., either not painful or painful, respectively) (see post-vasectomy pain syndrome ). The vast majority of sperm granulomas in vasectomized men are present as a result of the pressure-induced changes of vasectomy . [2] References [ edit ] ^ McDonald S.
She had normal intelligence, although she had had some learning difficulties, and did not have the dysmorphic features usually associated with the 18q- syndrome. By molecular methods, Kamholz et al. (1988) demonstrated that the deletion included the myelin basic protein gene (159430) but did not include the transthyretin gene (176300).
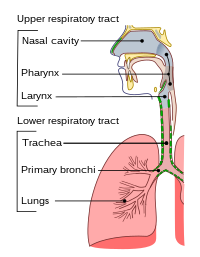
In many instances, tracheobronchial abnormalities are part of a syndrome. Wong et al. (1998) described monozygotic twin girls concordant for congenital tracheobronchial stenosis.
A rare malformation characterized by fixed narrowing of the tracheal lumen primarily due to complete tracheal cartilage rings and an absent membranous trachea, which causes breathing difficulty.
An EMG test reveals loss of the nerve supply, or denervation, in the affected limb without a conduction block (a nerve blockage restricted to a small segment of the nerve). [ citation needed ] In early stages of the disease MMA may be confused for amyotrophic lateral sclerosis (ALS), cervical spondylotic amyotrophy (CSA), and other challenging neurological diseases, as well as conditions that are minor but that call for very different treatments, such as advanced carpal tunnel syndrome (CTS). Symptoms somewhat differ. [15] [3] Pain and tingling in the hand is typically present in CTS and absent from MMA; loss of function presents differently; with careful electrophysiological study and neurological exams the two are distinguished. ... There is also a slowly progressive variant of MMA known as O'Sullivan-McLeod syndrome, which only affects the small muscles of the hand and forearm and has a slowly progressive course. [19] Epidemiology [ edit ] MMA is described most frequently in Asia, with studies of a few hundred individuals emerging from Japan, China and India; it is much less commonly seen in North America and Europe. ... "Hirayama disease (monomelic amyotrophy) clinically confused for carpal tunnel syndrome" . Neuropsychiatric Disease and Treatment . 2017:13: 1385–1388. doi : 10.2147/NDT.S138315 . ... PMID 24286527 . ^ Ghadiri-Sani, M; Huda, S; Larner, AJ (December 2014). "O'Sullivan-McLeod syndrome: clinical features, neuroradiology and nosology". ... External links [ edit ] Classification D ICD - 10 : G71.8 OMIM : 602440 MeSH : C538253 External resources Orphanet : 65684 monomelic_amyotrophy at NINDS v t e Diseases of the nervous system , primarily CNS Inflammation Brain Encephalitis Viral encephalitis Herpesviral encephalitis Limbic encephalitis Encephalitis lethargica Cavernous sinus thrombosis Brain abscess Amoebic Brain and spinal cord Encephalomyelitis Acute disseminated Meningitis Meningoencephalitis Brain / encephalopathy Degenerative Extrapyramidal and movement disorders Basal ganglia disease Parkinsonism PD Postencephalitic NMS PKAN Tauopathy PSP Striatonigral degeneration Hemiballismus HD OA Dyskinesia Dystonia Status dystonicus Spasmodic torticollis Meige's Blepharospasm Athetosis Chorea Choreoathetosis Myoclonus Myoclonic epilepsy Akathisia Tremor Essential tremor Intention tremor Restless legs Stiff-person Dementia Tauopathy Alzheimer's Early-onset Primary progressive aphasia Frontotemporal dementia / Frontotemporal lobar degeneration Pick's Dementia with Lewy bodies Posterior cortical atrophy Vascular dementia Mitochondrial disease Leigh syndrome Demyelinating Autoimmune Inflammatory Multiple sclerosis For more detailed coverage, see Template:Demyelinating diseases of CNS Episodic/ paroxysmal Seizures and epilepsy Focal Generalised Status epilepticus For more detailed coverage, see Template:Epilepsy Headache Migraine Cluster Tension For more detailed coverage, see Template:Headache Cerebrovascular TIA Stroke For more detailed coverage, see Template:Cerebrovascular diseases Other Sleep disorders For more detailed coverage, see Template:Sleep CSF Intracranial hypertension Hydrocephalus Normal pressure hydrocephalus Choroid plexus papilloma Idiopathic intracranial hypertension Cerebral edema Intracranial hypotension Other Brain herniation Reye syndrome Hepatic encephalopathy Toxic encephalopathy Hashimoto's encephalopathy Both/either Degenerative SA Friedreich's ataxia Ataxia–telangiectasia MND UMN only: Primary lateral sclerosis Pseudobulbar palsy Hereditary spastic paraplegia LMN only: Distal hereditary motor neuronopathies Spinal muscular atrophies SMA SMAX1 SMAX2 DSMA1 Congenital DSMA Spinal muscular atrophy with lower extremity predominance (SMALED) SMALED1 SMALED2A SMALED2B SMA-PCH SMA-PME Progressive muscular atrophy Progressive bulbar palsy Fazio–Londe Infantile progressive bulbar palsy both: Amyotrophic lateral sclerosis
Although there was a history of DTP vaccination in both patients, Gucuyener et al. (1991) pointed out that in their patients, the clinical course was not compatible with neuralgic amyotrophy. Delayed post-poliomyelitis syndrome, which begins many years after recovery from acute paralytic poliomyelitis, was considered unlikely because the patients had been vaccinated for polio and had no history of poliomyelitis during infancy, and also because of their young ages.
