-
Generalized Anxiety Disorder
Wikipedia
This has led to the continuation of GAD being medicated heavily with SSRIs. [25] Risk factors [ edit ] Genetics, family and environment [ edit ] The relationship between genetics and anxiety disorders is an ongoing area of research. [12] It is broadly understood that there exists an hereditary basis for GAD, but the exact nature of this hereditary basis is not fully appreciated. [7] While investigators have identified several genetic loci that are regions of interest for further study, there is no singular gene or set of genes that have been identified as causing GAD. [12] Nevertheless, genetic factors may play a role in determining whether an individual is at greater risk for developing GAD, [28] structural changes in the brain related to GAD, [29] or whether an individual is more or less likely to respond to a particular treatment modality. [28] Genetic factors that may play a role in development of GAD are usually discussed in view of environmental factors (e.g., life experience or ongoing stress) that might also play a role in development of GAD. [10] The traditional methods of investigating the possible hereditary basis of GAD include using family studies and twin studies (there are no known adoption studies of individuals who suffer anxiety disorders, including GAD [10] ). [7] [10] Meta-analysis of family and twin studies suggests that there is strong evidence of a hereditary basis for GAD in that GAD is more likely to occur in first-degree relatives of individuals who have GAD than in non-related individuals in the same population. [10] Twin studies also suggest that there may be a genetic linkage between GAD and major depressive disorder (MDD), which may explain the common occurrence of MDD in individuals who suffer GAD (e.g., comorbidity of MDD in individuals with GAD has been estimated at approximately 60% [30] ). [7] [31] When GAD is considered among all anxiety disorders (e.g., panic disorder, social anxiety disorder), genetic studies suggest that hereditary contribution to the development of anxiety disorders amounts to only approximately 30-40%, which suggests that environmental factors are likely more important to determining whether an individual may develop GAD. [7] [10] In regard to environmental influences in the development of GAD, it has been suggested that parenting behaviour may be an important influence since parents potentially model anxiety-related behaviours. [7] It has also been suggested that individuals who suffer GAD have experienced a greater number of minor stress-related events in life and that the number of stress-related events may be important in development of GAD (irrespective of other individual characteristics). [7] Studies of possible genetic contributions to the development of GAD have examined relationships between genes implicated in brain structures involved in identifying potential threats (e.g., in the amygdala ) and also implicated in neurotransmitters and neurotransmitter receptors known to be involved in anxiety disorders. [29] More specifically, genes studied for their relationship to development of GAD or demonstrated to have had a relationship to treatment response include: PACAP (A54G polymorphism): remission after 6 month treatment with Venlafaxine suggested to have a significant relationship with the A54G polymorphism (Cooper et al. (2013)) [29] HTR2A gene (rs7997012 SNP G allele): HTR2A allele suggested to be implicated in a significant decrease in anxiety symptoms associated with response to 6 months of Venlafaxine treatment (Lohoff et al. (2013)) [29] SLC6A4 promoter region (5-HTTLPR): Serotonin transporter gene suggested to be implicated in significant reduction in anxiety symptoms in response to 6 months of Venlafaxine treatment (Lohoff et al. (2013)) [29] Pathophysiology [ edit ] Amygdala (in red) brain structures linked to anxiety disorders The pathophysiology of GAD is an active and ongoing area of research often involving the intersection of genetics and neurological structures. [32] Generalized anxiety disorder has been linked to changes in functional connectivity of the amygdala and its processing of fear and anxiety. [13] Sensory information enters the amygdala through the nuclei of the basolateral complex (consisting of lateral, basal and accessory basal nuclei). [13] The basolateral complex processes the sensory-related fear memories and communicates information regarding threat importance to memory and sensory processing elsewhere in the brain, such as the medial prefrontal cortex and sensory cortices. [13] Neurological structures traditionally appreciated for their roles in anxiety include the amygdala, insula and orbitofrontal cortex (OFC). [32] It is broadly postulated that changes in one or more of these neurological structures are believed to allow greater amygdala response to emotional stimuli in individuals who have GAD as compared to individuals who do not have GAD. [32] Individuals who GAD have been suggested to have greater amygdala and medial prefrontal cortex (mPFC) activation in response to stimuli than individuals who do not have GAD. [32] However, the exact relationship between the amygdala and the frontal cortex (e.g., prefrontal cortex or the orbitofrontal cortex (OFC)) is not fully understood because there are studies that suggest increased or decreased activity in the frontal cortex in individuals who have GAD. [32] Consequently, because of the tenuous understanding of the frontal cortex as it relates to the amygdala in individuals who have GAD, it an open question as to whether individuals who have GAD bear an amygdala that is more sensitive than an amygdala in an individual without GAD or whether frontal cortex hyperactivity is responsible for changes in amygdala responsiveness to various stimuli. [32] Recent studies have attempted to identify specific regions of frontal cortex (e.g., dorsomedial prefrontal cortex (dmPFC)) that may be more or less reactive in individuals who have GAD [32] or specific networks that may be differentially implicated in individuals who have GAD. [13] Other lines of study investigate whether activation patterns vary in individuals who have GAD at different ages with respect to individuals who do not have GAD at the same age (e.g., amygdala activation in adolescents with GAD). [32] Treatment [ edit ] Traditional treatment modalities broadly fall into two (2) categories - i.e., psychotherapeutic and pharmacological intervention . [14] In addition to these two conventional therapeutic approaches, areas of active investigation include complementary and alternative medications (CAMs), brain stimulation, exercise, therapeutic massage and other interventions that have been proposed for further study. [33] Treatment modalities can, and often are utilized concurrently so that an individual may pursue psychological therapy (i.e., psychotherapy) and pharmacological therapy. [34] Both cognitive behavioral therapy (CBT) and medications (such as SSRIs ) have been shown to be effective in reducing anxiety. ... , National Institute of Mental Health. Accessed 28 May 2008. ^ Torpy, Janet M.; Burke, AE; Golub, RM (2011). ... "Establishing a common metric for self-reported anxiety: linking the MASQ, PANAS, and GAD-7 to PROMIS Anxiety" . Journal of Anxiety Disorders . 28 (1): 88–96. doi : 10.1016/j.janxdis.2013.11.006 . ... PMID 22865617 . ^ a b c "The Numbers Count" Archived 2014-07-28 at the Wayback Machine , National Institute of Mental Health. Accessed 28 May 2007. ^ a b Lieb, Roselind; Becker, Eni; Altamura, Carlo (2005).ZNF462, GAD1, GAD2, SLC30A10, SLC30A8, BDNF, ATF7IP, CRP, OPN1SW, SLC6A4, INS, HTR2A, SCLY, COMT, TAL1, HTR1A, NR3C1, IFNG, MAOA, LINC02210-CRHR1, DRD2, KRT7, OSR1, CAT, CRHR1, TPO, THAS, RBM14, THBS2, TNF, WASF2, TPH1, SMC2, BMS1, TWIST1, HGS, PSMG1, CDK5R1, WASF1, PHOX2B, BCAR1, CACYBP, TPPP, COBL, MIR4505, RBM14-RBM4, MIR663A, NPSR1, CACNA1G-AS1, ASPRV1, DYNLL2, TSACC, TP53INP1, STK32B, TMED9, PYCARD, PTPN22, KANK2, MMD, TFPI, ACACA, SOD1, CISH, GDNF, GCK, ERBB2, DUSP2, ATN1, DRD3, CSTA, KLF6, CECR, SLC6A12, BCL2, ARSD, STS, AMY1C, AMY1B, AMY1A, ALAD, TLE5, HARS1, HLA-DQB1, HRES1, IAPP, SLC6A3, SLC6A1, SRSF5, SET, RGS2, ADCYAP1R1, PON1, PDE1A, PAWR, PAM, OPRM1, NPY, NDUFS4, LTBP3, LCN2, IL18, IL4, PSMD9

