Cockayne syndrome is a rare disease which causes short stature, premature aging ( progeria ), severe photosensitivity , and moderate to severe learning delay. This syndrome also includes failure to thrive in the newborn, very small head (microcephaly), and impaired nervous system development. ... There are three subtypes according to the severity of the disease and the onset of the symptoms: Cockayne syndrome type 1 (type A) , sometimes called “classic” or "moderate" Cockayne syndrome, diagnosed during early childhood Cockayne syndrome type 2 (type B) , sometimes referred to as the “severe” or "early-onset" type, presenting with growth and developmental abnormalities at birth Cockayne syndrome type 3 (type C) , a milder form of the disorder Cockayne syndrome is caused by mutations in either the ERCC8 (CSA) or ERCC6 (CSB) genes.
Genetic Heterogeneity of Cockayne Syndrome Cockayne syndrome is a genetically heterogeneous disorder, and certain types show some overlap with certain forms of xeroderma pigmentosum (XP), another disorder caused by defective DNA repair. ... Paddison et al. (1963) reported a striking pedigree with Cockayne syndrome. In 4 patients with Cockayne syndrome, Brumback et al. (1978) noted development of the triad of normal pressure hydrocephalus: dementia, gait disturbance, and incontinence. ... Although the disorder resembled cerebrooculofacioskeletal syndrome (COFS; 214150), the pathologic and fibroblast studies seemed to indicate that it was the same as Cockayne syndrome. ... The authors cautioned that metronidazole causes acute hepatic failure in Cockayne syndrome, which may be fatal and should be avoided in anyone with a suspected diagnosis of Cockayne syndrome. ... Czeizel and Marchalko (1995) used the designation Cockayne syndrome type III for the disorder in a teenaged girl with characteristic somatic manifestations of Cockayne syndrome, particularly a cachectic phenotype.
Cockayne syndrome A (CSA; 216400) is caused by mutation in the ERCC8 gene (609412) on chromosome 5q11. Among patients with Cockayne syndrome, approximately 80% have mutations in the ERCC6 gene (Licht et al., 2003). For a phenotypic description and a discussion of genetic heterogeneity of Cockayne syndrome, see 216400. Clinical Features Falik-Zaccai et al. (2008) reported a large, highly consanguineous Druze kindred from northern Israel in which 6 members had Cockayne syndrome B. ... Using these criteria increased clinical recognition of Cockayne syndrome in their cohort of 102 patients to around 90%. The authors cautioned that metronidazole causes acute hepatic failure in Cockayne syndrome, which may be fatal and should be avoided in anyone with a suspected diagnosis of Cockayne syndrome.
Cockayne syndrome is a rare disease which causes short stature, premature aging ( progeria ), severe photosensitivity , and moderate to severe learning delay. This syndrome also includes failure to thrive in the newborn, very small head (microcephaly), and impaired nervous system development. ... There are three subtypes according to the severity of the disease and the onset of the symptoms: Cockayne syndrome type 1 (type A) , sometimes called “classic” or "moderate" Cockayne syndrome, diagnosed during early childhood Cockayne syndrome type 2 (type B) , sometimes referred to as the “severe” or "early-onset" type, presenting with growth and developmental abnormalities at birth Cockayne syndrome type 3 (type C) , a milder form of the disorder Cockayne syndrome is caused by mutations in either the ERCC8 (CSA) or ERCC6 (CSB) genes.
A number sign (#) is used with this entry because acrocallosal syndrome (ACLS) and Joubert syndrome-12 (JBTS12), 2 similar disorders, can be caused by homozygous mutation in the KIF7 gene (611254) on chromosome 15q26. Digenic inheritance of Joubert syndrome has also been reported; see MOLECULAR GENETICS. ... Since the manifestations of trisomy and tetrasomy 12p show some overlap with the acrocallosal syndrome (as in the Pallister-Killian syndrome with tetrasomy 12p), Pfeiffer et al. (1992) suggested that the mutation for acrocallosal syndrome may be situated on 12p. (For a discussion of the Pallister-Killian syndrome, see 190070; the KRAS2 gene was used in the study of this syndrome.) This is, of course, inconsistent with the idea that the acrocallosal syndrome is allelic to Greig syndrome, since the latter disorder maps to 7p13.
Hypoplastic tibia-polydactyly syndrome is a very rare congenital malformation syndrome characterized by bilateral hypoplasia of the tibia with polydactyly of the feet and hands. Epidemiology Prevalence is unknown but the syndrome is very rare with only a few case reports described in the literature. ... It is suggested that hypoplastic tibia-polydactyly syndrome and triphalangeal thumb-polysyndactyly syndrome (see this term) may be variants of the same disorder.