Additional rare manifestations include worsening of symptoms with exposure to cold (cold paresis), muscle cramps, cold hands, irregular coarse tremor and/or contraction fasciculations. O'Sullivan-McLeod syndrome (see this term), considered to be a variant of MA, presents with weakness in the intrinsic hand muscles.
Monomelic amyotrophy (MMA) is a rare disease that causes muscle weakness in the upper extremities. MMA affects the lower motor neurons. Lower motor neurons are cells that help communicate information from the brain to the muscles that are involved in movement ( skeletal muscles ). Specifically, monomelic amyotrophy causes weakness and loss of muscle mass in the arms and fingers. Symptoms of the disease typically begin between the ages of 14-25 years-old. The disease is most common in Asia, especially in Japan and India. Males are more likely to develop the disease than females.
Herpetic proctitis (inflammation of the anus and rectum) is common for individuals participating in anal intercourse . [8] After 2–3 weeks, existing lesions progress into ulcers and then crust and heal, although lesions on mucosal surfaces may never form crusts. [8] In rare cases, involvement of the sacral region of the spinal cord can cause acute urinary retention and one-sided symptoms and signs of myeloradiculitis (a combination of myelitis and radiculitis ): pain, sensory loss, abnormal sensations ( paresthesia ) and rash. [9] [10] Historically, this has been termed Elsberg syndrome, although this entity is not clearly defined. [9] Recurrence After a first episode of herpes genitalis caused by HSV-2 , there will be at least one recurrence in approximately 80% of people, while the recurrence rate for herpes genitalis caused by HSV-1 is approximately 50%. [11] Herpes genitalis caused by HSV-2 recurs on average four to six times per year, while that of HSV-1 infection occurs only about once per year. [11] People with recurrent genital herpes may be treated with suppressive therapy , which consists of daily antiviral treatment using acyclovir, valacyclovir or famciclovir. [12] Suppressive therapy may be useful in those who have at least four recurrences per year but the quality of the evidence is poor. [12] People with lower rates of recurrence will probably also have fewer recurrences with suppressive therapy. [13] Suppressive therapy should be discontinued after a maximum of one year to reassess recurrence frequency. [13] Transmission Genital herpes can be spread by viral shedding prior to and following the formation of ulcers. ... S2CID 24474530 . ^ Vonk P (December 1993). "[Elsberg syndrome: acute urinary retention following a viral infection]". ... External links Classification D ICD - 10 : A60 ICD - 9-CM : 054.1 MeSH : D006558 External resources MedlinePlus : 000857 v t e Skin infections , symptoms and signs related to viruses DNA virus Herpesviridae Alpha HSV Herpes simplex Herpetic whitlow Herpes gladiatorum Herpes simplex keratitis Herpetic sycosis Neonatal herpes simplex Herpes genitalis Herpes labialis Eczema herpeticum Herpetiform esophagitis Herpes B virus B virus infection VZV Chickenpox Herpes zoster Herpes zoster oticus Ophthalmic zoster Disseminated herpes zoster Zoster-associated pain Modified varicella-like syndrome Beta Human herpesvirus 6 / Roseolovirus Exanthema subitum Roseola vaccinia Cytomegalic inclusion disease Gamma KSHV Kaposi's sarcoma Poxviridae Ortho Variola Smallpox Alastrim MoxV Monkeypox CPXV Cowpox VV Vaccinia Generalized vaccinia Eczema vaccinatum Progressive vaccinia Buffalopox Para Farmyard pox : Milker's nodule Bovine papular stomatitis Pseudocowpox Orf Sealpox Other Yatapoxvirus : Tanapox Yaba monkey tumor virus MCV Molluscum contagiosum Papillomaviridae HPV Wart / plantar wart Heck's disease Genital wart giant Laryngeal papillomatosis Butcher's wart Bowenoid papulosis Epidermodysplasia