-
Febrile Seizure
Wikipedia
Similarly, the prognosis after a complex febrile seizure is excellent, although an increased risk of death has been shown for complex febrile seizures, partly related to underlying conditions. [28] Epidemiology [ edit ] Febrile seizures happen between the ages of 6 months and 5 years. [1] [3] [29] The peak age for a febrile seizure is 18 months, with the most common age range being 12–30 months of age. [30] They affect between 2-5% of children. [1] [3] [29] They are more common in boys than girls. [12] [6] Febrile seizures can occur in any ethnic group, although there have been higher rates in Guamanians (14%), Japanese (6-9%) and Indians (5-10%). [31] References [ edit ] ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj Graves RC, Oehler K, Tingle LE (January 2012). ... National Institute of Neurological Disorders and Stroke" . www.ninds.nih.gov . Archived from the original on 28 July 2017 . Retrieved 9 August 2017 .SCN1A, GABRG2, SCN2A, SCN1B, STX1B, ANO3, IMPA2, HCN1, SLC12A5, IL1B, PIGH, HCN2, AVP, NPY, GOT1, GOT2, CASP12, ACTB, ADGRV1, CPA6, SCN9A, GABRD, GABRB3, CD46, GRIN2A, CHD2, DYRK1A, GABRA1, IFI44L, PCDH19, TRNK, ACADM, MBD5, VPS11, KCNQ3, TBC1D24, KCNA1, NEUROD2, PIGP, SLC35C1, SLC6A3, CACNA1H, JRK, CASK, CPLX1, TBCD, STXBP1, CDKL5, ERLIN2, PNKP, SLC6A1, ASXL2, SLC2A1, SCN8A, RPS6KA3, CILK1, POGZ, SRPX2, RSRC1, PHIP, SETD5, IL6, PIGQ, EFHC1, GPT2, TRIM8, SIK1, KCTD7, ARX, RNU12, CLCN2, CHAT, GLS, GNAO1, GRIN1, SLC25A22, CACNB4, CACNA1A, MBOAT7, MIR29B2CHG, AUH, ATP1A3, SCN1A-AS1, APP, ANO3-AS1, HS6ST2, PRRT2, IL1A, IL10, TNF, IL1RN, APOE, HMGB1, IL1R1, FEB1, IL4, FGF13, DPP4, FEB2, CXCL8, CHRNA4, MEF2C, MMP9, TIMP1, IFNG, GAS5, ZGLP1, RECQL4, LGI1, ZBED1, P2RX5-TAX1BP3, AP3M2, HEMGN, MIR223, STK38, MIR146A, SLC17A7, GKN1, EHMT1, PREX2, P2RX2, SEZ6, TBC1D9, NLRP3, P2RX6, MARCHF1, ENOSF1, CAPNS2, CHPF, ABCB1, ARID1A, DNMT1, HRC, GRM1, GRIN2B, GLP1R, GCG, GABRA5, GABBR1, FGF2, PTK2B, EZH2, EMP1, DPT, DNMT3A, CSNK1G2, SLC30A3, CSF2, CRH, CNR1, CLCN6, CALB2, CA11, CA7, CA3, C3, BDNF, BAX, ATP1A2, AKT1, IFNA1, IFNB1, IL6R, CXCL10, VWF, TRPV1, TRPC3, TGFB1, SPARC, SOX2, SLC8A3, RIT1, PTGS2, PTGER3, PRKCD, ACHE, PAK1, P2RY2, P2RY1, P2RX7, P2RX5, P2RX4, P2RX3, P2RX1, NFYC, COX2, MRC1, MEFV, MECP2, LAMC2, KCNQ2, MTCO2P12

-
Child Sex Tourism
Wikipedia
Another US State Department report states (page 85) "In a newer trend, some arranged fishing expeditions to the Amazon were organized for the purpose of child sex tourism for European and American exploiters." [25] Recent Reports on Fox Atlanta and ABC World News Tonight have helped shine the light on this. [26] [27] [28] [29] [30] ECPAT-USA has recently posted a Brazilian National News story with English subtitles. [31] Webcam child sex tourism [ edit ] According to the Federal Bureau of Investigations estimate, there are 750,000 predators online at any given time in 40,000 public chat rooms. ... These islands have also been destinations for sex trafficking. [39] Under a Criminal Code in Indonesia, any Indonesian citizen can be punished for violating the Child Protection Act or the Criminal Code, whether it is inside Indonesia or outside. [39] The Child Protect Act 28 is a general act to protect the rights of children. [39] A few specific sections provide laws specific to sexual mistreatment of children. ... Citizens of the Russian Federation and stateless persons permanently residing in the Russian Federation who have committed outside the Russian Federation a crime against the interests guarded by the present Code shall be subject to criminal liability in accordance with the present Code, unless a decision of a foreign state's court exists concerning this crime in respect of these persons". [61] Federal Act No. 380-FZ of 28 December 2013 amended the Criminal Code by also adding laws regarding the receiving of sexual services from a minor. ... Christian Science Monitor. Archived from the original on 28 February 2006. ^ a b c Brittainy Bacon (27 July 2007). ... Retrieved 5 February 2014 . ^ "Official: More than 1M child prostitutes in India" . CNN . 11 May 2009 . Retrieved 28 April 2010 . ^ "LA_Brazils_Child_Prostitution_Crisis" .
-
Tension Headache
Wikipedia
A 2006 systematic review found no rigorous evidence supporting manual therapies for tension headache. [27] A 2005 structured review found only weak evidence for the effectiveness of chiropractic manipulation for tension headache, and that it was probably more effective for tension headache than for migraine. [28] A 2004 Cochrane review found that spinal manipulation may be effective for migraine and tension headache, and that spinal manipulation and neck exercises may be effective for cervicogenic headache . [29] Two other systematic reviews published between 2000 and May 2005 did not find conclusive evidence in favor of spinal manipulation. [30] A 2012 systematic review of manual therapy found that hands-on work may reduce both the frequency and the intensity of chronic tension-type headaches. [31] More current literature also appears to be mixed however, CTTH patients may benefit from massage and physiotherapy as suggested by a systemic review examining these modalities via RCTs specifically for this patient population [32] Despite being helpful, the review also makes a point to note that there is no difference in effectiveness long term (6 months) between those CTTH patients utilizing TCAs and physiotherapy. [32] Another systemic review comparing manual therapy to pharmacologic therapy also supports little long term difference in outcome regarding TTH frequency, duration, and intensity. [33] Epidemiology [ edit ] As of 2016 tension headaches affect about 1.89 billion people [34] and are more common in women than men (23% to 18% respectively). [7] Despite its benign character, tension-type headache, especially in its chronic form, can impart significant disability on patients as well as burden on society at large. [6] References [ edit ] ^ a b Derry S, Wiffen PJ, Moore RA, Bendtsen L (July 2015). ... Retrieved 2019-01-12 . ^ a b c d e f g h i Consumer Reports (28 April 2016). "Tension Headache Treatment and Prevention" .

