Acrokeratosis paraneoplastica of Bazex Aquagenic keratoderma Drug-induced keratoderma psoriasis Keratoderma blennorrhagicum keratosis : Seborrheic keratosis Clonal seborrheic keratosis Common seborrheic keratosis Irritated seborrheic keratosis Seborrheic keratosis with squamous atypia Reticulated seborrheic keratosis Dermatosis papulosa nigra Keratosis punctata of the palmar creases other hyperkeratosis : Acanthosis nigricans Confluent and reticulated papillomatosis Callus Ichthyosis acquisita Arsenical keratosis Chronic scar keratosis Hyperkeratosis lenticularis perstans Hydrocarbon keratosis Hyperkeratosis of the nipple and areola Inverted follicular keratosis Lichenoid keratosis Multiple minute digitate hyperkeratosis PUVA keratosis Reactional keratosis Stucco keratosis Thermal keratosis Viral keratosis Warty dyskeratoma Waxy keratosis of childhood other hypertrophy: Keloid Hypertrophic scar Cutis verticis gyrata Necrobiosis / granuloma Necrobiotic/palisading Granuloma annulare Perforating Generalized Subcutaneous Granuloma annulare in HIV disease Localized granuloma annulare Patch-type granuloma annulare Necrobiosis lipoidica Annular elastolytic giant-cell granuloma Granuloma multiforme Necrobiotic xanthogranuloma Palisaded neutrophilic and granulomatous dermatitis Rheumatoid nodulosis Interstitial granulomatous dermatitis / Interstitial granulomatous drug reaction Foreign body granuloma Beryllium granuloma Mercury granuloma Silica granuloma Silicone granuloma Zirconium granuloma Soot tattoo Tattoo Carbon stain Other/ungrouped eosinophilic dermatosis Granuloma faciale Dermis / localized CTD Cutaneous lupus erythematosus chronic: Discoid Panniculitis subacute : Neonatal ungrouped: Chilblain Lupus erythematosus–lichen planus overlap syndrome Tumid Verrucous Rowell's syndrome Scleroderma / Morphea Localized scleroderma Localized morphea Morphea–lichen sclerosus et atrophicus overlap Generalized morphea Atrophoderma of Pasini and Pierini Pansclerotic morphea Morphea profunda Linear scleroderma Atrophic / atrophoderma Lichen sclerosus Anetoderma Schweninger–Buzzi anetoderma Jadassohn–Pellizzari anetoderma Atrophoderma of Pasini and Pierini Acrodermatitis chronica atrophicans Semicircular lipoatrophy Follicular atrophoderma Linear atrophoderma of Moulin Perforating Kyrle disease Reactive perforating collagenosis Elastosis perforans serpiginosa Perforating folliculitis Acquired perforating dermatosis Skin ulcer Pyoderma gangrenosum Other Calcinosis cutis Sclerodactyly Poikiloderma vasculare atrophicans Ainhum / Pseudo-ainhum This article about a disease , disorder, or medical condition is a stub .

-
Acute Monocytic Leukemia
Wikipedia
External links [ edit ] Classification D ICD - 10 : C93.0 ICD - 9-CM : 206.0 MeSH : D007948 SNOMED CT : 22331004 Image at hmds.org.uk v t e Myeloid -related hematological malignancy CFU-GM / and other granulocytes CFU-GM Myelocyte AML : Acute myeloblastic leukemia M0 M1 M2 APL/M3 MP Chronic neutrophilic leukemia Monocyte AML AMoL/M5 Myeloid dendritic cell leukemia CML Philadelphia chromosome Accelerated phase chronic myelogenous leukemia Myelomonocyte AML M4 MD-MP Juvenile myelomonocytic leukemia Chronic myelomonocytic leukemia Other Histiocytosis CFU-Baso AML Acute basophilic CFU-Eos AML Acute eosinophilic MP Chronic eosinophilic leukemia / Hypereosinophilic syndrome MEP CFU-Meg MP Essential thrombocytosis Acute megakaryoblastic leukemia CFU-E AML Erythroleukemia/M6 MP Polycythemia vera MD Refractory anemia Refractory anemia with excess of blasts Chromosome 5q deletion syndrome Sideroblastic anemia Paroxysmal nocturnal hemoglobinuria Refractory cytopenia with multilineage dysplasia CFU-Mast Mastocytoma Mast cell leukemia Mast cell sarcoma Systemic mastocytosis Mastocytosis : Diffuse cutaneous mastocytosis Erythrodermic mastocytosis Adult type of generalized eruption of cutaneous mastocytosis Urticaria pigmentosa Mast cell sarcoma Solitary mastocytoma Systemic mastocytosis Xanthelasmoidal mastocytosis Multiple/unknown AML Acute panmyelosis with myelofibrosis Myeloid sarcoma MP Myelofibrosis Acute biphenotypic leukaemiaCEBPA, KMT2A, DNMT3A, FANCB, FANCA, FANCM, SBDS, SLX4, BRCA1, FANCG, FANCF, FANCE, CTC1, FANCD2, FANCC, RAD51C, RAD51, ERCC4, UBE2T, BRIP1, BLM, XRCC2, PALB2, FANCI, FANCL, MAD2L2, RUNX1, ELANE, BCL2, RUNX1T1, ABCB1, IDH1, KIT, CD34, MECOM, NUP98, IDH2, TBC1D9, FLT3, TP53, NCAM1, CCR7, NPM1, TSC2, SCT, CSF3, CD33, KAT6A, ASXL1, CXCR4, MYH11, JAK2, MDM2, CSF3R, PIK3CD, CPOX, MPO, EBP, ABCC1, TET2, TBX22, MCL1, EZH2, BCR, WT1, VEGFA, VDR, CTNNB1, HOXA9, PIK3CA, MIR155, PIK3CB, MDM4, PIK3CG, ABCG2, CDKN2B, CD38, TSC1, MLLT3, GATA2, BAALC, IL2, NRAS, IL6, NSD1, MSH3, PTP4A3, HIF1A, CDKN2A, CD19, CSF2, CALR, PTPN11, CREBBP, FAS, ABCC3, KRAS, RARA, ABL1, ACTB, ISG20, CBFB, AKT1, SPP1, IL18, BAX, CXCL8, MLLT10, LGALS3, GFI1, MLANA, FLT1, TESC, MTOR, GABPA, IL2RA, IL3RA, HAVCR2, MAPK8, CDKN1B, PML, PTPA, CDK9, SEPTIN6, MIR34A, DCK, MAP2K7, NFE2L2, VEGFC, AURKA, SMR3B, SUB1, KDM1A, NFATC1, NXT1, VIM, PPARG, IL1RAP, NME1, ELL, HMGA2, DEK, NOTCH1, ASXL2, NR4A3, ARID1B, STAT3, CD200, TXNIP, MVP, LRP1, EFS, TRIB2, KDR, FOXP3, HPGDS, RET, BCL2L11, EIF2AK2, BCLAF1, ADGRG1, SRSF2, SLC12A3, MRPL28, BABAM2, SOAT1, MEIS1, INPP5D, SIRT6, LMO2, NT5E, H3P10, NUP214, CD6, FGFR1, ALL1, CD44, MIR335, FABP4, ETS1, CD80, ERG, DAPK1, CAB39L, ERCC2, SLCO6A1, CBL, LIN28B, ATM, DNMT1, MALAT1, GSTK1, CDA, MIR142, CSF1R, ANPEP, ABO, H3P9, CHEK1, GSTT1, MIR29B2, MARCKSL1, MIR29B1, AHR, GATA1, WLS, XIAP, CTDSPL, CIB1, MTSS1, MIR451A, HDAC4, ATG7, MIR223, HDAC9, MIR483, IKBKE, NCOR1, LEF1-AS1, MIR217, LILRB2, IKZF1, NR1I3, ABI1, CD96, NCOA2, MIR17HG, TANK, BCL2L10, MIR29A, MIR363, SEMA3A, ABCB6, H4C15, LRPPRC, TRIM13, MIR342, GPHN, APOBEC3B, CARTPT, CDKN2B-AS1, LOC646762, H4C5, H4C8, H4C3, SYCE1L, H4C11, H4C12, MIR181A1HG, H4C6, H4C4, H4C1, GFI1B, H4C9, HOTTIP, MIR3151, KLRC4-KLRK1, MLRL, APOBEC3A_B, CDR3, CSAG2, PERCC1, RN7SL263P, PTP4A2, H4C2, H4C13, CXADRP1, H4C14, NCF1, NCR1, NCR2, MIR663A, KLF4, POTEF, MIR210, AURKB, USP2, VTRNA2-1, ASH2L, SOCS3, MBD4, DDX18, SOCS2, INPP4B, DLK1, BMI1P1, PIR, GAS7, CNTNAP1, MIR212, KLHL1, MIR21, ZBTB7A, HERC5, GLIS2, ADIPOR1, FIS1, DERL3, TWIST2, TMEM132D, SYCP3, H4-16, EHD3, ERVW-1, CD274, TBK1, OSCP1, CCDC26, SIRPA, IL23R, CLEC12A, ZNF296, APOBEC3A, CTAG1A, SYVN1, MAML2, CHORDC1, WT1-AS, BIRC6, TIGAR, SLC12A9, RPRM, PBK, PRDM16, ZC3H15, SOX6, VSIR, GORASP1, RMDN3, WNK1, PHF23, TUG1, ASRGL1, ULBP1, PARP9, UGT1A1, BCL11A, CMPK1, PHF6, EBF3, LATS2, MIR203A, MIR126, MIR130A, CHEK2, MIR132, MIR143, MIR144, MIR145, MIR146A, KAT7, FGFR1OP, GLIPR1, MIR149, MIR150, LILRB4, MIR183, BCORL1, SLC27A5, MLLT11, MIR192, SEPTIN9, KDM5B, NES, AKAP13, ACOT7, GNL3, MIR122, TUSC7, SAMHD1, FRYL, PRKD2, CADM1, DAPK2, PIGN, PRAME, SF3B1, RTL1, SIRT3, DICER1, CSAG3, KDM6B, SIPA1L3, ARHGAP26, CASC15, MIRLET7B, DKK1, KLRK1, ZHX2, MIR191, AADAC, TFPI2, ATN1, FOSB, FLNA, FOXO3, VEGFD, FGFR3, FDXR, FCGRT, FCGR3B, FCGR3A, FCGR1A, PTK2B, F2, EVPL, ETV6, ETS2, ESR1, EPHB4, EPHB2, EPHA1, EPAS1, EP300, ELN, EIF4B, EGFR, EGF, E2F3, E2F1, GAS6, KAT2A, GEM, NR4A1, IL7R, IL7, IL6ST, IL3, IL2RG, IGFBP2, IFNG, IDUA, HTC2, HOXC5, HOXB2, HOXA4, HMOX1, GLI1, HMMR, HLF, HLA-DRB4, HLA-A, HIP1, H2AX, MSH6, GSTM1, GRN, GNA12, GLUL, GLI3, DUSP7, ARID3A, ZMYM2, DRD2, CD47, CD40LG, CD40, CD36, CD14, CBFA2T3, CASR, CASP9, CASP1, BST1, BRAF, OPN1SW, BCAT1, ATR, ASAH1, ARR3, AR, APOE, APOA1, BIRC5, AMFR, AKR1B1, JAG1, AGER, TLE5, ADM, ACR, CD74, CDH2, CDK2, CTSK, DGUOK, TIMM8A, DECR1, ACE, DBH, DAP, CYP7A1, CYP3A4, CYP2D6, CYP2C19, CXADR, CTSL, CTSB, CDK7, CCN2, CTAG1B, CSNK1A1, ABCC2, CIRBP, CHD4, CEL, CEBPB, CDKN3, CDKN1C, CDKN1A, CDK8, CXCR2, TNFRSF9, IL17A, IDO1, SPN, SPG7, SPARC, SOS1, SMARCB1, PMEL, FBXW4, CX3CL1, CCL2, SATB1, S100A8, RRM1, RREB1, RPS6KA1, RORA, ROBO2, RNF2, RING1, RGS2, KDM5A, RAF1, MOK, NECTIN2, PVR, PTPRA, PTBP1, PSMB9, SSX2, STAT5A, STAT5B, TLR2, YWHAE, XPO1, XBP1, VCAM1, UBE2I, TYR, TXN, TTC4, TRAF2, NR2C2, TOP1, TLR4, TLE4, SYK, TLE1, TIAM1, THPO, TFRC, TFE3, TERT, PRDX2, TRBV20OR9-2, TBCE, TAZ, MAP3K7, SYT1, PSMA7, MAPK7, MAPK1, SMAD5, MT1E, MSH2, MSD, MMP9, MMP2, MLLT6, AFDN, MLLT1, MITF, CXCL9, MAP3K5, MATK, SMAD4, MYO1F, LLGL1, LCP2, LCK, RPSA, LAMP2, KIR3DL1, JARID2, JAK1, ITGB2, ITGAM, IRF7, IRF3, MTHFR, MYB, PRKAR1A, PIM1, PRKAB1, PRKAA2, PRKAA1, PPP2R2A, POU4F1, PMAIP1, PLS3, PLG, PLCG1, PLA2G4A, PKD1, PIN1, PAX5, MYC, PAFAH1B1, PA2G4, ORC5, NONO, NM, NFE2, NF1, NEDD8, SEPTIN2, NCL, MYH9, MYH8, RELA
-
Pyramidal Signs
Wikipedia
Flexion [ edit ] These phenomena are present if the fingers of the foot are going into the flection position: Rossolimo – Reaction on percussion of all fingertips. ( see video ) Clinical significance [ edit ] Parkinsonian-Pyramidal syndrome (PPS) are a combination of both pyramidal and parkinsonian signs that manifest in various neurodegenerative diseases. [3] See also [ edit ] Motor neurons Amyotrophic Lateral Sclerosis Reflexes References [ edit ] ^ Grant, Gerald A.; Xu, Linda; Ellenbogen, Richard G. (2018). "3 - Clinical Evaluation of the Nervous System". ... Retrieved 9 September 2020 . ^ Tranchant, Christine; Koob, Meriam; Anheim, Mathieu (June 2017). "Parkinsonian-Pyramidal syndromes: A systematic review". Parkinsonism & Related Disorders . 39 : 4–16. doi : 10.1016/j.parkreldis.2017.02.025 .SETX, SIGMAR1, LMNB1, CYP27A1, BSCL2, ADAR, SAMHD1, CAMTA1, ETHE1, ATXN10, RTTN, MLH3, TREX1, COQ2, GMPPB, POMT2, RRM2B, NDUFA13, FAN1, POMT1, ERLIN2, SQSTM1, RNF113A, GAN, ADD3, PLA2G6, PRKRA, SYNJ1, CTDP1, ERAP1, AIMP1, DNAJC6, DNM1L, BCAP31, SLC25A15, RNASEH2A, SPG21, TMEM106B, TLR4, VWA3B, COA8, NKX6-2, FAM126A, MPLKIP, TTBK2, IL23R, RNASEH1, VPS13C, NALCN, UBAC2, NDUFS7, GTF2H5, ATXN8, SNORD118, POMK, RNASEH2C, CLPB, SPG11, CTC1, PANK2, L2HGDH, RNASEH2B, FKRP, SEMA4A, IFIH1, ALS2, SLC12A5, TBC1D24, MYORG, COQ8A, POMGNT1, TTPA, KLRC4, MAPT, KARS1, GTF2E2, HTT, HLA-B, IDUA, IL10, IL12A, KCNC3, NDUFS2, KRAS, EPCAM, TGFBR2, MEFV, MLH1, MSH2, MSH6, GRM1, GM2A, GBE1, FUS, FUCA1, EXT2, EXT1, ERCC3, ERCC2, EPRS1, CCR1, CAPN1, C4A, BMPR1A, FAS, ALDH3A2, NAGA, IL12A-AS1, PPP2R2B, PODXL, SLC2A1, SCN1B, SLC6A3, SOX10, PMS1, PLP1, PSMB8, RPS20, PIK3CA, STAT4, ELOVL4, PHYH, SURF1, PEX10, TBP, PEX7, ATXN8OS, PMS2, FBXO7, MAD2L1BP, SPTBN2, HSPB3, ATXN2, TMEM240, OPN1MW2, OPN1MW3, ATXN7, NEFL, OPN1MW, KIF1B, OPA1, ATXN3, PLEKHG4, LY6E, THG1L, KIF5A, ITPR1, SBF1, MORC2, HSPB2, HSPB1, HSD17B4, SACS, C19orf12, TPO
-
Nodular Regenerative Hyperplasia
Wikipedia