The practices were united with each other after both submitted the gene as a candidate to the online service GeneMatcher , which matched them together and allowed them to confirm the syndrome. [7] In 2019, Okamoto proposed that Au–Kline syndrome and Okamoto syndrome were synonymous, because a mutation in the HNRNPK gene had been found in a new Okamoto syndrome patient, and the symptoms were virtually identical. [1] See also [ edit ] CDK13-related disorder Kabuki syndrome References [ edit ] ^ a b c d e f g h i j k l m Okamoto, Nobuhiko (May 2019). "Okamoto syndrome has features overlapping with Au-Kline syndrome and is caused by HNRNPK mutation". ... "Phenotypic spectrum of Au-Kline syndrome: a report of six new cases and review of the literature" . ... PMID 29904177 . ^ "Orphanet: Okamoto syndrome" . www.orpha.net . Retrieved 30 November 2019 . ^ a b c d e f g h i j k l m Au, P.Y. ... External links [ edit ] Au–Kline syndrome at the US National Institutes of Health (NIH) Genetics Home Reference Classification D OMIM : 604916 616580 MeSH : C565736 External resources GeneReviews : Au–Kline Syndrome GARD : Okamoto syndrome Orphanet : 2729 453499
Clinical Features Okamoto et al. (1997) reported what they believed to be a new MCA/MR syndrome in a 2-year-old Japanese girl and an unrelated 15-month-old Japanese boy. ... The authors considered this to be the third reported case of Okamoto syndrome. The infant also had idiopathic splenomegaly and nonspecific MRI changes in the brain, which had not been reported in the first 2 cases. ... Markouri et al. (2008) reported a 2-year-old Greek female with Okamoto syndrome, born to healthy, nonconsanguineous parents. ... Taylor and Aftimos (2010) reported what they believed to be the fifth reported case of Okamoto syndrome. The female offspring of nonconsanguineous parents of mixed ethnic background had multiple congenital anomalies and characteristic facial features.
Okamoto syndrome is characterised by congenital hydronephrosis, intellectual deficit, growth retardation, cleft palate, generalised hypotonia and a characteristic face.
The article describes an 18-year-old female suffering from hebefreno-paranoid schizophrenia who believed that her next door neighbor had transformed her physical self into the patient's double. [3] [6] The syndrome of subjective doubles and its variants were not given the name delusional misidentification syndromes until 1981. [2] Doubles of the self have been reported in literature even before the syndrome was named by Christodoulou. [2] The first patient with symptoms of Capgras syndrome , another delusional misidentification syndrome, was reported in 1923 by Joseph Capgras and Jean Reboul-Lachaux. ... This syndrome is also not defined in the DSM-IV or ICD-10. [7] [16] Additionally, some researchers use varying definitions of the syndrome. ... "The delusional misidentification syndromes: strange, fascinating, and instructive". ... The Little Black Book of Neuropsychology: A Syndrome-Based Approach . Springer. p. 259. ... Leong (April 1991). "A Case of Subjective Fregoli Syndrome" . Journal of Psychiatry and Neuroscience . 16 (2): 103–105.
Cleidocranial dysostosis Other names Cleidocranial dysplasia, [1] Marie-Sainton syndrome, [1] mutational dysostosis [2] Facial and forehead changes along with increased mobility of the shoulder girdles Specialty Medical genetics Symptoms Missing collarbone , prominent forehead, flat nose, shorter [1] Usual onset Present at birth [3] Causes Genetic ( RUNX2 gene) [1] Diagnostic method Based on symptoms and X-rays , confirmed by genetic testing [4] Differential diagnosis Mandibuloacral dysplasia , pyknodysostosis , osteogenesis imperfecta , Hajdu-Cheney syndrome [5] Treatment Supportive care [5] Prognosis Normal life expectancy [3] Frequency One per million people [1] Cleidocranial dysostosis ( CCD ), also called cleidocranial dysplasia , is a birth defect that mostly affects the bones and teeth . [1] The collarbones are typically either poorly developed or absent, which allows the shoulders to be brought close together. [1] The front of the skull often does not close until later, and those affected are often shorter than average. [1] Other symptoms may include a prominent forehead, wide set eyes, abnormal teeth, and a flat nose. [1] Symptoms vary among people; however, intelligence is typically unaffected. [1] The condition is either inherited from a person's parents or occurs as a new mutation . [1] It is inherited in an autosomal dominant manner. [1] It is due to a defect in the RUNX2 gene which is involved in bone formation. [1] Diagnosis is suspected based on symptoms and X-rays with confirmation by genetic testing . [4] Other conditions that can produce similar symptoms include mandibuloacral dysplasia , pyknodysostosis , osteogenesis imperfecta , and Hajdu-Cheney syndrome . [5] Treatment includes supportive measures such as a device to protect the skull and dental care. [5] Surgery may be performed to fix certain bone abnormalities. [4] Life expectancy is generally normal. [3] It affects