-
Rectal Prolapse
Wikipedia
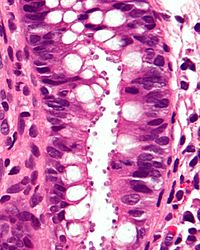
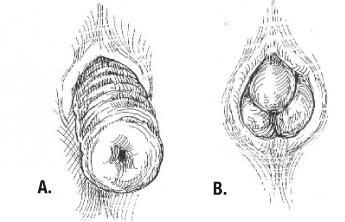
However, internal intussusception rarely progresses to external rectal prolapse. [27] The factors that result in a patient progressing from internal intussusception to a full thickness rectal prolapse remain unknown. [5] Defecography studies demonstrated that degrees of internal intussusception are present in 40% of asymptomatic subjects, raising the possibility that it represents a normal variant in some, and may predispose patients to develop symptoms, or exacerbate other problems. [28] Treatment [ edit ] Conservative [ edit ] Surgery is thought to be the only option to potentially cure a complete rectal prolapse. [6] For people with medical problems that make them unfit for surgery, and those who have minimal symptoms, conservative measures may be beneficial. ... Internal rectal intussusception [ edit ] Internal rectal intussusception (rectal intussusception, internal intussusception, internal rectal prolapse, occult rectal prolapse, internal rectal procidentia and rectal invagination) is a medical condition defined as a funnel shaped infolding of the rectal wall that can occur during defecation . [8] This phenomenon was first described in the late 1960s when defecography was first developed and became widespread. [5] Degrees of internal intussusception have been demonstrated in 40% of asymptomatic subjects, raising the possibility that it represents a normal variant in some, and may predispose patients to develop symptoms, or exacerbate other problems. [28] Symptoms [ edit ] Internal intussusception may be asymptomatic , but common symptoms include: [3] Fecal leakage [30] Sensation of obstructed defecation ( tenesmus ). [31] Pelvic pain. [3] Rectal bleeding . [3] Recto-rectal intussusceptions may be asymptomatic , apart from mild obstructed defecation.BMPR1A, RFC2, NSUN2, BCOR, MLXIPL, TBL2, TAB2, GTF2IRD1, BAZ1B, LTBP4, NAA10, CLIP2, CFTR, TGFB1, STK11, RPS6KA3, CCBE1, ELN, FCGR2A, GTF2I, LIMK1, LIG4, PTEN, REG1A, GAB2, BPIFA2, RAPH1, MRTFA, EPHB2, CRIM1, GPR4, FBLN5, RIDA, IL10, TCL1B, MMP1, TCL1A, MSMB, TNXB, TNXA, PLAU, MAPK1, STXBP3, PSPN, PSPH, TIMP1
-
Coma
Wikipedia
Some patients who have entered a vegetative state go on to regain a degree of awareness and in some cases, may remain in vegetative state for years or even decades (the longest recorded period being 42 years). [28] [29] Predicted chances of recovery will differ depending on which techniques were used to measure the patient's severity of neurological damage. ... Wijdicks studied 30 films (made between 1970 and 2004) that portrayed actors in prolonged comas, and he concluded that only two films accurately depicted the state of a coma victim and the agony of waiting for a patient to awaken: Reversal of Fortune (1990) and The Dreamlife of Angels (1998). The remaining 28 were criticized for portraying miraculous awakenings with no lasting side effects, unrealistic depictions of treatments and equipment required, and comatose patients remaining muscular and tanned. [34] Bioethics [ edit ] A person in a coma is said to be in an unconscious state. ... ISSN 1937-5239 . ^ a b Farisco, Michele (2016-04-28). Neurotechnology and Direct Brain Communication . doi : 10.4324/9781315723983 .CPS1, ATP1A2, TSHB, OXT, GCG, CYP2D6, CACNA1A, RANBP2, HNF1A, ABCC8, STAT3, SLC22A5, ACADM, PRF1, PLAGL1, PCCB, PCCA, OTC, NOTCH3, NDUFS4, MMUT, POLG, UCP2, MC2R, HYMAI, MMAB, MMAA, NAGS, NAXE, SLC19A3, MCCC2, MCCC1, KYNU, CFHR3, TRDN, SLC25A15, SLC25A13, EIF2AK3, SLC7A7, MEN1, IVD, KCNJ11, BCKDHA, CPT2, CPT1A, SLC25A20, BTD, BRAF, BCKDHB, AUH, DBT, ATP7B, ASS1, ASPA, ASL, APP, ALDOB, ACAT1, CTNNB1, FBP1, CFH, PDX1, INSR, INS, HNF4A, HMGCL, HLCS, CFHR1, HADHB, HADHA, GK, GCK, GCDH, ZFP57, TTR, PRNP, APOE, ABCD2
-
Laminopathy
Wikipedia
The exact dosage of lamin B in cells appears to be crucial for nuclear integrity as increased expression of lamin B causes a degenerative phenotype in fruit flies and leads to abnormal nuclear morphology. [14] Autoimmune antibodies [ edit ] Antibodies against lamins are detected in the sera of some individuals with autoimmune diseases . [15] DNA repair [ edit ] A-type lamins promote genetic stability by maintaining the levels of proteins that have key roles in DNA double-strand break repair during the processes of non-homologous end joining and homologous recombination . [16] Mutations in lamin A (LMNA) cause Hutchinson–Gilford progeria syndrome, a dramatic form of premature aging. [12] Mouse cells deficient for maturation of prelamin A show increased DNA damage and chromosome aberrations and are more sensitive to DNA damaging agents. [17] The inability to adequately repair DNA damages when A-type lamins are defective is likely responsible for some of the aspects of premature aging. [ citation needed ] Diagnosis [ edit ] Types of known laminopathies and other nuclear envelopathies [ edit ] Syndrome OMIM ID Symptoms Mutation in Identified in Atypical Werner syndrome 277700 Progeria with increased severity compared to normal Werner syndrome Lamin A/C 2003 [18] Barraquer–Simons syndrome 608709 Lipodystrophy Lamin B2 2006 [8] Buschke–Ollendorff syndrome 166700 Skeletal dysplasia , skin lesions LEM domain containing protein 3 (lamin-binding protein) 2004 [19] Cardiomyopathy, dilated, with quadriceps myopathy 607920 Cardiomyopathy Lamin A/C 2003 [21] Charcot–Marie–Tooth disease , axonal, type 2B1 605588 Neuropathy Lamin A/C 2002 [22] Emery–Dreifuss muscular dystrophy , X-linked (EDMD) 310300 Skeletal and cardiac muscular dystrophy Emerin (lamin-binding protein) 1996, [23] 2000 [24] Emery–Dreifuss muscular dystrophy , autosomal dominant (EDMD2) 181350 Skeletal and cardiac muscular dystrophy Lamin A/C 1999 [25] Emery–Dreifuss muscular dystrophy , autosomal recessive (EDMD3) 604929 Skeletal and cardiac muscular dystrophy Lamin A/C 2000 [26] Familial partial lipodystrophy of the Dunnigan type (FPLD) 151660 Lipoatrophic diabetes Lamin A/C 2002 [27] Greenberg dysplasia 215140 Skeletal dysplasia Lamin B receptor 2003 [28] Hutchinson–Gilford progeria syndrome (HGPS) 176670 Progeria Lamin A/C 2003 [12] Leukodystrophy, demyelinating, adult-onset, autosomal dominant (ADLD) 169500 Progressive demyelinating disorder affecting the central nervous system Lamin B1 (tandem gene duplication) 2006 [14] Limb-girdle muscular dystrophy type 1B (LGMD1B) 159001 Muscular dystrophy of hips and shoulders, cardiomyopathy Lamin A/C 2000 [29] Lipoatrophy with diabetes, hepatic steatosis, hypertrophic cardiomyopathy, and leukomelanodermic papules (LDHCP) 608056 Lipoatrophic diabetes , fatty liver , hypertrophic cardiomyopathy , skin lesions Lamin A/C 2003 [30] Mandibuloacral dysplasia with type A lipodystrophy (MADA) 248370 Dysplasia and lipodystrophy Lamin A/C 2002 [9] Mandibuloacral dysplasia with type B lipodystrophy (MADB) 608612 Dysplasia and lipodystrophy Zinc metalloprotease STE24 (prelamin-processing enzyme) 2003 [31] Pelger–Huet anomaly (PHA) 169400 Myelodysplasia Lamin B receptor 2002 [32] Restrictive dermopathy , lethal 275210 Dermopathy Lamin A/C or Zinc metalloprotease STE24 (prelamin-processing enzyme) 2004 [13] Treatment [ edit ] Currently, there is no cure for laminopathies and treatment is largely symptomatic and supportive. ... Proc. Natl. Acad. Sci. U.S.A . 101 (28): 10428–33. Bibcode : 2004PNAS..10110428V . doi : 10.1073/pnas.0401424101 .