verruciformis Verruca plana Pigmented wart Verrucae palmares et plantares BPV Equine sarcoid Parvoviridae Parvovirus B19 Erythema infectiosum Reticulocytopenia Papular purpuric gloves and socks syndrome Polyomaviridae Merkel cell polyomavirus Merkel cell carcinoma RNA virus Paramyxoviridae MeV Measles Togaviridae Rubella virus Rubella Congenital rubella syndrome ("German measles" ) Alphavirus infection Chikungunya fever Picornaviridae CAV Hand, foot, and mouth disease Herpangina FMDV Foot-and-mouth disease Boston exanthem disease Ungrouped Asymmetric periflexural exanthem of childhood Post-vaccination follicular eruption Lipschütz ulcer Eruptive pseudoangiomatosis Viral-associated trichodysplasia Gianotti–Crosti syndrome v t e Sexually transmitted infections (STI) Bacterial Chancroid ( Haemophilus ducreyi ) Chlamydia , lymphogranuloma venereum ( Chlamydia trachomatis ) Donovanosis ( Klebsiella granulomatis ) Gonorrhea ( Neisseria gonorrhoeae ) Mycoplasma hominis infection ( Mycoplasma hominis ) Syphilis ( Treponema pallidum ) Ureaplasma infection ( Ureaplasma urealyticum ) Protozoal Trichomoniasis ( Trichomonas vaginalis ) Parasitic Crab louse Scabies Viral AIDS ( HIV-1/HIV-2 ) Cancer cervical vulvar penile anal Human papillomavirus (HPV) Genital warts ( condyloma ) Hepatitis B ( Hepatitis B virus ) Herpes simplex HSV-1 & HSV-2 Molluscum contagiosum ( MCV ) General inflammation female Cervicitis Pelvic inflammatory disease (PID) male Epididymitis Prostatitis either Proctitis Urethritis / Non-gonococcal urethritis (NGU)
Overview Genital herpes is a common sexually transmitted infection (STI). The herpes simplex virus (HSV) causes genital herpes. Genital herpes can often be spread by skin-to-skin contact during sexual activity. Some people infected with the virus may have very mild symptoms or no symptoms. They can still able to spread the virus. Other people have pain, itching and sores around the genitals, anus or mouth. There is no cure for genital herpes. Symptoms often show up again after the first outbreak.
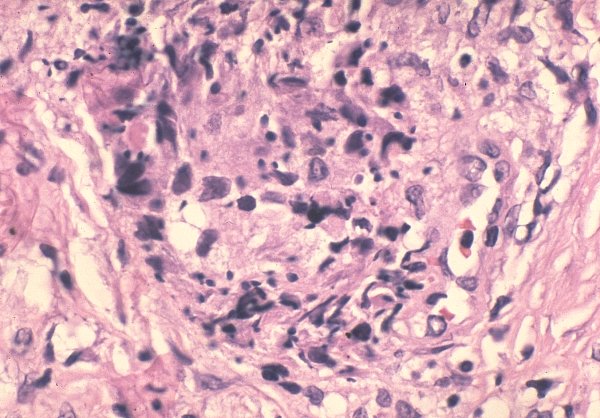
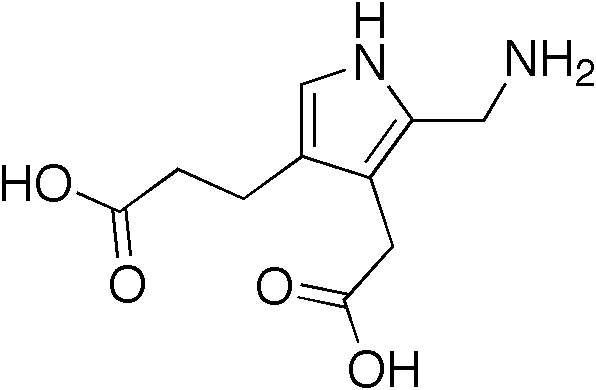
The patients are typically asymptomatic, with most gene carriers having no family history because the condition had remained latent for several generations. The syndrome marked by acute attacks affects only 10% of gene carriers. [4] The mean age at diagnosis is 33 years old. [5] Like other porphyrias, AIP is more likely to present in women. [6] A distinguishing feature of AIP that separates it from other porphyrias is the absence of photosensitive cutaneous symptoms that occur in addition to acute attacks. [7] Acute attacks [ edit ] AIP is one of the four porphyrias that presents as an acute attack. 90% of affected individuals never experience an acute attack and are asymptomatic, while an estimated 5% of affected individuals experience repeat attacks. [8] Attacks are most common in young adult women and are rare before puberty or after menopause. [9] Severe acute attacks may require hospitalization. ... External links [ edit ] Classification D ICD - 10 : E80.2 ICD - 9-CM : 277.1 OMIM : 176000 MeSH : D017118 DiseasesDB : 171 External resources eMedicine : med/1880 GeneReviews : Hydroxymethylbilane Synthase (HMBS) Deficiency v t e Heme metabolism disorders Porphyria , hepatic and erythropoietic ( porphyrin ) early mitochondrial: ALAD porphyria Acute intermittent porphyria cytoplasmic: Gunther disease/congenital erythropoietic porphyria Porphyria cutanea tarda / Hepatoerythropoietic porphyria late mitochondrial: Hereditary coproporphyria Harderoporphyria Variegate porphyria Erythropoietic protoporphyria Hereditary hyperbilirubinemia ( bilirubin ) unconjugated: Gilbert's syndrome Crigler–Najjar syndrome Lucey–Driscoll syndrome conjugated: Dubin–Johnson syndrome nd sheet Rotor syndrome