about one per million people. [1] Males and females are equally commonly affected. [5] Modern descriptions of the condition date to at least 1896. [6] The term is from cleido meaning collarbone, cranial from the Greek κρανιὀς meaning skull, and dysostosis meaning formation of abnormal bone. [7] Contents 1 Signs and symptoms 2 Genetics 3 Diagnosis 4 Treatment 5 Prognosis 6 Epidemiology 7 Notable cases 8 References 9 External links Signs and symptoms [ edit ] Mouth showing many over-retained deciduous teeth and some missing teeth. ... External links [ edit ] Cleidocranial dysostosis at Curlie Classification D ICD - 10 : Q74.0 ICD - 9-CM : 755.59 OMIM : 119600 MeSH : D002973 DiseasesDB : 30594 External resources MedlinePlus : 001589 GeneReviews : Cleidocranial Dysplasia v t e Congenital malformations and deformations of musculoskeletal system / musculoskeletal abnormality Appendicular limb / dysmelia Arms clavicle / shoulder Cleidocranial dysostosis Sprengel's deformity Wallis–Zieff–Goldblatt syndrome hand deformity Madelung's deformity Clinodactyly Oligodactyly Polydactyly Leg hip Hip dislocation / Hip dysplasia Upington disease Coxa valga Coxa vara knee Genu valgum Genu varum Genu recurvatum Discoid meniscus Congenital patellar dislocation Congenital knee dislocation foot deformity varus Club foot Pigeon toe valgus Flat feet Pes cavus Rocker bottom foot Hammer toe Either / both fingers and toes Polydactyly / Syndactyly Webbed toes Arachnodactyly Cenani–Lenz syndactylism Ectrodactyly Brachydactyly Stub thumb reduction deficits / limb Acheiropodia Ectromelia Phocomelia Amelia Hemimelia multiple joints Arthrogryposis Larsen syndrome RAPADILINO syndrome Axial Skull and face Craniosynostosis Scaphocephaly Oxycephaly Trigonocephaly Craniofacial dysostosis Crouzon syndrome Hypertelorism Hallermann–Streiff syndrome Treacher Collins syndrome other Macrocephaly Platybasia Craniodiaphyseal dysplasia Dolichocephaly Greig cephalopolysyndactyly syndrome Plagiocephaly Saddle nose Vertebral column Spinal curvature Scoliosis Klippel–Feil syndrome Spondylolisthesis Spina bifida occulta Sacralization Thoracic skeleton ribs : Cervical Bifid sternum : Pectus excavatum Pectus carinatum v t e Genetic disorders relating to deficiencies of transcription factor or coregulators (1) Basic domains 1.2 Feingold syndrome Saethre–Chotzen syndrome 1.3 Tietz syndrome (2) Zinc finger DNA-binding domains 2.1 ( Intracellular receptor ): Thyroid hormone resistance Androgen insensitivity syndrome PAIS MAIS CAIS Kennedy's disease PHA1AD pseudohypoaldosteronism Estrogen insensitivity syndrome X-linked adrenal hypoplasia congenita MODY 1 Familial partial lipodystrophy 3 SF1 XY gonadal dysgenesis 2.2 Barakat syndrome Tricho–rhino–phalangeal syndrome 2.3 Greig cephalopolysyndactyly syndrome / Pallister–Hall syndrome Denys–Drash syndrome Duane-radial ray syndrome MODY 7 MRX 89 Townes–Brocks syndrome Acrocallosal syndrome Myotonic dystrophy 2 2.5 Autoimmune polyendocrine syndrome type 1 (3) Helix-turn-helix domains 3.1 ARX Ohtahara syndrome Lissencephaly X2 MNX1 Currarino syndrome HOXD13 SPD1 synpolydactyly PDX1 MODY 4 LMX1B Nail–patella syndrome MSX1 Tooth and nail syndrome OFC5 PITX2 Axenfeld syndrome 1 POU4F3 DFNA15 POU3F4 DFNX2 ZEB1 Posterior polymorphous corneal dystrophy Fuchs' dystrophy 3 ZEB2 Mowat–Wilson syndrome 3.2 PAX2 Papillorenal syndrome PAX3 Waardenburg syndrome 1&3 PAX4 MODY 9 PAX6 Gillespie syndrome Coloboma of optic nerve PAX8 Congenital hypothyroidism 2 PAX9 STHAG3 3.3 FOXC1 Axenfeld syndrome 3 Iridogoniodysgenesis, dominant type FOXC2 Lymphedema–distichiasis syndrome FOXE1 Bamforth–Lazarus syndrome FOXE3 Anterior segment mesenchymal dysgenesis FOXF1 ACD/MPV FOXI1 Enlarged vestibular aqueduct FOXL2 Premature ovarian failure 3 FOXP3 IPEX 3.5 IRF6 Van der Woude syndrome Popliteal pterygium syndrome (4) β-Scaffold factors with minor groove contacts 4.2 Hyperimmunoglobulin E syndrome 4.3 Holt–Oram syndrome Li–Fraumeni syndrome Ulnar–mammary syndrome 4.7 Campomelic dysplasia MODY 3 MODY 5 SF1 SRY XY gonadal dysgenesis Premature ovarian failure 7 SOX10 Waardenburg syndrome 4c Yemenite deaf-blind hypopigmentation syndrome 4.11 Cleidocranial dysostosis (0) Other transcription factors 0.6 Kabuki syndrome Ungrouped TCF4 Pitt–Hopkins syndrome ZFP57 TNDM1 TP63 Rapp–Hodgkin syndrome / Hay–Wells syndrome / Ectrodactyly–ectodermal dysplasia–cleft syndrome 3 / Limb–mammary syndrome / OFC8 Transcription coregulators Coactivator: CREBBP Rubinstein–Taybi syndrome Corepressor: HR ( Atrichia with papular lesions )