-
Bartonellosis
Wikipedia
ELISA (enzyme-linked immunosorbent assay) is another method that has been used to detect Bartonella, but it has a low sensitivity (17-35%). [14] Western blot for protein detection of Bartonella-associated proteins has also been reported, but this method does not show clear immunoreactive profiles. [14] PCR [ edit ] The CDC states that PCR testing from a single blood draw is not sufficiently sensitive for B. henselae testing, [13] and can result in high false negative rates [17] due to a small sample volume and levels below the limit of molecular detection. [14] Bartonella spp. are fastidious, slow-growing bacteria that are difficult to grow using traditional solid agar plate culture methods due to complex nutritional requirements and potentially a low number of circulating bacteria. [13] [17] [18] [19] [20] This conventional method of culturing Bartonella spp. from blood inoculates plated directly onto solid agar plates requires an extended incubation period of 21 days due to the slow growth rate. [13] [17] [21] Enrichment Culture [ edit ] Bartonella growth rates improve when cultured in an enrichment inoculation step in a liquid insect-based medium [18] [21] [22] such as Bartonella α-Proteobacteria Growth Medium (BAPGM) [17] or Schneider’s Drosophila-based insect powder medium. [21] [22] Several studies have optimized the growing conditions of Bartonella spp. cultures in these liquid media, with no change in bacterial protein expressions or host interactions in vitro . [21] [22] Insect-based liquid media supports the growth and co-culturing of at least seven Bartonella species, [14] [17] [21] [22] reduces bacterial culturing time and facilitates PCR detection and isolation of Bartonella spp. from animal and patient samples. [14] [17] [19] Research shows that DNA may be detected following direct extraction from blood samples and become negative following enrichment culture, thus PCR is recommended after direct sample extraction and also following incubation in enrichment culture. [17] Several studies have successfully optimized sensitivity and specificity by using PCR amplification (pre-enrichment PCR) and enrichment culturing of blood draw samples, followed by PCR (post-enrichment PCR) and DNA sequence identification. [19] [23] Serial Testing [ edit ] As Bartonella spp. infect at low levels and cycle between blood and tissues, [18] multiple blood draws over time may be necessary to detect infection. [24] Treatment [ edit ] Treatment of infections caused by Bartonella species include: [25] [26] Disease Adults Children Cat-scratch disease Azithromycin + Rifampin Unknown Retinitis Doxycycline + rifampin unknown Trench fever or chronic bacteremia by B. quintana Doxycycline + gentamicin unknown Bacillary angiomatosis Erythromycin or doxycycline Erythromycin Peliosis hepatis Erythromycin or doxycycline Erythromycin Endocarditis Doxycycline + gentamicin + rifampin or ceftriaxone + gentamicin Carrión's disease (acute phase) Ciprofloxacin or chloramphenicol Chloramphenicol + beta-lactam Carrión's disease (chronic phase) Rifampin or macrolides Rifampin or macrolides Some authorities recommend the use of azithromycin . [27] Epidemiology [ edit ] Carrión's disease , or Oroya fever, or Peruvian wart is a rare infectious disease found only in Peru , Ecuador , and Colombia . [28] It is endemic in some areas of Peru , [29] is caused by infection with the bacterium Bartonella bacilliformis , and transmitted by sandflies of genus Lutzomyia . ... Carrión developed the disease three weeks after the inoculation and kept a meticulous record of clinical symptoms and signs until the disease rendered him incapable of the task and he died at age 28 several weeks later—October 5, 1885.
-
Kawasaki Disease
Wikipedia
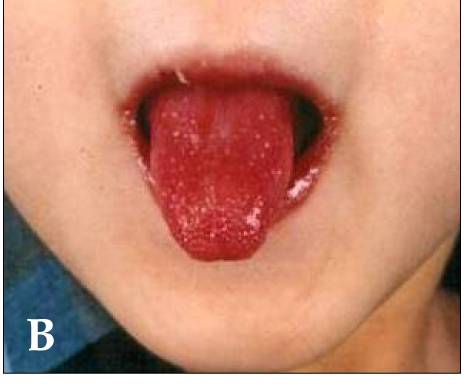
A disease found in young children Kawasaki disease Other names Kawasaki syndrome, [1] mucocutaneous lymph node syndrome [2] A child showing the characteristic " strawberry tongue " seen in Kawasaki disease [3] Specialty Pediatrics Symptoms Fever > 5 days, large lymph nodes , rash, sore throat , diarrhea [1] Complications Coronary artery aneurysms [1] Usual onset < 5 years old [1] Duration ~ 3 weeks [1] Causes Unknown [1] Risk factors Age of < 5 years old Diagnostic method Based on symptoms, ultrasound of the heart [1] Differential diagnosis Scarlet fever , juvenile rheumatoid arthritis , paediatric multisystem inflammatory syndrome [4] [1] Medication Aspirin , immunoglobulin [1] Prognosis Mortality 0.2% with treatment [3] Frequency 8–124 per 100,000 people under five [5] Kawasaki disease is a syndrome of unknown cause that results in a fever and mainly affects children under 5 years of age. [6] It is a form of vasculitis , where blood vessels become inflamed throughout the body. [1] The fever typically lasts for more than five days and is not affected by usual medications . [1] Other common symptoms include large lymph nodes in the neck, a rash in the genital area, and red eyes , lips, palms , or soles of the feet. [1] Within three weeks of the onset, the skin from the hands and feet may peel, after which recovery typically occurs. [1] In some children, coronary artery aneurysms form in the heart . [1] While the specific cause is unknown, it is thought to result from an excessive immune system response to an infection in children who are genetically predisposed . [6] It does not spread between people. [7] Diagnosis is usually based on a person's signs and symptoms. [1] Other tests such as an ultrasound of the heart and blood tests may support the diagnosis. [1] Diagnosis must take into account many other conditions that may present similar features, including scarlet fever and juvenile rheumatoid arthritis . [8] An emerging 'Kawasaki-like' disease temporally associated with COVID-19 [9] appears to be a distinct syndrome. [10] Typically, initial treatment of Kawasaki disease consists of high doses of aspirin and immunoglobulin . [1] Usually, with treatment, fever resolves within 24 hours and full recovery occurs. [1] If the coronary arteries are involved, ongoing treatment or surgery may occasionally be required. [1] Without treatment, coronary artery aneurysms occur in up to 25% and about 1% die. [3] [11] With treatment, the risk of death is reduced to 0.17%. [11] People who have had coronary artery aneurysms after Kawasaki disease require lifelong cardiological monitoring by specialized teams. [12] Kawasaki disease is rare. [1] It affects between 8 and 67 per 100,000 people under the age of five except in Japan, where it affects 124 per 100,000. [5] Boys are more commonly affected than girls. [1] The disorder is named after Japanese pediatrician Tomisaku Kawasaki , who first described it in 1967. [5] [13] Contents 1 Signs and symptoms 1.1 Cardiac 1.2 Other 2 Causes 2.1 Genetics 3 Diagnosis 3.1 Investigations 3.2 Subtypes 3.3 Case definition 3.4 Differential diagnosis 3.4.1 Kawasaki-like disease temporally associated with COVID-19 4 Classification 5 Treatment 6 Prognosis 7 Epidemiology 8 History 9 References 10 External links Signs and symptoms [ edit ] Kawasaki disease often begins with a high and persistent fever that is not very responsive to normal treatment with paracetamol (acetaminophen) or ibuprofen . [14] [15] This is the most prominent symptom of Kawasaki disease, and is a characteristic sign that the disease is in its acute phase; the fever normally presents as a high (above 39–40 °C) and remittent , and is followed by extreme irritability . [15] [16] Recently, it is reported to be present in patients with atypical or incomplete Kawasaki disease; [17] [18] nevertheless, it is not present in 100% of cases. [19] The first day of fever is considered the first day of the illness, [14] and its duration is typically one to two weeks; in the absence of treatment, it may extend for three to four weeks. [3] Prolonged fever is associated with a higher incidence of cardiac involvement. [20] It responds partially to antipyretic drugs and does not cease with the introduction of antibiotics . [3] However, when appropriate therapy is started – intravenous immunoglobulin and aspirin – the fever subsides after two days. [21] Bilateral conjunctival inflammation has been reported to be the most common symptom after fever. [22] [23] It typically involves the bulbar conjunctivae, is not accompanied by suppuration, and is not painful. [24] This usually begins