The cause of hyponatremia is not clear; both SIADH (syndrome of inappropriate antidiuretic hormone release) and renal salt wasting have been proposed as mechanisms. ... The main finding is posterior reversible encephalopathy syndrome [Pischik & Kauppinen 2009]. Twenty-two individuals with AIP presenting with posterior reversible encephalopathy syndrome were investigated with MRI imaging [Zheng et al 2018]; 95% of these presented with seizures that may be related to hyponatremia.
Acute intermittent porphyria (AIP) is one of the liver (hepatic) porphyrias . AIP is caused by low levels of porphobilinogen deaminase (PBGD), an enzyme also often called hydroxymethylbilane synthase. The low levels of PBGD are generally not sufficient to cause symptoms; however, activating factors such as hormones, drugs, and dietary changes may trigger symptoms. Although most individuals with AIP never develop symptoms, symptomatic individuals typically present with abdominal pain with nausea. Treatment is dependent on the symptoms.
A rare, severe form of the acute hepatic porphyrias characterized by the occurrence of neuro-visceral attacks without cutaneous manifestations. Clinical description Patients suffer intermittent neuro-visceral attacks that can persist for several days and that repeat over several weeks. These attacks manifest as intense abdominal pain (>95% of cases) and neurological and/or psychological symptoms. The abdominal pain is often associated with lumbago irradiating to the thighs, and with nausea, vomiting and relentless constipation. Psychological symptoms are variable: irritability, emotionality, depression, considerable anxiety and, more rarely, auditory and visual hallucinations, disorientation, mental confusion.
Nomenclature WDR26 -related intellectual disability has also been referred to as Skraban-Deardorff syndrome. Prevalence WDR26 -related intellectual disability is rare. ... Differential Diagnosis Developmental delay with delayed speech and febrile and/or non-febrile seizures, the most frequent features of WDR26 -related ID, are relatively common and have an extensive differential diagnosis. The following syndromes with significant phenotypic overlap with WDR26 -related ID have been considered in some affected individuals before the diagnosis of WDR26 -related ID was established (Table 2). ... Disorders with Developmental Delay / Intellectual Disability to Consider in the Differential Diagnosis of WDR26 -Related Intellectual Disability View in own window Differential Diagnosis Disorder Gene / Genetic Mechanism MOI Clinical Features of the Differential Diagnosis Disorder Overlapping w/ WDR26 -related ID Distinguishing from WDR26 -related ID Angelman syndrome Deficient expression/ function of maternally inherited UBE3A allele See footnote 1 Happy demeanor Seizures Abnormal gait Widely spaced teeth Inappropriate laughter/excitability Microcephaly common Pitt-Hopkins syndrome TCF4 or deletion of the chromosome region in which TCF4 is located See footnote 2 Seizures Widely spaced teeth Full lips Episodic hyperventilation &/or breath-holding spells Severe myopia Alpha-thalassemia X-linked intellectual disability syndrome ATRX XL Hypotonia Coarse facial features Alpha-thalassemia & HbH inclusion bodies Genital anomalies Microcephaly common Postnatal growth deficiency Kleefstra syndrome EHMT1 or deletion at 9q34.3 AD Seizures Hypotonia Autistic features Congenital malformations more common Severe infections AD = autosomal dominant; ID = intellectual disability; MOI = mode of inheritance; XL = X-linked 1. The risk to sibs of a proband depends on the genetic mechanism leading to the loss of UBE3A function: typically less than 1% risk for probands with a deletion or uniparental disomy, and as high as 50% for probands with an imprinting defect or a pathogenic variant of UBE3A . 2. Pitt-Hopkins syndrome is caused by haploinsufficiency of TCF4 .