It is associated with rheumatoid arthritis, Felty syndrome, myeloproliferative disorders, liver, kidney and bone marrow transplantation, cytotoxic drugs like azathioprine, mercaptopurine, thioguanine, antiretroviral drugs for HIV like didanosine and vitamin A. ... External links [ edit ] Classification D ICD - 10 : K76.8 External resources Orphanet : 48372 v t e Digestive system neoplasia GI tract Upper Esophagus Squamous cell carcinoma Adenocarcinoma Stomach Gastric carcinoma Signet ring cell carcinoma Gastric lymphoma MALT lymphoma Linitis plastica Lower Small intestine Duodenal cancer Adenocarcinoma Appendix Carcinoid Pseudomyxoma peritonei Colon/rectum Colorectal polyp : adenoma , hyperplastic , juvenile , sessile serrated adenoma , traditional serrated adenoma , Peutz–Jeghers Cronkhite–Canada Polyposis syndromes: Juvenile MUTYH-associated Familial adenomatous / Gardner's Polymerase proofreading-associated Serrated polyposis Neoplasm: Adenocarcinoma Familial adenomatous polyposis Hereditary nonpolyposis colorectal cancer Anus Squamous cell carcinoma Upper and/or lower Gastrointestinal stromal tumor Krukenberg tumor (metastatic) Accessory Liver malignant : Hepatocellular carcinoma Fibrolamellar Hepatoblastoma benign : Hepatocellular adenoma Cavernous hemangioma hyperplasia : Focal nodular hyperplasia Nodular regenerative hyperplasia Biliary tract bile duct : Cholangiocarcinoma Klatskin tumor gallbladder : Gallbladder cancer Pancreas exocrine pancreas : Adenocarcinoma Pancreatic ductal carcinoma cystic neoplasms : Serous microcystic adenoma Intraductal papillary mucinous neoplasm Mucinous cystic neoplasm Solid pseudopapillary neoplasm Pancreatoblastoma Peritoneum Primary peritoneal carcinoma Peritoneal mesothelioma Desmoplastic small round cell tumor This article about a disease , disorder, or medical condition is a stub .

-
Androgenetic Alopecia
Medlineplus
In women, this form of hair loss is associated with an increased risk of polycystic ovary syndrome (PCOS). PCOS is characterized by a hormonal imbalance that can lead to irregular menstruation, acne, excess hair elsewhere on the body (hirsutism), and weight gain. ... Researchers continue to investigate the connection between androgenetic alopecia and other medical conditions, such as coronary heart disease and prostate cancer in men and polycystic ovary syndrome in women. They believe that some of these disorders may be associated with elevated androgen levels, which may help explain why they tend to occur with androgen-related hair loss.SRD5A2, AR, ABCC2, SUPV3L1, VDR, ZFP36, MTHFR, TNFRSF10A, BRD4, ZDHHC13, HR, PRKAR1A, CRH, PARP1, RHOA, WNT10A, C1orf127, FAF1, MKLN1-AS, TBX15, HOXD-AS2, ARL17B, LINC01432, SSPN, SLC14A2, FAM53B, EMC2, HDAC9, EDAR, MAPT-AS1, DRAIC, DKK2, KLF15, MEMO1, RSPO2, KANSL1, MRPS22, LINC00670, LRMDA, OFCC1, DPY30, GORAB, SPPL2C, THADA, GORAB-AS1, EBF1, RUNX1, MAPT, MKLN1, EIF3E, OPHN1, IRF4, FGF5, AGA, EDA2R, KLK3, TGFB1, GGCT, CD200, DKK1, CTNNB1, IGF1, CD34, DPP4, CYP27B1, COX8A, CRP, COL17A1, CARD14, PRNP, NLRP3, FGF2, CDKN2A, MS4A1, CASP3, C4BPA, MIR223, MIR451A, MIR146B, BDNF, XIAP, AGXT, AGT, AKR1C4, IL1B, KRT20, VEGFA, PTPN1, SHBG, SRD5A1, PPARA, ABCB1, OTC, PRDX2, TGFB1I1, TLR4, TNF, TP53, WNT10B, GHR, NFE2L2, NCOA4, LEP, KRT5, ABCB6, DHRS9, IL17A, MMRN1, TBC1D9, PTGDS, HPGDS, TGFBR1

-
Type Ii Collagen Disorders Overview
Gene_reviews
Disorders with Known Genetic Etiology to Consider in the Differential Diagnosis of Type II Collagen Disorders View in own window Type II Collagen Disorder Differential Diagnosis Disorder Gene(s) MOI Clinical Features of Differential Diagnosis Disorder Overlapping w/type II collagen disorders Distinguishing from type II collagen disorders Most severe 1 – achondrogenesis type II; hypochondrogenesis; platyspondylic dysplasia, Torrance type Severe OI (see COL1A1/2-OI) COL1A1 COL1A2 CRTAP P3H1 ( LEPRE1 ) PPIB AD AR Poor/delayed ossification Short limbs Multiple fractures & deformities of long bones No extraskeletal type II collagen characteristic abnormalities 2 Hypophosphatasia ALPL AD AR Poor/delayed ossification Absent ossification of the skull Absent ossification of posterior elements of vertebrae Low serum ALP No extraskeletal type II collagen characteristic abnormalities 2 Achondrogenesis type 1A (OMIM 200600) TRIP11 AR Poor/delayed ossification Hydropic appearance Poorly ossified skull bones Short, thin, easily fractured ribs Tubular bones more severely shortened & bowed Achondrogenesis type 1B SLC26A2 AR Poor ossification Flat face, short neck Hydropic appearance Crescent-shaped ilia Extremely short limbs w/loss of longitudinal orientation Short fingers & toes Hypoplasia of thorax Protuberant abdomen Atelosteogenesis type 2 SLC26A2 AR Often delayed ossification of upper thoracic vertebra & pubic bone Short limbs Cleft palate, distinctive facial features (midface retrusion, depressed nasal bridge, micrognathia) Hitchhiker (abducted) thumbs Poor/delayed ossification less severe than severe type II collagen disorder Distal tapering of humeri Hypoplastic fibulae Diastrophic dysplasia SLC26A2 AR Short limbs Spine & joint deformities Hitchhiker thumbs/toes Dyssegmental dysplasia, Silverman-Handmaker type (OMIM 224410) (may include Rolland-Desbuquois type) HSPG2 AR Narrow chest Short limbs Cleft palate Vertebral disorganization Marked differences in size & shape