shortly after the onset of fever during the acute stage of the disease. [14] Anterior uveitis may be present under slit-lamp examination . [25] [26] Iritis can occur, too. [27] Keratic precipitates are another eye manifestation (detectable by a slit lamp, but are usually too small to be seen by the unaided eye). [14] [28] Kawasaki disease also presents with a set of mouth symptoms, the most characteristic of which are a red tongue, swollen lips with vertical cracking, and bleeding. [29] The mucosa of the mouth and throat may be bright red, and the tongue may have a typical " strawberry tongue " appearance (marked redness with prominent gustative papillae ). [3] [30] These mouth symptoms are caused by necrotizing microvasculitis with fibrinoid necrosis . [29] Cervical lymphadenopathy is seen in 50% to 75% of children, whereas the other features are estimated to occur in 90%, [14] [22] but sometimes it can be the dominant presenting symptom. [28] [31] According to the diagnostic criteria, at least one impaired lymph node ≥ 15 mm in diameter should be involved. [30] Affected lymph nodes are painless or minimally painful, nonfluctuant, and nonsuppurative; erythema of the neighboring skin may occur. [14] Children with fever and neck adenitis who do not respond to antibiotics should have Kawasaki disease considered as part of the differential diagnoses . [14] Less common manifestations System Manifestations GIT Diarrhea , chest pain , abdominal pain , vomiting , liver dysfunction , pancreatitis , hydrops gallbladder , [32] parotitis , [22] [33] cholangitis , intussusception , intestinal pseudo-obstruction , ascites , splenic infarction MSS Polyarthritis and arthralgia CVS Myocarditis , pericarditis , tachycardia , [30] valvular heart disease GU Urethritis , prostatitis , cystitis , priapism , interstitial nephritis , orchitis , nephrotic syndrome CNS Lethargy , semicoma , [22] aseptic meningitis , and sensorineural deafness RS Shortness of breath , [30] influenza-like illness , pleural effusion , atelectasis Skin Erythema and induration at BCG vaccination site, Beau's lines , and finger gangrene Source: review, [30] table. [34] In the acute phase of the disease, changes in the peripheral extremities can include erythema of the palms and soles , which is often striking with sharp demarcation [14] and often accompanied by painful, brawny edema of the dorsa of the hands or feet, so affected children frequently refuse to hold objects in their hands or to bear weight on their feet. [3] [14] Later, during the convalescent or the subacute phase, desquamation of the fingers and toes usually begins in the periungual region within two to three weeks after the onset of fever and may extend to include the palms and soles. [35] Around 11% of children affected by the disease may continue skin-peeling for many years. [36] One to two months after the onset of fever, deep transverse grooves across the nails may develop ( Beau's lines ), [37] and occasionally nails are shed. [37] The most common skin manifestation is a diffuse macular - papular erythematous rash, which is quite nonspecific. [38] The rash varies over time and is characteristically located on the trunk; it may further spread to involve the face, extremities, and perineum. [3] Many other forms of cutaneous lesions have been reported; they may include scarlatiniform , papular, urticariform , multiform-like erythema , and purpuric lesions; even micropustules were reported. [39] [40] It can be polymorphic, not itchy , and normally observed up to the fifth day of fever. [41] However, it is never bullous or vesicular . [3] In the acute stage of Kawasaki disease, systemic inflammatory changes are evident in many organs. [42] Joint pain ( arthralgia ) and swelling, frequently symmetrical, and arthritis can also occur. [22] Myocarditis , [43] diarrhea , [30] pericarditis , valvulitis , aseptic meningitis , pneumonitis , lymphadenitis , and hepatitis may be present and are manifested by the presence of inflammatory cells in the affected tissues. [42] If left untreated, some symptoms will eventually relent, but coronary artery aneurysms will not improve, resulting in a significant risk of death or disability due to myocardial infarction . [30] If treated quickly, this risk can be mostly avoided and the course of illness cut short. [44] Signs and symptoms and time course of Kawasaki disease [14] [45] Other reported nonspecific symptoms include cough , rhinorrhea , sputum , vomiting , headache , and seizure . [22] The course of the disease can be divided into three clinical phases. [46] The acute febrile phase, which usually lasts for one to two weeks, is characterized by fever, conjunctival injection , erythema of the oral mucosa, erythema and swelling of the hands and feet, rash, cervical adenopathy, aseptic meningitis , diarrhea, and hepatic dysfunction . [30] Myocarditis is common during this time, and a pericardial effusion may be present. [14] Coronary arteritis may be present, but aneurysms are generally not yet visible by echocardiography . ... The Pediatric Infectious Disease Journal . 28 (6): 538–9. doi : 10.1097/INF.0b013e3181945984 .
-
Pedophilia
Wikipedia
Hendricks in 1997, sex offenders who are diagnosed with certain mental disorders, particularly pedophilia, can be subject to indefinite involuntary commitment . [19] Contents 1 Definitions 2 Signs and symptoms 2.1 Development 2.2 Comorbidity and personality traits 2.3 Child pornography 3 Causes 4 Diagnosis 4.1 DSM and ICD-11 4.2 Debate regarding criteria 5 Treatment 5.1 General 5.2 Cognitive behavioral therapy 5.3 Behavioral interventions 5.4 Sex drive reduction 6 Epidemiology 6.1 Pedophilia and child molestation 7 History 8 Law and forensic psychology 8.1 Definitions 8.2 Civil and legal commitment 9 Society and culture 9.1 General 9.2 Misuse of medical terminology 9.3 Pedophile advocacy groups 9.4 Anti-pedophile activism 10 See also 11 References 12 Further reading 13 External links Definitions The word pedophilia comes from the Greek παῖς, παιδός ( paîs, paidós ), meaning "child", and φιλία ( philía ), "friendly love" or "friendship". [20] Pedophilia is used for individuals with a primary or exclusive sexual interest in prepubescent children aged 13 or younger. [4] [5] Infantophilia is a sub-type of pedophilia; it is used to refer to a sexual preference for children under the age of 5 (especially infants and toddlers ). [21] [10] This is sometimes referred to as nepiophilia (from the Greek : νήπιος ( népios ) meaning "infant" or "child," which in turn derives from "ne-" and "epos" meaning "not speaking"), though this term is rarely used in academic sources. [22] [23] Hebephilia is defined as individuals with a primary or exclusive sexual interest in 11- to 14-year-old pubescents. [24] The DSM-5 does not list hebephilia among the diagnoses; while evidence suggests that hebephilia is separate from pedophilia, the ICD-10 includes early pubertal age (an aspect of hebephilia) in its pedophilia definition, covering the physical development overlap between the two philias. [25] In addition to hebephilia , some clinicians have proposed other categories that are somewhat or completely distinguished from pedophilia; these include pedohebephilia (a combination of pedophilia and hebephilia) and ephebophilia (though ephebophilia is not considered pathological). [26] [27] Signs and symptoms Development Pedophilia emerges before or during puberty, and is stable over time. [28] It is self-discovered, not chosen. [7] For these reasons, pedophilia has been described as a disorder of sexual preference, phenomenologically similar to a heterosexual or homosexual orientation. [28] These observations, however, do not exclude pedophilia from the group of mental disorders because pedophilic acts cause harm, and mental health professionals can sometimes help pedophiles to refrain from harming children. [29] In response to misinterpretations that the American Psychiatric Association considers pedophilia a sexual orientation because of wording in its printed DSM-5 manual, which distinguishes between paraphilia and what it calls "paraphilic disorder", subsequently forming a division of "pedophilia" and "pedophilic disorder", the association commented: "'[S]exual orientation' is not a term used in the diagnostic criteria for pedophilic disorder and its use in the DSM-5 text discussion is an error and should read 'sexual interest.'"