Overview Pityriasis rosea is a rash that often begins as an oval spot on the face, chest, abdomen or back. This is called a herald patch and may be up to 4 inches (10 centimeters) across. Then you may get smaller spots that sweep out from the middle of the body in a shape that looks like drooping pine-tree branches. The rash can be itchy. Pityriasis (pit-ih-RIE-uh-sis) rosea can happen at any age but is most common between the ages of 10 and 35. It tends to go away on its own within 10 weeks. Treatment may help relieve the symptoms.
Contents 1 Presentation 1.1 Complications 1.1.1 Late effects 2 Cause 3 Diagnosis 4 Treatment 4.1 Management of fetal SCTs 4.2 Management of adult SCTs 5 See also 6 References 7 External links Presentation [ edit ] Complications [ edit ] Maternal complications of pregnancy may include mirror syndrome . [1] Maternal complications of delivery may include a Cesarean section or, alternatively, a vaginal delivery with mechanical dystocia . [2] Complications of the mass effect of a teratoma in general are addressed on the teratoma page. ... An often used decision tree is as follows: Perform detailed ultrasound exam including fetal echocardiogram and Doppler flow analysis If fetal high output failure , placentomegaly , or hydrops If fetus not mature, perform pregnancy termination or fetal intervention Else fetus mature, perform emergency Cesarean section Else no emergent problems, perform serial non-stress tests and ultrasound biophysical profiles and plan delivery, as follows If emergent problems develop, return to top of decision tree Else if SCT over 5–10 cm or polyhydramnios , perform early (37 weeks gestation) elective Cesarean section Else SCT small and no complications, permit term spontaneous vaginal delivery Emergent problems include maternal mirror syndrome , polyhydramnios , and preterm labor . ... There are case reports of good outcomes. [27] See also [ edit ] Currarino syndrome Teratoma Sacrococcygeal symphysis References [ edit ] ^ Finamore PS, Kontopoulos E, Price M, Giannina G, Smulian JC (2007). "Mirror syndrome associated with sacrococcygeal teratoma: a case report". ... External links [ edit ] Classification D External resources eMedicine : med/2248 v t e Overview of tumors , cancer and oncology Conditions Benign tumors Hyperplasia Cyst Pseudocyst Hamartoma Malignant progression Dysplasia Carcinoma in situ Cancer Metastasis Primary tumor Sentinel lymph node Topography Head and neck ( oral , nasopharyngeal ) Digestive system Respiratory system Bone Skin Blood Urogenital Nervous system Endocrine system Histology Carcinoma Sarcoma Blastoma Papilloma Adenoma Other Precancerous condition Paraneoplastic syndrome Staging / grading TNM Ann Arbor Prostate cancer staging Gleason grading system Dukes classification Carcinogenesis Cancer cell Carcinogen Tumor suppressor genes / oncogenes Clonally transmissible cancer Oncovirus Carcinogenic bacteria Misc.
A sacrococcygeal teratoma is a tumor that grows at the base of the spine in a developing fetus. It occurs in one in 40,000 newborns and girls are four times more likely to be affected than boys. Though it is usually benign , there is a possibility that the teratoma could become malignant . As such, the recommended treatment of a teratoma is complete removal of the tumor by surgery, performed soon after the birth. If not all of the tumor is removed during the initial surgery, the teratoma may grow back ( recur ) and additional surgeries may be needed.