of vertebral bodies (anisospondyly) Bowed long bones Severe to moderately severe – Kniest dysplasia; SEDC; SEMD, Strudwick type Metatropic dysplasia (see TRPV4 -Associated Disorders TRPV4 AD Limb shortening Spine & joint deformities Narrow transverse diameter of thorax Vertebral bodies diamond/oval shape, no coronal clefts Medially placed (inset) pedicles More distal flaring in femur & proximal tibia Most often no facial, ophthalmic, or auditory abnormalities 2 Normal ossification of skeleton Intermediate severity – spondyloperipheral dysplasia; SED w/metatarsal shortening (Czech dysplasia); 3 Stickler syndrome type 1 MED, AD COL9A1 COL9A2 COL9A3 COMP MATN3 AD Presents in early childhood, usually w/pain in hips &/or knees No facial, ophthalmic, or auditory abnormalities 2 Often no spine involvement MED, recessive SLC26A2 AR Presents in early childhood, usually w/pain in hips &/or knees Brachydactyly No facial, ophthalmic, or auditory abnormalities 2 Clubfeet Cleft palate Double-layered patella observed on lateral knee radiographs in 60% Often no spine involvement Progressive pseudorheumatoid dysplasia (SED w/progressive arthropathy) CCN6 AR Joint pain, multiple joint contractures, & prominent interphalangeal joints Short stature Moderate platysplondyly Widening of the metaphyses, enlarged ephiphyses Early osteoarthritis No facial, ophthalmic, or auditory abnormalities 2 Toes are distinct from SED w/metatarsal shortening 3 Stickler syndrome types 2, 3, 4, & 5 COL11A1 COL11A2 COL9A1 COL9A2 COL9A3 AD AR Craniofacial, ophthalmic, & auditory abnormalities Skeletal manifestations on x-ray (spondyloepiphyseal dysplasia) & joint involvement Ophthalmologic complications often less severe than Stickler type 1 Ocular phenotypes in other Stickler subtypes most often comprise type 2 congenital vitreous anomaly ("beaded" vitreous phenotype). ... Disorders of Unknown Etiology to Consider in the Differential Diagnosis of Type II Collagen Disorders View in own window Type II Collagen Disorder Differential Diagnosis Disorder Clinical Features of Differential Diagnosis Disorder Overlapping w/type II collagen disorders Distinguishing from type II collagen disorders Intermediate severity – spondyloperipheral dysplasia; SED w/metatarsal shortening (Czech dysplasia) 1 ; Stickler syndrome type 1 Juvenile idiopathic arthritis Presents in childhood, usually w/joint pain No facial, ophthalmic, or auditory abnormalities 3 Calve-Legg Perthes 2 Presents in childhood, usually w/hip pain No facial, ophthalmic, or auditory abnormalities 3 Often unilateral, & if bilateral (10%-15% of cases) often asynchronous involvement (femoral heads in different stages of disease) 2 No spine involvement Mild severity – mild SED w/premature arthrosis Rheumatoid arthritis Joint pain Radiographic skeletal changes of osteoarthritis More pronounced clinical & laboratory signs of inflammation Juvenile idiopathic arthritis Joint pain No facial, ophthalmic, or auditory abnormalities 3 Often presents at younger age AD = autosomal dominant; ALP = alkaline phosphatase test; AR = autosomal recessive; MED = multiple epiphyseal dysplasia; MOI = mode of inheritance; OI = osteogenesis imperfecta; SED = spondyloepiphyseal dysplasia; SEDC = spondyloepiphyseal dysplasia congenita; SEMD = spondyloepimetaphyseal dysplasia 1. ... Consider prophylactic retinopexy in Stickler syndrome type 1 ( COL2A1 -related) Hearing impairment Hearing aids &/or surgery if indicated Joint problems (laxity, contractures, pain due to early-onset arthrosis) Referral to orthopedic surgeon for evaluation Referral to physiotherapist Referral to occupational therapist if indicated Analgesics Advice on joint-friendly activities (e.g., swimming, cycling) Consider need for a mobility device. ... Recommended Surveillance for Individuals with Type II Collagen Disorders View in own window System/ Concern Evaluation Frequency General health Physical examination Annually or as indicated Cervical spine Flexion-extension radiograph Flexion-extension MRI if instability & compression on radiographs or limited interpretation on radiographs Every 2-3 yrs in those w/severe type II collagen disorder & no instability Thoracolumbar spine Clinical examination Radiographs when indicated Every 6-12 mos, depending on severity Respiratory Pulmonary function tests Polysomnography On a regular basis in individuals w/severe type II collagen disorder or severe, progressive kyphoscoliosis Eyes Dilated eye examination Annually unless complications Consider prophylactic retinopexy in Stickler syndrome type 1 ( COL2A1 -related) ENT/ Mouth Hearing evaluation Evaluation for cleft palate & palatal insufficiency Every 6-12 mos depending on severity Feeding Swallowing assessment On a regular basis until normal feeding Musculoskeletal Clinical examination Referral to orthopedic surgeon if indicated Referral to physiotherapist if indicated Annually or as indicated Obesity Weight Annually or as indicated Psychosocial concerns Specific attention to any issues when taking history & during physical examination Annually or as indicated Adapted from Savarirayan et al [2019] Agents/Circumstances to Avoid In individuals with cervical spine instability, extreme neck extension and neck flexion and contact sports should be avoided.