-
Sluggish Schizophrenia
Wikipedia
Petersburg academic psychiatrist professor Yuri Nuller notes that the concept of Snezhnevsky's school allowed psychiatrists to consider, for example, schizoid psychopathy and even schizoid character traits as early, delayed in their development, stages of the inevitable progredient process, rather than as personality traits inherent to the individual, the dynamics of which might depend on various external factors. [23] The same also applied to a number of other personality disorders. [23] It entailed the extremely broadened diagnostics of sluggish (neurosis-like, psychopathy-like) schizophrenia. [23] Despite a number of its controversial premises, but in line with the traditions of then Soviet science, Snezhnevsky's hypothesis immediately acquired the status of dogma, which was later overcome in other disciplines but firmly stuck in psychiatry. [24] Snezhnevsky's concept, with its dogmatism , proved to be psychologically comfortable for many psychiatrists, relieving them from doubt when making a diagnosis. [24] On the covert orders of the KGB , thousands of social and political reformers—Soviet dissidents—were incarcerated in mental hospitals after being labelled with diagnoses of sluggish schizophrenia. [25] Snezhnevsky himself diagnosed, or was otherwise involved in, a series of famous dissident cases, [19] and in dozens of cases he personally signed a commission decision on the legal insanity of dissidents who were in fact mentally healthy, including Vladimir Bukovsky , Natalya Gorbanevskaya , Leonid Plyushch , Mikola Plakhotnyuk , [26] and Pyotr Grigorenko . [27] Revaz Korinteli, a professor of the Grigol Robakidze University , says that Snezhnevsky broadened the borders of schizophrenia, and in this connection there was legal and theoretical justification for employing compulsory, involuntary treatment of dissenters in mental hospitals. [28] Premises for using the diagnosis [ edit ] According to the Global Initiative on Psychiatry chief executive Robert van Voren , the political abuse of psychiatry in the USSR arose from the concept that people who opposed the Soviet regime were mentally ill (since there was no logical reason to oppose the sociopolitical system considered the best in the world). [29] The diagnosis of sluggish schizophrenia furnished a framework for explaining this behavior. [29] This seemed to many Soviet psychiatrists a logical explanation for why someone would be willing to abandon his happiness, family, and career for a conviction so different from what most individuals seemed to believe. [17] Popularity of diagnosis [ edit ] Because of diagnoses of sluggish schizophrenia, Russia in 1974 had 5–7 cases of schizophrenia per 1,000 population, compared to 3–4 per 1,000 in the United Kingdom. [30] In the 1980s, Russia had three times as many schizophrenic patients per capita as the US, twice as many schizophrenic patients as West Germany , Austria and Japan , [31] and more schizophrenic patients than any Western country. [31] The city with the highest diagnosed prevalence of schizophrenia in the world was Moscow . [32] Along with paranoia , sluggish schizophrenia was the diagnosis most frequently used for the psychiatric incarceration of dissenters. [15] Darrel Regier of the National Institute of Mental Health , one of the U.S. experts who visited Soviet psychiatric hospitals in 1989, testified that a "substantial number" of political dissenters had been recognized as mentally sick on the basis of such symptoms as "anti-Soviet thoughts" or "delusions of reformism". [33] According to Moscow psychiatrist Alexander Danilin , the nosological approach in the Moscow psychiatric school established by Andrei Snezhnevsky (whom Danilin considered a state criminal) boiled down to the ability to diagnose schizophrenia. [34] Systematics by Snezhnevsky [ edit ] The Soviet model of schizophrenia is based on the hypothesis that a fundamental characteristic (by which schizophrenia spectrum disorders are distinguished clinically) is its longitudinal course. [35] The hypothesis implies three main types of schizophrenia: Continuous: unremitting, proceeding rapidly ("malignant") or slowly ("sluggish"), with a poor prognosis Periodic (or recurrent): characterized by an acute attack, followed by full remission with little or no progression Mixed ( German : schubweise ; in German, schub means "phase" or "attack"): mixture of continuous and periodic types which occurs periodically and is characterized by only partial remission. [35] The classification of schizophrenia types attributed to Snezhnevsky [36] is still used in Russia, [37] and considers sluggish schizophrenia an example of the continuous type. [38] The prevalence of Snezhnevsky's theories has particularly led to a broadening of the boundaries of disease such that even the mildest behavioral change is interpreted as indication of mental disorder. [39] Conditions posed as symptoms [ edit ] A carefully crafted description of sluggish schizophrenia established that psychotic symptoms were non-essential for the diagnosis, but symptoms of psychopathy , hypochondria , depersonalization or anxiety were central to it. [15] Symptoms considered part of the "negative axis" included pessimism , poor social adaptation and conflict with authorities, and were themselves sufficient for a formal diagnosis of "sluggish schizophrenia with few symptoms". [15] According to Snezhnevsky, patients with sluggish schizophrenia could present as seemingly sane but manifest minimal (and clinically relevant) personality changes which could remain unnoticed by the untrained eye . [15] Patients with non-psychotic mental disorders (or who were not mentally ill) could be diagnosed with sluggish schizophrenia. [15] Harold Merskey and Bronislava Shafran write that many conditions which would probably be diagnosed elsewhere as hypochondriacal or personality disorders, anxiety disorders or depressive disorders appear liable to come under the banner of slowly progressive schizophrenia in Snezhnevsky's system. [40] The incidence of sluggish schizophrenia increased because, according to Snezhnevsky and his colleagues, patients with this diagnosis were capable of socially functioning almost normally. [29] Their symptoms could resemble those of a neurosis or paranoia. [29] Patients with paranoid symptoms retained insight into their condition, but overestimated their significance and had grandiose ideas of reforming society. [29] Sluggish schizophrenia could have such symptoms as "reform delusions", "perseverance" and "struggle for the truth". [29] As Viktor Styazhkin reported, Snezhnevsky diagnosed a reform delusion in every case where a patient "develops a new principle of human knowledge, drafts an ideal of human happiness or other projects for the benefit of mankind". [41] During the 1960s and 1970s, theories which contained ideas about reforming society, struggling for the truth, and religious convictions were not considered delusional paranoid disorders in nearly any foreign classifications; however, Soviet psychiatry (for ideological reasons) considered critiques of the political system and proposals to reform it as delusional behavior. [42] The diagnoses of sluggish schizophrenia and paranoid states with delusions of reform were used only in the Soviet Union and several Eastern European countries . [43] An audience member at a lecture by Georgi Morozov on forensic psychiatry in the Serbsky Institute asked, “Tell us, Georgi Vasilevich, what is actually the diagnosis of sluggish schizophrenia?” ... Danilin, Alexander [Александр Данилин] . Тупик . Russkaya Zhizn . 28 March 2008 [Retrieved 21 April 2011]. ... Дело Косенко: лечение и возмещение ; 28 November 2012 [Retrieved 12 December 2012]. ... Дневник психиатра [The Psychiatrist's Diary] . 2014 [ archived 28 April 2014]:1–4. Russian. Snezhnevsky, Andrei [Андрей Снежневский] .