Disorders to Consider in the Differential Diagnosis of Cleidocranial Dysplasia (CCD) Spectrum Disorder View in own window Disorder Name or Genetic Mechanism Gene(s) MOI Clinical Features Shared w/CCD spectrum disorder Distinguishing from CCD spectrum disorder 16q22 deletion (incl deletion of CBFB ) (OMIM 614541) CBFB Wide-open fontanelles & short clavicles Failure to thrive Delayed psychomotor development Congenital heart defect Crane-Heise syndrome (OMIM 218090) Unknown AR? Large head Poorly mineralized calvarium Cleft lip & palate Low-set, dysplastic ears Hypoplastic clavicles & scapulae Hypoplasic/absent phalanges Absence of cervical vertebrae Genital hypoplasia Lethal condition IUGR Multiple joint contractures Severe vertebral & limb anomalies w/absence of cervical vertebrae Mandibuloacral dysplasia (OMIM PS248370) LMNA , ZMPSTE24 AR Short stature, delayed closure of cranial sutures, mandibular hypoplasia, & dysplastic clavicles Scalp hair sparse by 3rd decade Progressively stiff joints Acroosteodysplasia of fingers & toes w/delayed ossification of carpal bones Micrognathia Early tooth loss Atrophic skin w/↓ subcutaneous fat Acroosteolysis Hyperpigmentation Lipodystrophy Alopecia Pycnodysostosis CTSK AR Short stature, osteopetrosis w/↑ bone fragility, short terminal phalanges Failure of closure of cranial sutures w/persistence of an open fontanelle Radio-opacity of all bones ↑ due to ↑ density of the trabecular bone but not the cortices Osteopetrosis Acrosteolysis Yunis Varon syndrome (OMIM 216340) FIG4 AR Prenatal growth deficiency Wide-open fontanelles & sutures, unusual mineralization of the skull, & hypoplastic clavicles Hypoplastic or absent thumbs & great toes Absence/hypoplasia of thumbs, halluces & distal phalanges Gracile bones Brain malformations CDAGS syndrome (OMIM 603116) Unknown AR Craniosynostosis, delayed closure of fontanelles, cranial defects, clavicular hypoplasia 1 Anal & genitourinary malformations Skin eruption Craniosynostosis Anal anomalies Skin lesions (porokeratosis) Hypophosphatasia 2 ALPL AR AD 3 Generalized defect of mineralization w/delayed ossification of multiple skeletal elements Children w/infantile form may present w/very poorly mineralized cranium, widened cranial sutures short ribs, & narrow thorax. Very low alkaline phosphatase activity in serum & tissues Clavicles least affected No supernumerary teeth Premature deciduous tooth loss Rachitic skeletal changes Nephrocalcinosis Hypercalcemia Parietal foramina with cleidocranial dysplasia 4 MSX2 AD Parietal foramina Mild craniofacial dysmorphisms Clavicular hypoplasia Not associated w/dental abnormalities seen in classic CCD 5 Microduplications upstream of MSX2 Phenocopy of cleidocranial dysplasia 6 Synpolydactyly in some Familial supernumerary teeth AD Supernumerary premolar teeth Nonsyndromic supernumerary premolar teeth 7 Hypothyroidism Delayed fontanelle closure IUGR = intrauterine growth restriction; MOI = mode of inheritance 1. CDAGS syndrome brings together the apparently opposing pathophysiologic and developmental processes of accelerated suture closure and delayed ossification [Mendoza-Londono et al 2005]. 2.
Cleidocranial dysplasia is a condition that primarily affects development of the bones and teeth. Signs and symptoms of cleidocranial dysplasia can vary widely in severity, even within the same family. Individuals with cleidocranial dysplasia usually have underdeveloped or absent collarbones, also called clavicles ("cleido-" in the condition name refers to these bones). As a result, their shoulders are narrow and sloping, can be brought unusually close together in front of the body, and in some cases can be made to meet in the middle of the body. Delayed maturation of the skull (cranium) is also characteristic of this condition, including delayed closing of the growth lines where the bones of the skull meet (sutures) and larger than normal spaces (fontanelles) between the skull bones that are noticeable as "soft spots" on the heads of infants.
Cleidocranial dysplasia (CCD) affects the development of the bones, skull, and teeth. Signs and symptoms include underdeveloped or absent collarbones (clavicles), dental abnormalities, and delayed closing of the spaces between the skull bones (fontanels). Other symptoms may include decreased bone density (osteopenia), hearing loss, bone abnormalities of the hands, and recurrent sinus and ear infections. People with CCD may develop curvature of the spine (scoliosis), osteoporosis, and may be shorter than average. CCD occurs due to a RUNX2 gene that is not working correctly and is inherited in an autosomal dominant pattern.
A number sign (#) is used with this entry because of evidence that cleidocranial dysplasia (CCD) is caused by heterozygous loss-of-function mutation in the RUNX2 gene (600211), encoding transcription factor CBFA1, on chromosome 6p21. Heterozygous duplication in RUNX2 resulting in a gain of function causes metaphyseal dysplasia and maxillary hypoplasia with or without brachydactyly (MDMHB; 156510). Description The main clinical features of CCD include persistently open skull sutures with bulging calvaria, hypoplasia or aplasia of the clavicles permitting abnormal facility in apposing the shoulders, wide pubic symphysis, short middle phalanx of the fifth fingers, dental anomalies, and often vertebral malformation. See 168550 for a discussion of the combination of cleidocranial dysplasia and parietal foramina. Pycnodysostosis (265800) and mandibuloacral dysplasia (248370) are disorders to be considered in the differential diagnosis of cleidocranial dysplasia.