Please consider expanding the lead to provide an accessible overview of all important aspects of the article. ( March 2020 ) Central nervous system disease Central nervous system in yellow ( brain and spinal cord ) Specialty Psychiatry , Neurology , Neurosurgery Central nervous system diseases , also known as central nervous system disorders , are a group of neurological disorders that affect the structure or function of the brain or spinal cord , which collectively form the central nervous system (CNS). [1] [2] [3] Contents 1 Signs and symptoms 2 Causes 2.1 Trauma 2.2 Infections 2.3 Degeneration 2.4 Structural defects 2.5 CNS Tumors 2.6 Autoimmune disorders 2.7 Stroke 3 Functions 3.1 Spinal cord 3.2 Brain 4 Diagnosis 4.1 Types of CNS disorders 4.1.1 Addiction 4.1.2 Arachnoid cysts 4.1.3 Attention deficit/hyperactivity disorder (ADHD) 4.1.4 Autism 4.1.5 Bipolar disorder 4.1.6 Catalepsy 4.1.7 Depression 4.1.8 Encephalitis 4.1.9 Epilepsy/Seizures 4.1.10 Infection 4.1.11 Locked-in syndrome 4.1.12 Meningitis 4.1.13 Migraine 4.1.14 Multiple sclerosis 4.1.15 Myelopathy 4.1.16 Neurodegenerative disorders 4.1.16.1 Alzheimer’s 4.1.16.2 Huntington's disease 4.1.16.3 Parkinson's 4.1.17 Tourette's 5 Treatments 6 See also 7 References 8 External links Signs and symptoms [ edit ] Every disease has different signs and symptoms . ... A number of different pathogens (i.e., certain viruses , bacteria , protozoa , fungi , and prions ) can cause infections that adversely affect the brain or spinal cord. Locked-in syndrome [ edit ] A medical condition, Locked-in syndrome usually resulting from a stroke that damages part of the brainstem, in which the body and most of the facial muscles are paralysed but consciousness remains and the ability to perform certain eye movements is preserved. ... Parkinson's disease , Attention deficit/hyperactivity disorder (ADHD) and Bi-polar disorder , all appear to have some connection to one another, as all three nervous system disorders involve lower than normal levels of the brain chemical dopamine (In ADHD, Parkinson's, and the depressive phase of Bi-polar disorder.) or too much dopamine (in Mania or Manic states of Bi-polar disorder ) in different areas of the brain: [27] [32] [33] [34] Tourette's [ edit ] Main article: Tourette's syndrome Tourette's syndrome is an inherited neurological disorder. ... External links [ edit ] Classification D MeSH : D002493 v t e Diseases of the nervous system , primarily CNS Inflammation Brain Encephalitis Viral encephalitis Herpesviral encephalitis Limbic encephalitis Encephalitis lethargica Cavernous sinus thrombosis Brain abscess Amoebic Brain and spinal cord Encephalomyelitis Acute disseminated Meningitis Meningoencephalitis Brain / encephalopathy Degenerative Extrapyramidal and movement disorders Basal ganglia disease Parkinsonism PD Postencephalitic NMS PKAN Tauopathy PSP Striatonigral degeneration Hemiballismus HD OA Dyskinesia Dystonia Status dystonicus Spasmodic torticollis Meige's Blepharospasm Athetosis Chorea Choreoathetosis Myoclonus Myoclonic epilepsy Akathisia Tremor Essential tremor Intention tremor Restless legs Stiff-person Dementia Tauopathy Alzheimer's Early-onset Primary progressive aphasia Frontotemporal dementia / Frontotemporal lobar degeneration Pick's Dementia with Lewy bodies Posterior cortical atrophy Vascular dementia Mitochondrial disease Leigh syndrome Demyelinating Autoimmune Inflammatory Multiple sclerosis For more detailed coverage, see Template:Demyelinating diseases of CNS Episodic/ paroxysmal Seizures and epilepsy Focal Generalised Status epilepticus For more detailed coverage, see Template:Epilepsy Headache Migraine Cluster Tension For more detailed coverage, see Template:Headache Cerebrovascular TIA Stroke For more detailed coverage, see Template:Cerebrovascular diseases Other Sleep disorders For more detailed coverage, see Template:Sleep CSF Intracranial hypertension Hydrocephalus Normal pressure hydrocephalus Choroid plexus papilloma Idiopathic intracranial hypertension Cerebral edema Intracranial hypotension Other Brain herniation Reye syndrome Hepatic encephalopathy Toxic encephalopathy Hashimoto's encephalopathy Both/either Degenerative SA Friedreich's ataxia Ataxia–telangiectasia MND UMN only: Primary lateral sclerosis Pseudobulbar palsy Hereditary spastic paraplegia LMN only: Distal hereditary motor neuronopathies Spinal muscular atrophies SMA SMAX1 SMAX2 DSMA1 Congenital DSMA Spinal muscular atrophy with lower extremity predominance (SMALED) SMALED1 SMALED2A SMALED2B SMA-PCH SMA-PME Progressive muscular atrophy Progressive bulbar palsy Fazio–Londe Infantile progressive bulbar palsy both: Amyotrophic lateral sclerosis