-
Glycine Encephalopathy
Wikipedia
External links [ edit ] Classification D OMIM : 605899 MeSH : D020158 v t e Inborn error of amino acid metabolism K → acetyl-CoA Lysine /straight chain Glutaric acidemia type 1 type 2 Hyperlysinemia Pipecolic acidemia Saccharopinuria Leucine 3-hydroxy-3-methylglutaryl-CoA lyase deficiency 3-Methylcrotonyl-CoA carboxylase deficiency 3-Methylglutaconic aciduria 1 Isovaleric acidemia Maple syrup urine disease Tryptophan Hypertryptophanemia G G→ pyruvate → citrate Glycine D-Glyceric acidemia Glutathione synthetase deficiency Sarcosinemia Glycine → Creatine : GAMT deficiency Glycine encephalopathy G→ glutamate → α-ketoglutarate Histidine Carnosinemia Histidinemia Urocanic aciduria Proline Hyperprolinemia Prolidase deficiency Glutamate / glutamine SSADHD G→ propionyl-CoA → succinyl-CoA Valine Hypervalinemia Isobutyryl-CoA dehydrogenase deficiency Maple syrup urine disease Isoleucine 2-Methylbutyryl-CoA dehydrogenase deficiency Beta-ketothiolase deficiency Maple syrup urine disease Methionine Cystathioninuria Homocystinuria Hypermethioninemia General BC / OA Methylmalonic acidemia Methylmalonyl-CoA mutase deficiency Propionic acidemia G→ fumarate Phenylalanine / tyrosine Phenylketonuria 6-Pyruvoyltetrahydropterin synthase deficiency Tetrahydrobiopterin deficiency Tyrosinemia Alkaptonuria / Ochronosis Tyrosinemia type I Tyrosinemia type II Tyrosinemia type III / Hawkinsinuria Tyrosine → Melanin Albinism : Ocular albinism ( 1 ) Oculocutaneous albinism ( Hermansky–Pudlak syndrome ) Waardenburg syndrome Tyrosine → Norepinephrine Dopamine beta hydroxylase deficiency reverse: Brunner syndrome G→ oxaloacetate Urea cycle / Hyperammonemia ( arginine aspartate ) Argininemia Argininosuccinic aciduria Carbamoyl phosphate synthetase I deficiency Citrullinemia N-Acetylglutamate synthase deficiency Ornithine transcarbamylase deficiency / translocase deficiency Transport / IE of RTT Solute carrier family : Cystinuria Hartnup disease Iminoglycinuria Lysinuric protein intolerance Fanconi syndrome : Oculocerebrorenal syndrome Cystinosis Other 2-Hydroxyglutaric aciduria Aminoacylase 1 deficiency Ethylmalonic encephalopathy Fumarase deficiency Trimethylaminuria

-
Sleep State Misperception
Wikipedia
Philadelphia: WB Saunders, 1994. [ page needed ] External links [ edit ] Classification D ICD - 10 : F51.0 , G47.0 ICD - 9-CM : 307.42 , 307.49 , 780.52 MeSH : D020919 DiseasesDB : 26877 SNOMED CT : 427745001 External resources eMedicine : med/2698 v t e Sleep and sleep disorders Stages of sleep cycles Rapid eye movement (REM) Non-rapid eye movement Slow-wave Brain waves Alpha wave Beta wave Delta wave Gamma wave K-complex Mu rhythm PGO waves Sensorimotor rhythm Sleep spindle Theta wave Sleep disorders Dyssomnia Excessive daytime sleepiness Hypersomnia Insomnia Kleine–Levin syndrome Narcolepsy Night eating syndrome Nocturia Sleep apnea Catathrenia Central hypoventilation syndrome Obesity hypoventilation syndrome Obstructive sleep apnea Periodic breathing Sleep state misperception Circadian rhythm disorders Advanced sleep phase disorder Cyclic alternating pattern Delayed sleep phase disorder Irregular sleep–wake rhythm Jet lag Non-24-hour sleep–wake disorder Shift work sleep disorder Parasomnia Bruxism Nightmare disorder Night terror Periodic limb movement disorder Rapid eye movement sleep behavior disorder Sleepwalking Somniloquy Benign phenomena Dreams Exploding head syndrome Hypnic jerk Hypnagogia / Sleep onset Hypnopompic state Sleep paralysis Sleep inertia Somnolence Nocturnal clitoral tumescence Nocturnal penile tumescence Nocturnal emission Treatment Sleep diary Sleep hygiene Sleep induction Hypnosis Lullaby Somnology Polysomnography Other Sleep medicine Behavioral sleep medicine Sleep study Daily life Bed Bunk bed Daybed Four-poster bed Futon Hammock Mattress Sleeping bag Bed bug Bedding Bedroom Bedtime Bedtime story Bedtime toy Biphasic and polyphasic sleep Chronotype Dream diary Microsleep Mouth breathing Nap Nightwear Power nap Second wind Siesta Sleep and creativity Sleep and learning Sleep deprivation / Sleep debt Sleeping while on duty Sleepover Snoring
-
Muteness
Wikipedia
For example, there is a spectrum of possible neurobehavioural deficits in the posterior fossa syndrome in children following cerebellar tumor surgery. [10] Psychological causes [ edit ] When children do not speak, psychological problems or emotional stress , such as anxiety , may be involved. ... Communication disorders or developmental language delays may occur for several different reasons. [17] [18] Language delays may be associated with other developmental delays. [19] For example, children with Down syndrome often have impaired language and speech. [20] [21] Children with autism, categorized as a neurodevelopmental disorder in the DSM-V, often demonstrate language delays. [22] [23] Recent studies have found that autistic children with language delays are often more able to benefit from treatment services to help build language than was previously believed. [24] Treatment [ edit ] For language delays or communication disorders in children, early assessment is strongly recommended. [25] Language delays may impact expressive language, receptive language, or both. ... "The spectrum of neurobehavioural deficits in the Posterior Fossa Syndrome in children after cerebellar tumour surgery". ... "Language Characteristics of Individuals with Down Syndrome" . Topics in Language Disorders . 29 (2): 112–132. doi : 10.1097/tld.0b013e3181a71fe1 . ... PMID 20428477 . ^ "Speech and Language Resources | National Down Syndrome Congress" . Retrieved 2020-04-19 . ^ Volkers, Nancy (2018).MEF2C, ACTB, TBK1, TBP, TCF4, VCP, SQSTM1, ADAMTS2, SLC9A6, TARDBP, CHMP2B, TREM2, ACTG1, NDUFB11, TMEM106B, PRDM8, EHMT1, SLC19A3, SHANK3, AMER1, CKAP2L, C9orf72, SMARCA2, CHCHD10, PSEN1, PLEC, ATP1A3, COL1A1, COL1A2, COX7B, CSF1R, FGFR1, FTL, FUS, GLE1, GRN, HCCS, HNRNPA1, HNRNPA2B1, KRAS, MAPT, NDUFA6, LINS1, NOS1, NOS2, ZBTB38, RASA2
-
Hepatomegaly
Wikipedia