Goodman et al. (1975) described 2 families in which offspring of unaffected consanguineous parents had a particularly severe form of cleidocranial dysplasia. Spinal anomalies were present and the affected persons were dwarfed. HEENT - Brachycephaly Growth - Dwarfism Inheritance - Severe autosomal recessive form, usually dominant Skel - Aplasia of clavicles - Spinal anomalies ▲ Close
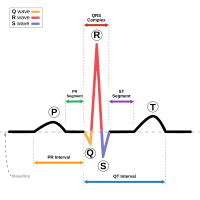
A list of genes in which variants have been associated with short QT syndrome can be found in the table below. ... "Short QT syndrome" . Cardiovascular Research . 67 (3): 357–66. doi : 10.1016/j.cardiores.2005.03.026 . ... "Sudden death associated with short-QT syndrome linked to mutations in HERG" . ... (February 2014). "Type 2 short QT syndrome and vestibular dysfunction: mirror of the Jervell and Lange-Nielsen syndrome?". ... External links [ edit ] "Short QT syndrome" . Genetics Home Reference . U.S.
15q13.3 microdeletion syndrome is a genetic disorder caused by a deletion of several genes on chromosome 15 . When a syndrome is caused by the deletion of several genes, it is also known as a microdeletion syndrome or a contiguous gene deletion syndrome. Individuals with 15q13.3 microdeletion syndrome may have very different signs and symptoms from other affected individuals (even within the same family), or no symptoms at all. ... Various dysmorphic (abnormally formed) features have been reported, but there are no consistent physical features among individuals who have the condition. 15q13.3 microdeletion syndrome is caused by a deletion on the long arm of chromosome 15 that spans at least 7 genes and usually includes the CHRNA7 gene.It can be inherited in an autosomal dominant manner with reduced penetrance, or can occur as a new (de novo) deletion.
Individuals with the 15q13.3 microdeletion are at increased risk for a wide range of clinical manifestations including intellectual disability, seizures, autism spectrum disorders, and schizophrenia; however, the microdeletion itself does not appear to lead to a clinically recognizable syndrome and a subset of persons with the deletion have no obvious clinical findings. ... The deletion itself may not lead to a clinically recognizable syndrome and a subset of persons with the deletion have no obvious clinical findings, implying that penetrance for the deletion is incomplete.
15q13.3 microdeletion is a chromosomal change in which a small piece of chromosome 15 is deleted in each cell. The deletion occurs on the long (q) arm of the chromosome at a position designated q13.3. This chromosomal change increases the risk of intellectual disability, seizures, behavioral problems, and psychiatric disorders. However, some people with a 15q13.3 microdeletion do not appear to have any associated features. About half of all people with a 15q13.3 microdeletion have learning difficulties or intellectual disability, which is usually mild or moderate.
A number sign (#) is used with this entry because it represents a contiguous gene deletion syndrome (chr15: 28.7-30.3 Mb, NCBI36). ... See also chromosome 15q11-q13 duplication syndrome (608636), which has been associated with overlapping features. ... Clinical Features Sharp et al. (2008) reported a recurrent microdeletion syndrome characterized by mental retardation, epilepsy, and variable dysmorphism of the face and digits. ... Sharp et al. (2008) recommended that testing for the 15q13.3 deletion syndrome should be considered in individuals with unexplained mental retardation, seizures, and mild dysmorphic features. ... They concluded that knockout of Chrna7 in mice does not recapitulate phenotypes observed in humans with chromosome 15q13.3 microdeletion syndrome.
15q13.3 microdeletion (microdel15q13.3) syndrome is characterized by a wide spectrum of neurodevelopmental disorders with no or subtle dysmorphic features. ... Males are more likely to be symptomatic. Clinical description The syndrome manifests in childhood or later in life. ... Asymptomatic carriers may have a history of learning difficulties. Etiology The syndrome is due to submicroscopic deletions in the proximal 15q region, known for its instability and high density of low-copy repeat (LCR) sequences mediating non-allelic homologous recombination (NAHR), resulting in genomic rearrangements. ... Genetic counseling should be offered cautiously as the syndrome may be either sporadic or familial. ... However, not all carriers will develop the syndrome. Management and treatment The clinical picture should guide treatment.
Landau-Kleffner syndrome (LKS) is a rare neurological syndrome characterized by the sudden or gradual development of aphasia (the inability to understand or express language) and recurrent seizures (epilepsy). Children with LKS typically develop normally until signs and symptoms of the syndrome begin to develop between age 2 and 8 years. ... In about 20% of people with LKS, mutations (changes) in the GRIN2A gene have been identified. The syndrome is inherited in an autosomal dominant manner. In other cases, the syndrome may be caused by changes to other unidentified genes. LKS is diagnosed when a doctor sees clinical features that are consistent with the syndrome such as a loss of speech and an electroencephalogram (EEG) that shows specific kinds of seizure activity.
Differential diagnosis Differential diagnosis includes any epileptic syndrome with sleep potentiation of epileptiform activity such as Landau-Kleffner syndrome, Panayiotopoulos and Gastaut types of benign childhood occipital epilepsy and rolandic epilepsy (see these terms).
Landau-Kleffner syndrome (LKS) is an age-related epileptic encephalopathy where developmental regression occurs mainly in the language domain and the electroencephalographic (EEG) abnormalities are mainly localized around the temporal-parietal regions. ... Differential diagnosis The differential diagnosis includes any epileptic syndrome with sleep potentiation of epileptiform activity such as continuous spikes and waves during sleep, Panayiotopoulos and Gastaut types of benign childhood occipital epilepsy and rolandic epilepsy (see these terms).