-
Tuberous Sclerosis
Wikipedia
The mTOR inhibitor everolimus was approved in the US for treatment of TSC-related tumors in the brain ( subependymal giant cell astrocytoma ) in 2010 and in the kidneys (renal angiomyolipoma ) in 2012. [23] [24] Oral everolimus (rapalog) reduces tumour size, is effective in terms of response to skin lesions and does not increase the risk of adverse events. [25] Everolimus also showed evidence of effectiveness at treating epilepsy in some people with TSC. [26] [27] In 2017, the European Commission approved everolimus for treatment of refractory partial-onset seizures associated with TSC. [28] Neurosurgical intervention may reduce the severity and frequency of seizures in TSC patients. [29] [30] Embolization and other surgical interventions can be used to treat renal angiomyolipoma with acute hemorrhage. ... "Analysis of 65 tuberous sclerosis complex (TSC) patients by TSC2 DGGE, TSC1/TSC2 MLPA, and TSC1 long-range PCR sequencing, and report of 28 novel mutations". Human Mutation . 26 (4): 374–83. doi : 10.1002/humu.20227 .TSC2, TSC1, IFNG, EIF4EBP1, PKD1, PIK3CB, TESC, SLC12A3, PIK3CD, PIK3CG, MTOR, PIK3CA, PTEN, AKT1, TP53, STK11, IGF1, RPS6KB1, DDIT4, TYMS, RASA1, OGG1, BRAF, IL1B, CCL26, VDR, IL6, PRKAA1, PRKAA2, PRKAB1, RHEB, MAPK1, GH1, PRKD1, MIR21, ABCB1, TBC1D7, PTGS2, BCL2L11, GRM5, COX2, MFAP1, MEN1, RGS6, NF1, FMR1, VIM, TERF2IP, PCNA, RABGEF1, CRTC1, VEGFA, VEGFC, PTPN4, MIR147B, MIR146A, MIR132, RPS6, C20orf181, TNF, RAP1A, FLCN, MTCO2P12, EGF, ABO, EPHB2, MAPK3, EGFR, APRT, DCX, LRPPRC, ST14, SPP1, AKT3, DEPDC5, STIM1, SPINT1, GRAP2, ADIPOQ, LILRB2, KLF4, STAT3, IRS2, CDK5R1, RIPK2, ELOC, TCOF1, GLRX3, CASK, IKBKG, SLC7A5, HMGA2, AIMP2, YWHAZ, YWHAB, TFRC, TRPC4, TYR, ZNRD2, ABCA4, AHSA1, WNT3A, ARID1B, RPTOR, CIP2A, GRHL3, IL21, NEUROG2, DHDDS, FUZ, COL18A1, CCDC8, BEX2, ORAI1, LINGO1, UBASH3B, CDCA5, DCTN6, PLB1, RMDN2, MARCHF10, HEXD, TICAM2, MIR142, MIR223, PIM3, OPN1MW2, IH, TMED7-TICAM2, FECD3, OPN1MW3, UPK3B, SLC12A5, RALGAPB, CHPT1, WDR45B, TNFSF13B, OGA, NES, UTS2, TRIM31, WDR45, PARK7, DKK1, TBC1D9, PHLPP1, RPGRIP1L, MLYCD, AMACR, PPP1R15A, RNF19A, POLDIP2, BEX3, LAT, SGSM3, NOX4, IL21R, IL22, TMED7, RMDN1, TLR7, TNFRSF12A, IL23A, RMDN3, SYBU, SOX9, PSMD9, SLC12A2, CTLA4, DBH, DECR1, NQO1, EIF4G1, EREG, PTK2B, FCN2, FLNA, FLT1, FLT4, GABPA, GC, GCHFR, OPN1MW, GFAP, GJA1, GCLC, GNA11, GNA12, GPT, GRN, GRIN2C, GSK3B, HCRT, HGF, HMBS, HRAS, CTNNB1, CCN2, SLC2A1, CSF2, ACTB, AGER, AKT2, AMELX, AMH, ANXA1, ANXA6, AQP4, ARNTL, ATM, KIF1A, CCND1, BCL2, OPN1SW, BDNF, BMP4, C1QBP, CANX, CBR1, CD8A, CDK7, CDKN2A, CDX2, CLN3, CMM, CRK, MAPK14, HTR2C, ICAM1, IFI27, IKBKB, TNFRSF11B, PRDX1, PAH, PAK2, PAM, PDCD1, PDGFRB, PEX13, PIK3C3, PITX1, PLA2G1B, PLCD1, PLG, PRRX1, POMC, ABL1, PTGS1, PVALB, RAP1GAP, RBBP4, S100A1, S100B, CCL2, CCL24, SDC2, SDHB, SHOX, NTF4, NTF3, NPC1, MME, IL4, IL6ST, CXCL8, IL12A, IL17A, ING2, INHA, IRF7, IRS1, KRAS, LAMC2, LIG4, MMP2, NOTCH1, MNAT1, MPP2, ABCC1, MYO1B, COX1, MTTP, MUC1, MYC, NFE2L2, NFKB1, NGF, NM, H3P23

-
List Of Periodontal Diseases
Wikipedia
Archived from the original (PDF) on 2010-11-28. ^ American Academy of Periodontology (1999). ... "Lymphocyte-fibroblast interaction in the pathogenesis of inflammatory gingival disease". Experientia . 28 (10): 1228–30. doi : 10.1007/BF01946188 .CTSC, PON1, IL17A, IL16, IL15, CD80, CD40LG, IL24, IL19, IL7, IL21, TNF, MMP8, IL10, IL6, IL1A, IL1B, NLRP3, VDR, TNFSF11, IL4, CRP, TLR4, VEGFA, IFNG, TNFRSF11B, FN1, PTGS2, CD14, IL1RN, COX2, MMP9, MTCO2P12, GCFC2, CAMP, TREM1, MPO, STAT1, SQSTM1, F2RL1, ALOX5, LRWD1, DEFB1, TGFB1, ADRB3, TLR2, IL18, CXCL10, GOPC, TREM2, TLR9, FBLIM1, WNT5A, PWAR1, CXCL8, SLC52A2, IL2RA, MIR146A, CDKN2B-AS1, IFI16, ICAM1, IBSP, ISG20, MMP3, LTA, LTF, VCAM1, SOCS1, DLK1, CCN6, TIMP3, HPD, SMPD1, CXCL12, CCL2, RARRES2, ADM, NR1I2, PLG, NOS3, AGO2, IL37, VSX1, TRIM25, MMP1, HSPD1, NAT2, PTX3, FOXO1, CD28, CASP9, COX8A, CTLA4, APOE, EGF, F2R, FGF2, CAT, HIF1A, MIR15A, PES1, DHS, SDS, BTF3P11, SLC7A9, WDHD1, PADI2, KDM4B, JMJD6, CAMTA1, SIRT1, ANGPTL2, MAPK8IP2, SEMA4D, PADI4, BSG, BPI, TRBV16, TRBV7-9, TRBC1, SETD2, PKN3, BDNF, DPP7, BCHE, PDPN, CRTAP, AHSG, AIM2, PEA15, MIR1226, IL18R1, CASP8, HDAC3, CASP3, CASP1, MSC, VAMP3, AGTR1, NTN1, CYTIP, GPNMB, PLPPR4, HDAC6, EDIL3, ARPC5, CTDSP2, EBI3, DDX39A, CTDSPL, EDS8, TLR6, NOD1, IL22, TRAT1, FOXP3, UNC5B, IL33, DNER, IL17F, ALPL, MRGPRX2, RBM45, ALOX15, IL34, ESCO2, MIR30E, TMPRSS6, ALDH2, CRACR2A, MIR22, IL27, PCSK9, COPD, FDCSP, IFNL1, BRINP3, SERPINA13P, RTL1, SMIM10L2A, MIR106B, SMIM10L2B, PPP1R2C, GAL, DRAM1, ANGPTL4, HSPA14, IL23A, CD19, AZU1, AR, KLK3, DEFA1B, FAM20A, ODAM, SLC52A1, ATF7IP, TET1, AMY1C, SLAMF7, CXCL16, NLRC4, MIR646, AMY1B, ACE2, TRPV4, NOD2, AMY1A, DHX40, IL17D, HLA-DRB1, RECK, FBN1, KIR3DL1, LBP, LGALS9, ESR1, LYZ, MBL2, MFGE8, MAP3K11, MARK2, MMP2, ELN, EGFR, MMP13, EDN1, MT2A, ECE1, MTNR1B, NFATC1, NFKB1, NFKBIL1, NHS, NOS2, RCAN1, NOTCH1, PNP, ITGB2, IRF1, OCA2, FCGR3A, HLA-DQB1, TNC, HGF, CFH, IRF8, HBB, GSTP1, IGFBP2, IGFBP3, IGHA1, GSR, GRN, GOT1, IL2, GIP, GHSR, GEM, FPR1, FOLR1, CXCR1, IL12RB2, IL13, FGF7, FGB, FCGR3B, NRAS, DMBT1, DDX39B, SLC6A4, CTSB, SNAP25, SOD2, SPG7, SPP1, STAT3, SYK, ADAM17, CST2, TRB, TRBV20OR9-2, CSF1, TGFB3, TH, THRB, CRYGD, CCR5, CCR1, TNFRSF1A, TNFRSF1B, CLU, CFTR, CD81, TLX2, CXCR4, SLIT3, SLC2A4, OTC, SLC2A1, P2RX7, SERPINE1, PECAM1, PIN1, PLAU, DEFB4A, PLTP, DEFA1, PPARG, HTRA1, ACE, CUX1, CTSS, REN, S100A2, S100A12, CTSK, CCL3, CCL7, CCL20, CTSD, SELE, SELL, SETMAR, SH3BP2, CD34

-
Mccarthyism
Wikipedia
The first recorded uses of the term "McCarthyism" were in the Christian Science Monitor on March 28, 1950 ("Their little spree with McCarthyism is no aid to consultation"); [18] and then, on the following day, in a political cartoon by Washington Post editorial cartoonist Herbert Block (Herblock). ... In many cases, they were not even told of what they were accused. [28] Hoover's influence extended beyond federal government employees and beyond the loyalty-security programs.