Depending on the cause, it may sometimes present along with jaundice . [1] Contents 1 Signs and symptoms 2 Causes 2.1 Infective 2.2 Neoplastic 2.3 Biliary 2.4 Metabolic 2.5 Drugs (including alcohol) 2.6 Congenital 2.7 Others 3 Mechanism 4 Diagnosis 4.1 Workup 5 Treatment 6 See also 7 References 8 Further reading 9 External links Signs and symptoms [ edit ] The individual may experience many symptoms, including weight loss, poor appetite and lethargy ( jaundice and bruising may also be present). [1] Causes [ edit ] Leptospirosis Among the causes of hepatomegaly are the following: Infective [ edit ] Glandular fever (Infectious mononucleosis) [1] Hepatitis (A, B or C) [4] Liver abscess (pyogenic abscess) [1] Malaria [1] Amoeba infections [5] Hydatid cyst [6] Leptospirosis [7] Actinomycosis [8] Neoplastic Metastatic tumours [4] Hepatocellular carcinoma [4] Myeloma [1] Leukemia [4] Lymphoma [1] Biliary Primary biliary cirrhosis . [1] Primary sclerosing cholangitis . [1] Metabolic Haemochromatosis [1] Cholesteryl ester storage disease [9] Porphyria [1] Wilson's disease [1] Niemann Pick disease [4] Non-alcoholic fatty liver disease . [1] Glycogen storage disease (GSD) [4] Drugs (including alcohol) Alcohol abuse [4] Drug-induced hepatitis [1] Congenital Hemolytic anemia [1] Polycystic Liver Disease [1] Sickle cell disease [1] Hereditary fructose intolerance [4] Others Hunter syndrome (Spleen affected) [10] Zellweger's syndrome [11] Carnitine palmitoyltransferase I deficiency [12] Granulomatous: Sarcoidosis [13] Mechanism [ edit ] The mechanism of hepatomegaly consists of vascular swelling, inflammation (due to the various causes that are infectious in origin) and deposition of (1) non-hepatic cells or (2) increased cell contents (such due to iron in hemochromatosis or hemosiderosis and fat in fatty liver disease). [14] Diagnosis [ edit ] Abdominal ultrasonography of the liver, as a sagittal plane through the midclavicular line , with some standard measurements. [2] Right lobe of the liver at the midclavicular line at ages 0 to 7. [15] Suspicion of hepatomegaly indicates a thorough medical history and physical examination , wherein the latter typically includes an increased liver span . [ citation needed ] On abdominal ultrasonography , the liver can be measured by the maximum dimension on a sagittal plane view through the midclavicular line , which is normally up to 18 cm in adults. [2] It is also possible to measure the cranio-caudal dimension , which is normally up to 15 cm in adults. [2] This can be measured together with the ventro-dorsal dimension (or depth ), which is normally up to 13 cm. [2] Also, the caudate lobe is enlarged in many diseases. ... Retrieved 2016-03-11 . ^ "Hunter's Syndrome. MPS II information; symptoms | Patient" . ... External links [ edit ] Merck Manual : Hepatomegaly Classification D ICD - 10 : R16..0 ICD - 9-CM : 789.1 MeSH : D006529 External resources MedlinePlus : 003275 Patient UK : Hepatomegaly Scholia has a topic profile for Hepatomegaly . v t e Symptoms and signs relating to the human digestive system or abdomen Gastrointestinal tract Nausea Vomiting Heartburn Aerophagia Pagophagia Dysphagia oropharyngeal esophageal Odynophagia Bad breath Xerostomia Hypersalivation Burping Wet burp Goodsall's rule Chilaiditi syndrome Dance's sign Aaron's sign Arapov's sign Markle sign McBurney's point Sherren's triangle Radiologic signs : Hampton's line Klemm's sign Accessory liver : Councilman body Mallory body biliary: Boas' sign Courvoisier's law Charcot's cholangitis triad / Reynolds' pentad cholecystitis ( Murphy's sign Lépine's sign Mirizzi's syndrome ) Nardi test Defecation Flatulence Fecal incontinence Encopresis Fecal occult blood Rectal tenesmus Constipation Obstructed defecation Diarrhea Rectal discharge Psoas sign Obturator sign Rovsing's sign Hamburger sign Heel tap sign Aure-Rozanova's sign Dunphy sign Alder's sign Lockwood's sign Rosenstein's sign Abdomen Pain Abdominal pain Acute abdomen Colic Baby colic Abdominal guarding Blumberg sign Distension Abdominal distension Bloating Ascites Tympanites Shifting dullness Ascites Fluid wave test Masses Abdominal mass Hepatosplenomegaly Hepatomegaly Splenomegaly Other Jaundice Mallet-Guy sign Puddle sign Ballance's sign Aortic insufficiency Castell's sign Kehr's sign Cullen's sign Grey Turner's sign Hernia Howship–Romberg sign Hannington-Kiff sign Other Cupola sign Fothergill's sign Carnett's sign Sister Mary Joseph nodule v t e Medicine Specialties and subspecialties Surgery Cardiac surgery Cardiothoracic surgery Colorectal surgery Eye surgery General surgery Neurosurgery Oral and maxillofacial surgery Orthopedic surgery Hand surgery Otolaryngology ENT Pediatric surgery Plastic surgery Reproductive surgery Surgical oncology Transplant surgery Trauma surgery Urology Andrology Vascular surgery Internal medicine Allergy / Immunology Angiology Cardiology Endocrinology Gastroenterology Hepatology Geriatrics Hematology Hospital medicine Infectious disease Nephrology Oncology Pulmonology Rheumatology Obstetrics and gynaecology Gynaecology Gynecologic oncology Maternal–fetal medicine Obstetrics Reproductive endocrinology and infertility Urogynecology Diagnostic Radiology Interventional radiology Nuclear medicine Pathology Anatomical Clinical pathology Clinical chemistry Cytopathology Medical microbiology Transfusion medicine Other Addiction medicine Adolescent medicine Anesthesiology Dermatology Disaster medicine Diving medicine Emergency medicine Mass gathering medicine Family medicine General practice Hospital medicine Intensive care medicine Medical genetics Narcology Neurology Clinical neurophysiology Occupational medicine Ophthalmology Oral medicine Pain management Palliative care Pediatrics Neonatology Physical medicine and rehabilitation PM&R Preventive medicine Psychiatry Addiction psychiatry Radiation oncology Reproductive medicine Sexual medicine Sleep medicine Sports medicine Transplantation medicine Tropical medicine Travel medicine Venereology Medical education Medical school Bachelor of Medicine, Bachelor of Surgery Bachelor of Medical Sciences Master of Medicine Master of Surgery Doctor of Medicine Doctor of Osteopathic Medicine MD–PhD Related topics Alternative medicine Allied health Dentistry Podiatry Pharmacy Physiotherapy Molecular oncology Nanomedicine Personalized medicine Public health Rural health Therapy Traditional medicine Veterinary medicine Physician Chief physician History of medicine Book Category Commons Wikiproject Portal