Unsourced material may be challenged and removed. Find sources: "Landau–Kleffner syndrome" – news · newspapers · books · scholar · JSTOR ( February 2015 ) ( Learn how and when to remove this template message ) Landau–Kleffner syndrome Landau–Kleffner syndrome is characterized by aphasia and an abnormal EEG Specialty Neurology , psychiatry Landau–Kleffner syndrome (LKS) —also called infantile acquired aphasia , acquired epileptic aphasia [1] or aphasia with convulsive disorder —is a rare childhood neurological syndrome . ... In a study of 77 cases of Landau–Kleffner syndrome, 6 were found to have this type of aphasia. ... "Syndrome of acquired aphasia with convulsive disorder in children". ... PMID 9867583 . ^ a b c "Landau-Kleffner Syndrome (LKS or Infantile Acquired Aphasia)" (medicinenet) . ... (December 1995). "Landau-Kleffner syndrome. Treatment with subpial intracortical transection".
The conditions in the epilepsy-aphasia spectrum, which all begin in childhood, include Landau-Kleffner syndrome (LKS), epileptic encephalopathy with continuous spike-and-wave during sleep syndrome (ECSWS), autosomal dominant rolandic epilepsy with speech dyspraxia (ADRESD), intermediate epilepsy-aphasia disorder (IEAD), atypical childhood epilepsy with centrotemporal spikes (ACECTS), and childhood epilepsy with centrotemporal spikes (CECTS).
Rolandic epilepsy-speech dyspraxia syndrome is a rare, genetic epilepsy characterized by speech disorder (including a range of symptoms from dysarthria, speech dyspraxia, receptive and expressive language delay/regression and acquired aphasia to subtle impairments of conversational speech) and epilepsy (mostly focal and secondary generalized childhood-onset seizures, sometimes with aura).
Fowler’s syndrome mainly affects young women and leads to the inability to empty the bladder ( urinary retention ). Many women have no other symptoms, although some women experience stomach pain. Fowler's syndrome is caused by spasms of the external urethral sphincter, a band of muscle that opens and closes at the exit of the bladder . The cause is unknown, but it has been known to occur after a surgical procedure, childbirth, opiate use, or other medical condition. Fowler's syndrome is difficult to diagnose, but many women with Fowler's syndrome have abnormal electrical activity on a specialized test called concentric needle electromyography . Fowler's syndrome is most often treated by using a device placed inside the body that helps stimulate the bladder.
A rare urogenital disease characterized by otherwise unexplained chronic urinary retention of more than 1 liter of sterile urine on catheterization, an asensitive bladder with loss of urge to void, and no help of straining. Poor tolerance of self-catheterization is typically reported. The condition occurs in women between menarche and menopause.
Autosomal dominant Alport syndrome is a genetic condition characterized by kidney disease, hearing loss, and eye abnormalities. Most affected individuals experience progressive loss of kidney function, usually resulting in end-stage kidney disease. People with Alport syndrome frequently develop sensorineural hearing loss in late childhood or early adolescence. The eye abnormalities seen in this condition seldom lead to vision loss. Alport syndrome can have different patterns of inheritance. Alport syndrome has autosomal dominant inheritance in about 5 percent of cases. People with this form of Alport syndrome have one mutation in either the COL4A3 or COL4A4 gene in each cell.
Supernumerary nipples–uropathies–Becker's nevus syndrome Other names SNUB syndrome Specialty Dermatology Supernumerary nipples–uropathies–Becker's nevus syndrome (also known as "SNUB syndrome" [1] ) is a cutaneous condition that may be associated with genitourinary tract abnormalities. [1] See also [ edit ] Silver–Russell syndrome List of cutaneous conditions References [ edit ] ^ a b Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007).
Visual snow syndrome affects the way the visual information is processed by the brain and eyes. People with visual snow syndrome see many flickering tiny dots, like snow or static, that fill the entire visual field. ... In addition, people with visual snow syndrome may have light sensitivity, difficulty with night vision, migraines , and ringing in the ears. The symptoms do not usually change over time. The cause of visual snow syndrome is unknown, but it is likely to be involve how the brain processes vision. Visual snow syndrome is diagnosed based on the symptoms.
Visual snow syndrome is a rare neurologic disease characterized by persistent continuous bilateral visual experience of flickering snow-like dots throughout the visual field in association with other visual (including palinopsia, enhanced entopic phenomena, nyctalopia, photophobia and photopsia) and non-visual (migraine with or without aura, tinnitus and occasionally tremor) symptoms.
20p12.3 microdeletion syndrome is a recently described syndrome characterized by Wolff-Parkinson-White syndrome (see this term), variable developmental delay and facial dysmorphism. ... Clinical description Dysmorphic features include macrocephaly, hypertelorism, down-slanting palpebral fissures and microstomia. Etiology This syndrome is caused by an interstitial deletion encompassing 20p12.3. ... They have a variable size with the smallest region of overlap including only one gene, BMP2 , which is a good candidate gene for explaining the phenotype of Wolff-Parkinson-White syndrome.
Marcus-Gunn syndrome is characterised by ptosis associated with maxillopalpebral synkinesis. Epidemiology The syndrome is responsible for 5% of congenital ptoses. ... Differential diagnosis Inverse Marcus Gunn phenomenon and Marin-Amat syndrome present as eyelid drooping on jaw opening. The first is a congenital condition in which the eyelid levator muscle is inhibited, while Marin-Amat syndrome occurs after facial paralysis and is not associated with impairment of orbicularis oculi and levator muscle function. Genetic counseling The syndrome is generally unilateral and sporadic, but bilateral and familial cases with autosomal dominant transmission have been reported.