Contents 1 Signs and symptoms 2 Causes 2.1 Asphyxia 2.2 Neonatal jaundice 2.3 Thalamic stroke 2.4 Fahr's syndrome 3 Treatments 4 Related disorders 4.1 Choreoathetosis 4.2 Cerebral palsy 4.3 Pseudoathetosis 5 Social implications 6 History 7 Research directions 8 See also 9 References 10 External links Signs and symptoms [ edit ] Athetosis can vary from mild to severe motor dysfunction; it is generally characterized by unbalanced, involuntary movements of muscle and a difficulty maintaining a symmetrical posture. ... It is proposed that this loss of proprioception and the ensuing loss of synergic stabilization may also lead to abnormal movements, such as those dealt with in athetosis. [8] Fahr's syndrome [ edit ] Main article: Fahr's syndrome Treatments [ edit ] There are several different treatment approaches to dealing with athetosis. ... ISBN 978-1-58890-514-7 . ^ a b c d e Foley J (April 1983). "The athetoid syndrome. A review of a personal series" . ... External links [ edit ] Classification D ICD - 10 : R25.8 ICD - 9-CM : 781.0 MeSH : D001264 DiseasesDB : 16662 SNOMED CT : 44913001 v t e Symptoms and signs relating to movement and gait Gait Gait abnormality CNS Scissor gait Cerebellar ataxia Festinating gait Marche à petit pas Propulsive gait Stomping gait Spastic gait Magnetic gait Truncal ataxia Muscular Myopathic gait Trendelenburg gait Pigeon gait Steppage gait Antalgic gait Coordination Ataxia Cerebellar ataxia Dysmetria Dysdiadochokinesia Pronator drift Dyssynergia Sensory ataxia Asterixis Abnormal movement Athetosis Tremor Fasciculation Fibrillation Posturing Abnormal posturing Opisthotonus Spasm Trismus Cramp Tetany Myokymia Joint locking Paralysis Flaccid paralysis Spastic paraplegia Spastic diplegia Spastic paraplegia Syndromes Monoplegia Diplegia / Paraplegia Hemiplegia Triplegia Tetraplegia / Quadruplegia General causes Upper motor neuron lesion Lower motor neuron lesion Weakness Hemiparesis Other Rachitic rosary Hyperreflexia Clasp-knife response v t e Diseases of the nervous system , primarily CNS Inflammation Brain Encephalitis Viral encephalitis Herpesviral encephalitis Limbic encephalitis Encephalitis lethargica Cavernous sinus thrombosis Brain abscess Amoebic Brain and spinal cord Encephalomyelitis Acute disseminated Meningitis Meningoencephalitis Brain / encephalopathy Degenerative Extrapyramidal and movement disorders Basal ganglia disease Parkinsonism PD Postencephalitic NMS PKAN Tauopathy PSP Striatonigral degeneration Hemiballismus HD OA Dyskinesia Dystonia Status dystonicus Spasmodic torticollis Meige's Blepharospasm Athetosis Chorea Choreoathetosis Myoclonus Myoclonic epilepsy Akathisia Tremor Essential tremor Intention tremor Restless legs Stiff-person Dementia Tauopathy Alzheimer's Early-onset Primary progressive aphasia Frontotemporal dementia / Frontotemporal lobar degeneration Pick's Dementia with Lewy bodies Posterior cortical atrophy Vascular dementia Mitochondrial disease Leigh syndrome Demyelinating Autoimmune Inflammatory Multiple sclerosis For more detailed coverage, see Template:Demyelinating diseases of CNS Episodic/ paroxysmal Seizures and epilepsy Focal Generalised Status epilepticus For more detailed coverage, see Template:Epilepsy Headache Migraine Cluster Tension For more detailed coverage, see Template:Headache Cerebrovascular TIA Stroke For more detailed coverage, see Template:Cerebrovascular diseases Other Sleep disorders For more detailed coverage, see Template:Sleep CSF Intracranial hypertension Hydrocephalus Normal pressure hydrocephalus Choroid plexus papilloma Idiopathic intracranial hypertension Cerebral edema Intracranial hypotension Other Brain herniation Reye syndrome Hepatic encephalopathy Toxic encephalopathy Hashimoto's encephalopathy Both/either Degenerative SA Friedreich's ataxia Ataxia–telangiectasia MND UMN only: Primary lateral sclerosis Pseudobulbar palsy Hereditary spastic paraplegia LMN only: Distal hereditary motor neuronopathies Spinal muscular atrophies SMA SMAX1 SMAX2 DSMA1 Congenital DSMA Spinal muscular atrophy with lower extremity predominance (SMALED) SMALED1 SMALED2A SMALED2B SMA-PCH SMA-PME Progressive muscular atrophy Progressive bulbar palsy Fazio–Londe Infantile progressive bulbar palsy both: Amyotrophic lateral sclerosis