OutlineTRIM37, TGFB1, ADAMTSL2, PEPD, SLC29A3, CYBA, A1BG, NOS2, NOS3, ADAM3A, CYP1B1, CYP1A2, CYP1A1, ABCC3, DSCAM, MAPK14, CRYGD, COPS3, KLF11, NR1H2, CYGB, NFE2L2, ATG5, NR1I2, HNF1A, LEP, LEPR, DAPK2, IGKC, MLC1, AKR7A3, HMGCS2, HDC, MYO1B, ADAMTS5, NR1H4, NR1I3, NR5A2, KEAP1, FGF12, GALNT13, SESN2, CABCOCO1, RELA, MIR192, GPR155, ALB, SBSPON, ACOT1, PRSS35, PPARA, AHR, ALDH1B1, MBOAT2, CAMK2A, STAC3, KRT6C, SGSH, MRPL3, PLPBP, KCNQ1OT1, SEC63, TERC, KLF1, SCO1, AGPAT2, RNASEH2A, HYOU1, COG5, TCIRG1, CD96, SLC25A15, SLC25A13, RASGRP1, TSFM, NPC2, CLCA4, POLG2, USP18, BSCL2, SLC17A5, TINF2, IFT172, RPL5, NDUFAF3, RRAS, AMACR, KAT6B, TNFRSF13B, SF3B1, SAA1, RPGRIP1L, VPS13A, FASTKD2, NLRP1, DOLK, MRAS, SC5D, SKIV2L, VPS45, GNE, SLC20A2, SLC2A1, ABCC8, TNFRSF11A, AKR1D1, STX11, ABCB11, TNFSF11, SRP54, AP3B1, PEX3, STX1A, LZTR1, MOGS, MFN2, ALMS1, ZAP70, XRCC4, WT1, UQCRB, TALDO1, UCP2, TUFM, TNFRSF1B, TCF4, SPTB, SPTA1, SOX10, PEX11B, PLEKHM1, SLC4A1, TERT, IFT140, SLCO2A1, LPIN2, TTC37, SLC22A5, EIF2AK3, CYP7B1, PEX16, XPR1, CLDN1, SLC7A7, AP3D1, SMPD1, SOS1, DPM2, DPM1, SOS2, GNMT, NPHP3, LARS1, BBS9, NLRP3, PIGS, PIGM, G6PC3, COG7, NDUFAF2, RFT1, ATPAF2, TMEM67, GFM1, LRRCC1, ALG2, COX14, COX4I2, C15orf41, COA8, CCDC115, ANTXR1, MAGT1, ITCH, FERMT3, JAM3, HSD3B7, NUBPL, CTC1, DHDDS, ALG13, ALG9, FDX2, TNFRSF13C, OSTM1, COX20, OCLN, RNU4ATAC, PET100, NCF1, BOLA3, DIPK1A, FAM111B, NHLRC2, NDUFS7, GPIHBP1, MMAB, SUMF1, CAVIN1, SLC13A5, NEK8, H19, UNC13D, GLIS3, MMAA, NAGS, HJV, LACC1, A2ML1, HGSNAT, DNAJC21, DIS3L2, NDUFA11, RHBDF2, USB1, EFL1, CYBC1, FOXRED1, SLC30A10, NOP10, STEAP3, WRAP53, AGGF1, TMEM70, TET2, NDUFB11, ADA2, RTEL1, MPC1, PTRH2, DYNC2LI1, RIT1, DCDC2, TIMMDC1, GLRX5, TACO1, DCTN4, SBDS, NDUFAF1, ABHD5, MRPS7, SNX10, ICOS, NDUFAF4, SLC39A4, CHD7, NHP2, CC2D2A, GNPTAB, NDUFAF5, ALG8, DDRGK1, VPS33A, DCLRE1C, XYLT1, CIDEC, TRAPPC11, SLC25A19, NLRC4, HAMP, WDR35, PEX26, MYORG, SCYL1, PNPLA2, HYMAI, INPP5E, BTNL2, ALG1, TMEM126B, TMEM165, NGLY1, IFT122, TRMU, RMRP, PTPN11, RHAG, GBA, GALT, GALNS, GALE, GAA, SLC37A4, G6PC, FUCA1, FOS, FGA, GPC4, FBP1, FAH, F5, EWSR1, ETFDH, ETFB, ETFA, ERCC6, ERBB3, EPB42, DNASE1L3, DLD, DKC1, DHFR, DGUOK, DAXX, CD55, GATA2, GCDH, CTSK, GPC3, IL1RN, IGF2, SP110, IDUA, IDS, HSD17B4, HPGD, HNF4A, HMOX1, HMGCL, HLA-DRB1, HFE, HEXA, HBG2, HBG1, HBB, HBA2, HBA1, HADHA, H3-3A, GUCY2D, GUSB, GPR35, GPD1, GPC1, GNS, GLB1, CYBB, CTNNB1, RASA2, BMP2, AUH, ATRX, ATP7B, ATP6AP1, ATP6V1B2, ALDH7A1, ASS1, ASL, ASAH1, ARSB, FASLG, FAS, APOE, APOC2, APOA1, XIAP, ANK1, ALDOB, AKT2, AGL, AGA, ADA, ACOX1, ACAT1, ACADVL, ACADM, ACADL, B2M, BRAF, CTNS, BTD, CTLA4, CR2, CPT2, CPT1A, CPOX, COX10, COX8A, COX6B1, ABCC2, CLCN7, ERCC8, LYST, CFTR, CDKN1C, CD70, CD40LG, SCARB2, CD28, CD27, CD19, CBS, CAV1, CASR, CASP10, CALR, SLC25A20, CA2, IL2RA, IL2RB, IL2RG, ABCB4, PEX14, PEX13, PEX12, PEX10, PEX6, PEX1, PDGFRB, PDGFRA, PDGFB, PCK1, PCCB, PCCA, PC, PARN, NRAS, NPC1, NOTCH2, NEU1, NDUFV2, NDUFS8, NDUFS6, NDUFS4, NDUFV1, NDUFS3, NDUFS2, NDUFS1, NDUFB10, ATP8B1, PHKA2, NDUFB3, PHKB, RAG2, RAG1, RAF1, RAB27A, PYGL, PEX5, PEX2, ABCD3, PEX19, PTPRC, ABCA1, PSMB9, PSMB8, PSMB4, PSAP, PRKCSH, PRKCD, PRF1, PPARG, POLG, POLD1, PMM2, PLAGL1, PKHD1, PIK3C2A, SERPINA1, PHKG2, NDUFB9, NDUFA6, IL6, NDUFA1, MECP2, MCM4, MARS1, MAN2B1, LYZ, SH2D1A, LTBP3, LRP5, LMNA, LIPE, LIPA, LIG4, LCAT, LBR, KRT17, KRT16, KRT6B, KRT6A, KRAS, KCNQ1, KCNN4, KCNJ11, KCNH1, JAK2, ITK, INPPL1, IL7R, MEFV, MET, MIF, MPI, NCF4, NCF2, NAGLU, NAGA, MYD88, MYBPC3, MVK, MMUT, TRNW, TRNV, TRNS1, TRNN, TRNL1, TRNK, TRNE, ND6, ND5, ND4, ND3, ND2, ND1, ATP6, MST1, MPV17, MPL, H19-ICR, EHHADH, LTBR

-
Epilepsy In Children
Wikipedia
Contents 1 Presentation 1.1 Education 1.2 Social 1.3 Language 2 Causes 3 Treatment 4 See also 5 References Presentation [ edit ] Diagnosis In 2014 the International League Against Epilepsy (ILAE) Task Force proposed the operational (practical) clinical definition of epilepsy, intended as a disease of the brain defined by any of the following conditions: [2] At least two unprovoked (or reflex) seizures occurring >24 h apart. [2] One unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years. [2] Diagnosis of an epilepsy syndrome. [2] It is important that as soon as someone is diagnosed with SE, they immediately get medical treatment that usually involves the use of medication. ... The New Yorker . v t e Seizures and epilepsy Basics Seizure types Aura (warning sign) Postictal state Epileptogenesis Neonatal seizure Epilepsy in children Management Anticonvulsants Investigations Electroencephalography Epileptologist Personal issues Epilepsy and driving Epilepsy and employment Seizure types Focal Seizures Simple partial Complex partial Gelastic seizure Epilepsy Temporal lobe epilepsy Frontal lobe epilepsy Rolandic epilepsy Nocturnal epilepsy Panayiotopoulos syndrome Vertiginous epilepsy Generalised Tonic–clonic Absence seizure Atonic seizure Automatism Benign familial neonatal seizures Lennox–Gastaut syndrome Myoclonic astatic epilepsy Epileptic spasms Status epilepticus Epilepsia partialis continua Complex partial status epilepticus Myoclonic epilepsy Progressive myoclonus epilepsy Dentatorubral–pallidoluysian atrophy Unverricht–Lundborg disease MERRF syndrome Lafora disease Juvenile myoclonic epilepsy Non-epileptic seizure Febrile seizure Psychogenic non-epileptic seizure Related disorders Sudden unexpected death in epilepsy Todd's paresis Landau–Kleffner syndrome Epilepsy in animals Organizations Citizens United for Research in Epilepsy (US) Epilepsy Action (UK) Epilepsy Action Australia Epilepsy Foundation (US) Epilepsy Outlook (UK) Epilepsy Research UK Epilepsy Society (UK)
-
Paraphrenia
Wikipedia
Paraphrenia Other names Paraphrenic syndrome Specialty Psychiatry Paraphrenia is a mental disorder characterized by an organized system of paranoid delusions with or without hallucinations (the positive symptoms of schizophrenia) and without deterioration of intellect or personality (its negative symptom ). [1] [2] [3] This disorder is also distinguished from schizophrenia by a lower hereditary occurrence, less premorbid maladjustment, and a slower rate of progression. [4] Onset of symptoms generally occurs later in life, near the age of 60. [2] [5] The prevalence of the disorder among the elderly is between 0.1% and 4%. [1] Paraphrenia is not included in the DSM-5 ; psychiatrists often diagnose patients presenting with paraphrenia as having atypical psychoses, delusional disorder , psychoses not otherwise specified, schizoaffective disorders , and persistent persecutory states of older adults. [4] Recently, mental health professionals have also been classifying paraphrenia as very late-onset schizophrenia-like psychosis. [4] In the Russian psychiatric manuals, paraphrenia (or paraphrenic syndrome) is the last stage of development of paranoid schizophrenia . ... Late paraphrenia: A variant of schizophrenia manifest in late life or an organic clinical syndrome? A review of recent evidence. International Journal of Geriatric Psychiatry, 13 , 775-784 ^ a b c d e f g h i j k l m n Casanova, M. ... Late paraphrenia: A variant of schizophrenia manifest in late life or an organic clinical syndrome? A review of recent evidence. International Journal of Geriatric Psychiatry, 13, 775-784 ^ a b Berrios G E (2003) A Conceptual History of Paraphrenia. Journal of Nutrition, Health and Aging 7: 394-399 ^ a b c McKenna, P.J. (1997). Schizophrenia and related syndromes . Psychology Press. pp. 239 –242.