Marcus Gunn phenomenon is a rare condition characterized by movement of the upper eyelid in a rapid rising motion (a "wink") each time the jaw moves. The wink phenomenon may be elicited by opening the mouth, thrusting the jaw to the side, jaw protrusion, chewing, smiling, or sucking. It is usually present at birth and may occur with other eye abnormalities (such as strabismus) or vision problems. Although it usually affects one eye, it can affect both eyes in rare cases. The exact cause is not known. Marcus Gunn phenomenon is generally sporadic , but familial cases have been reported.
Description The Marcus Gunn phenomenon consists of unilateral congenital ptosis and rapid exaggerated elevation of the ptotic lid on moving of the lower jaw. Although it usually persists into adult life, the phenomenon is seen in its most marked forms in infancy when the rapid spasmodic movements of the lid are apparent during sucking and thus are noted soon after birth (Doco-Fenzy et al., 2006). Inheritance Falls et al. (1949) reported 3 cases of Marcus Gunn phenomenon in 2 generations, suggesting autosomal dominant inheritance. Kirkham (1969) described brother and sister with unilateral Marcus Gunn phenomenon. Cytogenetics Doco-Fenzy et al. (2006) reported a girl with Marcus Gunn phenomenon and multiple other congenital anomalies associated with a pure de novo direct duplication of chromosome 12q: dup(12)(q24.1-q24.2).
Kenny-Caffey syndrome Other names Kenny syndrome Kenny-Caffey syndrome is a rare genetic condition causing skeletal abnormalities. [1] Individuals with the condition have a shortened stature and thickened long bones. Hypocalcemia is also common. [2] KCS is autosomal dominant and caused by a mutation in FAM111A . [2] It affects males and females in equal proportion. [1] Treatment is based on symptoms. [1] References [ edit ] ^ a b c "Kenny-Caffey Syndrome" . ^ a b "OMIM Entry - # 127000 - KENNY-CAFFEY SYNDROME, TYPE 2; KCS2" . www.omim.org .
A rare primary bone dysplasia syndrome characterized by growth retardation with proportionate short stature, cortical thickening and medullary stenosis of the long bones, delayed anterior fontanelle closure, hypocalcemia due to congenital hypoparathyroidism and facial dysmorphism, including prominent forehead, microphthalmia, and micrognathia.
A number sign (#) is used with this entry because the autosomal recessive form of Kenny-Caffey syndrome (KCS1) is caused by mutation in the gene encoding tubulin-specific chaperone E (TBCE; 604934). Biallelic mutation in the TBCE gene can also cause Sanjad-Sakati syndrome (HRDS; 241410) and PEAMO (617207). Inheritance of Kenny-Caffey syndrome is most often autosomal dominant (KCS2; 127000) (Franceschini et al., 1992). Clinical Features Franceschini et al. (1992) suggested autosomal recessive inheritance of Kenny-Caffey syndrome in female and male sibs, born of normal consanguineous parents. ... Molecular Genetics Parvari et al. (2002) demonstrated mutations in the TBCE gene in both Kenny-Caffey syndrome and Sanjad-Sakati syndrome (see 604934.0001).
A number sign (#) is used with this entry because of evidence that autosomal dominant Kenny-Caffey syndrome (KCS2) is caused by heterozygous mutation in the FAM111A gene (615292) on chromosome 11q12. ... See KCS1 (244460) for a discussion of an autosomal recessive form of Kenny-Caffey syndrome. Clinical Features Kenny and Linarelli (1966) described mother and son who were markedly dwarfed with dense tubular bones and narrow marrow cavities. ... McKusick (1980) observed severe hypermetropia and apparent papilledema thought to represent pseudotumor cerebri in a 6-year-old boy with Kenny-Caffey syndrome. Boynton et al. (1979) described a similar finding, with tortuous and dilated retinal vessels. ... In addition to previously described characteristics of the syndrome, hypoplastic nails, persistent neutropenia, abnormal T-cell function, and neonatal liver disease were observed. ... Molecular Genetics In 5 patients with autosomal dominant Kenny-Caffey syndrome and 5 patients with gracile bone dysplasia (602361), Unger et al. (2013) identified heterozygosity for 6 mutations in the FAM111A gene (615292.0001-615292.0006, respectively).
Kenny-Caffey syndrome type 2 is a genetic disorder that affects the skeleton, head, and eyes. It causes frequent episodes of low blood calcium ( hypocalcemia ). This syndrome is caused by changes (pathogenic variants) in the FAM111A gene and is inherited in an autosomal dominant pattern.
Singleton-Merten syndrome is a very rare disease that affect many organs. ... Severe systemic lupus erythematosus can also occur with Singleton-Merten syndrome. Singleton-Merten syndrome is caused by mutations in the IFIH1 gene, and in the DDX58 genes (which causes anatypical form of Singleton-Merten syndrome where there are no teeth problems). ... The genes causing Singeleton-Merten syndrome can activate type I interferon (IFN1) responses. ... These diseases include Aicardi-Goutières syndrome , familial chilblain lupus , spondyloenchondrodysplasia , the proteasome associated autoinflammatory syndromes , IFN-stimulated gene 15 ( ISG15 ) deficiency , Singleton-Merten syndrome, STING-associated vasculopathy with onset in infancy (SAVI) .