Solid tumour with metastasis (e.g. breast cancer or classically squamous cell carcinoma , which can be PTHrP -mediated) Solid tumour with humoral mediation of hypercalcaemia (e.g. lung cancer , most commonly non-small cell lung cancer [16] or kidney cancer , phaeochromocytoma ) Haematologic cancers ( multiple myeloma , lymphoma , leukaemia ) Ovarian small cell carcinoma of the hypercalcemic type Vitamin-D disorders [ edit ] Hypervitaminosis D (vitamin D intoxication) Elevated 1,25(OH) 2 D (see calcitriol under Vitamin D ) levels (e.g. sarcoidosis and other granulomatous diseases such as tuberculosis , berylliosis , histoplasmosis , Crohn's disease , and granulomatosis with polyangiitis ) Idiopathic hypercalcaemia of infancy [17] Rebound hypercalcaemia after rhabdomyolysis High bone-turnover [ edit ] Hyperthyroidism Multiple myeloma Prolonged immobilization Paget's disease Thiazide use Vitamin A intoxication Kidney failure [ edit ] Tertiary hyperparathyroidism Aluminium intoxication Milk-alkali syndrome Other [ edit ] Acromegaly Adrenal insufficiency Zollinger–Ellison syndrome Diagnosis [ edit ] Diagnosis should generally include either a corrected calcium or ionized calcium level and be confirmed after a week. [1] There is, however, controversy around the usefulness of corrected calcium as it may be no better than total calcium. [18] The normal range is 2.1–2.6 mmol/L (8.8–10.7 mg/dL , 4.3–5.2 mEq/L ), with levels greater than 2.6 mmol/L defined as hypercalcaemia. [1] [2] [4] Moderate hypercalcaemia is a level of 2.88–3.5 mmol/L (11.5–14 mg/dL) while severe hypercalcaemia is > 3.5 mmol/L (>14 mg/dL). [19] ECG [ edit ] An Osborn wave, an abnormal EKG tracing that can be associated with hypercalcemia. ... External links [ edit ] Classification D ICD - 10 : E83.5 ICD - 9-CM : 275.42 MeSH : D006934 DiseasesDB : 6196 SNOMED CT : 66931009 External resources MedlinePlus : 000365 eMedicine : med/1068 emerg/260 ped/1062 Patient UK : Hypercalcaemia v t e Metal deficiency and toxicity disorders Iron excess: Iron overload Hemochromatosis Hemochromatosis/HFE1 Juvenile/HFE2 HFE3 African iron overload/HFE4 Aceruloplasminemia Atransferrinemia Hemosiderosis deficiency: Iron deficiency Copper excess: Copper toxicity Wilson's disease deficiency: Copper deficiency Menkes disease / Occipital horn syndrome Zinc excess: Zinc toxicity deficiency: Acrodermatitis enteropathica Other Inborn errors of metabolism v t e Paraneoplastic syndromes Endocrine Hypercalcaemia SIADH Zollinger–Ellison syndrome Cushing's syndrome Hematological Multicentric reticulohistiocytosis Nonbacterial thrombotic endocarditis Neurological Paraneoplastic cerebellar degeneration Encephalomyelitis Limbic encephalitis Opsoclonus Polymyositis Transverse myelitis Lambert–Eaton myasthenic syndrome Anti-NMDA receptor encephalitis Musculoskeletal Dermatomyositis Hypertrophic osteopathy Mucocutaneous reactive erythema Erythema gyratum repens Necrolytic migratory erythema papulosquamous Acanthosis nigricans Ichthyosis acquisita Acrokeratosis paraneoplastica of Bazex Extramammary Paget's disease Florid cutaneous papillomatosis Leser-Trélat sign Pityriasis rotunda Tripe palms Other Febrile neutrophilic dermatosis Pyoderma gangrenosum Paraneoplastic pemphigus
Overview Hypercalcemia is a condition in which the calcium level in your blood is above normal. Too much calcium in your blood can weaken your bones, create kidney stones, and interfere with how your heart and brain work. Hypercalcemia is usually a result of overactive parathyroid glands. These four tiny glands are situated in the neck, near the thyroid gland. Other causes of hypercalcemia include cancer, certain other medical disorders, some medications, and taking too much of calcium and vitamin D supplements. Signs and symptoms of hypercalcemia range from nonexistent to severe.