-
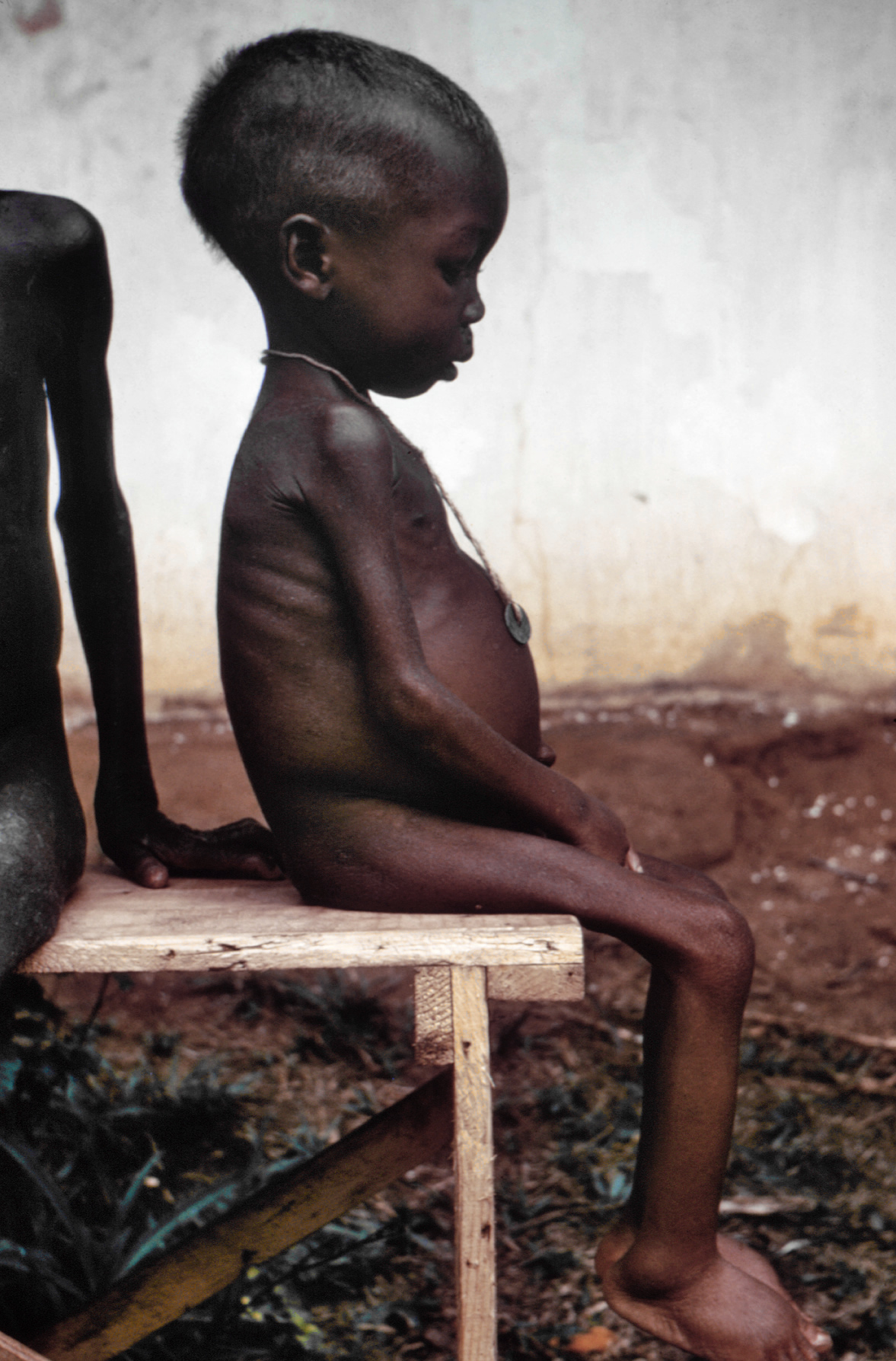
Kwashiorkor
Wikipedia
In dry climates, marasmus is the more frequent disease associated with malnutrition. Another malnutrition syndrome includes cachexia , although it is often caused by underlying illnesses. ... A case was described where parents who fed their child cassava failed to recognize malnutrition because of the edema caused by the syndrome and believed the child was well-nourished despite the lack of dietary protein. [18] Protein should be supplied only for anabolic purposes. ... WHO criteria for clinical assessment of malnutrition are based on the degree of wasting (MUAC), stunting (weight-for-height Z-score), and the presence of edema (mild to severe). [24] Prevention [ edit ] In order to avoid refeeding syndrome , the person must be rehabilitated with small but frequent rations, given every two to four hours. ... External links [ edit ] Media related to Kwashiorkor at Wikimedia Commons Classification D ICD - 10 : E40 MeSH : D007732 v t e Malnutrition Protein-energy malnutrition Kwashiorkor Marasmus Catabolysis Vitamin deficiency B vitamins B 1 Beriberi Wernicke–Korsakoff syndrome Wernicke's encephalopathy Korsakoff's syndrome B 2 Riboflavin deficiency B 3 Pellagra B 6 Pyridoxine deficiency B 7 Biotin deficiency B 9 Folate deficiency B 12 Vitamin B 12 deficiency Other A: Vitamin A deficiency Bitot's spots C: Scurvy D: Vitamin D deficiency Rickets Osteomalacia Harrison's groove E: Vitamin E deficiency K: Vitamin K deficiency Mineral deficiency Sodium Potassium Magnesium Calcium Iron Zinc Manganese Copper Iodine Chromium Molybdenum Selenium Keshan disease Growth Delayed milestone Failure to thrive Short stature Idiopathic General Anorexia Weight loss Cachexia UnderweightIGF1, ALB, IL6, RPTOR, AGO2, TTR, STAT3, SLC6A6, SHBG, MOG, IL2, AQP5, HIF1A, GH1, MTOR, DAB2, CSF3R, CAT, ACE2