A number sign (#) is used with this entry because of evidence that Singleton-Merten syndrome-2 (SGMRT2) is caused by heterozygous mutation in the DDX58 gene (609631) on chromosome 9p21. Description Singleton-Merten syndrome-2 is characterized by variable expression of glaucoma, aortic calcification, and skeletal abnormalities, without dental anomalies (summary by Jang et al., 2015). For a general phenotypic description and discussion of genetic heterogeneity of Singleton-Merten syndrome, see SGMRT1 (182250). Clinical Features Jang et al. (2015) studied a large 4-generation Korean family with aortic calcification, glaucoma, and skeletal abnormalities. ... Jang et al. (2015) designated the phenotype in the 2 families 'atypical Singleton-Merten syndrome' manifesting with variable expression of glaucoma, aortic calcification, and skeletal abnormalities, without dental anomalies.
A number sign (#) is used with this entry because of evidence that Singleton-Merten syndrome-1 (SGMRT1) is caused by heterozygous mutation in the IFIH1 gene (606951) on chromosome 2q24. Description Singleton-Merten syndrome (SGMRT) is an uncommon autosomal dominant disorder characterized by abnormalities of blood vessels, teeth, and bone. ... Genetic Heterogeneity of Singleton-Merten Syndrome An atypical form of Singleton-Merten syndrome (SGMRT2; 616298) is caused by mutation in the DDX58 gene (609631) on chromosome 9p21. ... Inheritance The transmission pattern of Singleton-Merten syndrome in the family described by Feigenbaum et al. (1988) was consistent with autosomal dominant inheritance. Molecular Genetics In affected individuals from 3 unrelated families with Singleton-Merten syndrome, previously reported by Feigenbaum et al. (1988), Rutsch et al. (2005), and Valverde et al. (2010), respectively, Rutsch et al. (2015) performed whole-exome sequencing and identified heterozygosity for a missense mutation in the IFIH1 gene (R822Q; 606951.0009).
Singleton-Merten dysplasia is characterized by dental dysplasia, progressive calcification of the thoracic aorta with stenosis, osteoporosis and expansion of the marrow cavities in hand bones. Additional features included generalized muscle weakness and atrophy, and chronic psoriasiform skin eruptions. It has been reported in four unrelated patients (male and female) and in a family with multiple affected members (male).
Please help to improve this article by introducing more precise citations. ( October 2017 ) ( Learn how and when to remove this template message ) Singleton Merten syndrome Other names Singleton-Merten dysplasia Singleton Merten syndrome is inherited in an autosomal dominant manner Singleton Merten Syndrome is an autosomal dominant genetic disorder with variable expression with an onset of symptoms during childhood . ... You can help by adding to it . ( August 2017 ) Sources [ edit ] Singleton, EB, Merten DF: An unusual syndrome of widened medullary cavities of the metacarpals and phalanges, aortic calcification and abnormal dentition, Pediatric Radiol 1:2, 1973. [1] Resources form the National Institutes of Health [2] WebMD information References [ edit ] ^ Ferreira CR, Crow YJ, Gahl WA, Gardner PJ, Goldbach-Mansky R, Hur S, de Jesús AA, Nehrebecky M, Park JW, Briggs TA (2018) DDX58 and classic Singleton-Merten syndrome.
Rowell's Syndrome was described by Professor Neville Rowell and colleagues in 1963. ... "Rowell's syndrome". Clinical and Experimental Dermatology . 24 (2): 74–7. doi : 10.1046/j.1365-2230.1999.00422.x . ... "Lupus Erythematosus and Erythema Multiforme-like Lesions: A Syndrome With Characteristic Immunological Abnormalities". ... Duarte AF, Mota A, Pereira M, Baudrier T, Azevedo F (2008). "Rowell syndrome - case report and review of the literature". ... Lee A, Batra P, Furer V, Cheung W, Wang N, Franks A (2009). "Rowell syndrome (systemic lupus erythematosus + erythema multiforme)" .
Rosenthal–Kloepfer syndrome Other names Familial pachydermoperiostosis Specialty Dermatology Rosenthal–Kloepfer syndrome , is a cutaneous condition characterized by abnormal growth of bone and skin , coupled with clouding of the cornea . [1] It was described in 1962. [2] Another name for the condition is Acromegaly-cutis verticis gyrata-corneal leukoma syndrome. ... Diagnosis [ edit ] Radiographic imaging reveals thickening of bones, especially of the skull , and widening of the bones in the fingers . [4] See also [ edit ] Amniotic band syndrome List of cutaneous conditions References [ edit ] ^ "Rosenthal-Kloepfer Syndrome | Hereditary Ocular Diseases" . disorders.eyes.arizona.edu . ... "An acromegaloid, cutis verticis gyrata, corneal leukoma syndrome. A new medical entity" . Arch. ... Archived from the original on 2012-03-06. ^ "Rosenthal-Kloepfer Syndrome | Hereditary Ocular Diseases" . disorders.eyes.arizona.edu . Retrieved 2018-02-27 . ^ "Rosenthal-Kloepfer Syndrome | Hereditary Ocular Diseases" . disorders.eyes.arizona.edu .
Clinical Features Rosenthal and Kloepfer (1962) described a 'new' syndrome with these three features in 13 persons of 4 generations of a Louisiana black family.