-
Vaginal Anomalies
Wikipedia
Sometimes a small border of hymenal tissue is left around the opening of the vagina. [25] Congenital adrenal hyperplasia can cause the abnormal development of the vagina. [26] [27] [28] Vaginal adenosis is the abnormal presence of cervical and uterine tissue within the wall of the vagina. [29] Ten percent of women have this condition and remain unsymptomatic. ... Pan African Medical Journal . 15 : 28. doi : 10.11604/pamj.2013.15.28.2251 .

-
Apathy
Wikipedia
Management of apathetic symptoms using methylphenidate has shown promise in randomized placebo controlled trials of Alzheimer's patients. [27] [28] [29] A phase III multi-centered randomized placebo-controlled trial of methylphenidate for the treatment of apathy is currently underway and planned for completion in August 2020. [30] Anxiety [ edit ] While apathy and anxiety may appear to be separate, and different, states of being, there are many ways that severe anxiety can cause apathy. ... Journal of Clinical Psychopharmacology . 28 (3): 296–301. doi : 10.1097/JCP.0b013e318172b479 .GRN, TBK1, MAPT, ACAT1, DNAJC6, TARDBP, ATP13A2, DNAJC13, PARK7, SQSTM1, CHMP2B, VCP, UCHL1, SPAST, SNCA, PSEN1, ATXN10, GIGYF2, PRKAR1B, COQ2, HTRA2, TREM2, TMEM106B, VPS13C, VPS35, JPH3, PINK1, EHMT1, LRRK2, HGSNAT, C9orf72, TMEM240, CHCHD10, PRNP, SMARCB1, PODXL, CACNA1A, FUS, DNMT1, GBA, PDGFB, DCTN1, GM2A, HEXA, CSF1R, HLA-DQB1, HMGCL, EIF4G1, PRKN, APOE, MCIDAS, ACHE, CSF2, SLC6A4, LAMC2, TLE5, SLC6A3, COMT, DRD1, USH1G, AR, BDNF, PRX, DRD3, CRP, PRND, DRD4, CFLAR, SGCA, MSN, SOD1, MC4R, LIPA, TRPV1, IGFALS, ENPEP, ADAMTS2, RAPGEF4, MAPK8IP3, HCRT, SMUG1, TPSG1, NPS

-
Female Genital Mutilation In The United States
Wikipedia
During the 19th and 20th centuries, the clitoris was considered the center of female sexuality. [4] In addition, Victorian concepts of female sexuality resulted in a widely-held belief that women were less sexual than men. [25] Female sexuality was typically thought of only within the constructs of heterosexual marriage, and behaviors that strayed from this schema, such as masturbation, were deemed symptomatic, and often resulted in operation on the clitoris. [26] [4] Depending on the symptoms and diagnosis, physicians performed four different procedures of varying invasiveness on women. [4] Doctors would either remove the smegma surrounding the clitoris, lacerate adhesions restricting the clitoris, or remove the clitoral hood altogether (female circumcision). [4] In the most extreme cases, doctors would perform a clitoridectomy, removing the clitoris entirely. [4] Reflex neurosis was a common diagnosis in the 19th century. [4] Characterized by excessive nervous stimulation, this condition could often manifest in an overstimulation of the clitoris that women would attempt to quell with masturbation. [4] Women diagnosed with reflex neurosis were often circumcised in an effort to remove the irritant. [4] From the 1880s to 1950s, excision was often performed to prevent and treat lesbianism, masturbation, depression, hysteria, and nymphomania. [27] [28] These procedures continued well into the 1970s, and were covered by Blue Cross Blue Shield Insurance until 1977. [7] Dr. ... Congress required the Department of Health and Human services to provide information for medical students about treatment recommendations. [30] Education policy was also included in the Illegal Immigration Reform and Immigrant Responsibility Act of 1996 . [31] The IIRARA mandated that visa recipients from 28 high-risk countries receive culturally appropriate information on the personal and legal repercussions of FGM in the United States at or before the time of entry. [31] [32] Prior to the Act being declared unconstitutional, FGM on anyone under the age of 18 had become a felony in the United States with the passage of the Female Genital Mutilation Act of 1996. [8] The law was introduced by former congresswoman Pat Schroeder in October 1993. [33] [34] The Female Genital Mutilation Act included education and community outreach programs that provide information about the physical and emotional harm caused by FGM. [8] [33] [35] In November 20, 2018, Federal Judge Barnard A.

-
Tooth Mobility
Wikipedia
Although occlusal trauma and excessive occlusal forces does not initiate periodontitis or cause loss of connective tissue attachment alone, there are certain cases where occlusal trauma can exacerbate periodontitis. [28] Moreover, pre-existing plaque-induced periodontitis can also cause occlusal trauma to increase the rate of connective tissue loss, [29] which in turn may increase tooth mobility. ... Indian Journal of Dental Research . 28 (1): 10–15. doi : 10.4103/ijdr.ijdr_8_16 .

-
Subcutaneous Emphysema
Wikipedia
Treatment [ edit ] Subcutaneous emphysema is usually benign . [1] Most of the time, SCE itself does not need treatment (though the conditions from which it results may); however, if the amount of air is large, it can interfere with breathing and be uncomfortable. [28] It occasionally progresses to a state "Massive Subcutaneous Emphysema" which is quite uncomfortable and requires surgical drainage. ... "Fournier gangrene: Role of imaging" . Radiographics . 28 (2): 519–528. doi : 10.1148/rg.282075048 .

-
Cryptosporidiosis
Wikipedia
B cells do not help with the initial response or the fight to eliminate the parasite. [25] Previous infection in immunocompetent individuals produces little resistance to future infection, however it may decrease the severity of disease and the number of oocysts excreted. [28] [29] Diagnosis [ edit ] There are many diagnostic tests for Cryptosporidium . ... "Prevalence of Cryptosporidium , microsporidia and Isospora infection in HIV-infected people: a global systematic review and meta-analysis" . Parasites & Vectors . 11 (1): 28. doi : 10.1186/s13071-017-2558-x . ... After an incubation period of 5–10 days (range 2–28 days), an infected individual develops watery diarrhea ... fever may be low grade or nonexistent; ... ... Archived from the original (PDF) on 28 September 2007 . Retrieved 6 May 2007 . ^ Korich DG, Mead JR, Madore MS, Sinclair NA, Sterling CR (May 1990). ... Principles and Practice of Infectious Diseases (6th ed.). Elsevier . pp. 3215–28. Upton, Steve J. (12 September 2003).IFNG, MBL2, BDNF, PTGES3, UNG, VAV1, CP20, BRAP, STK24, CDK5R1, PDPN, TMED10, TNF, DKK1, LAMP3, PLB1, TMED10P1, MIR221, CEMP1, CNE7, TPT1, TAC1, CD7, RRAS, CDC42, CCR5, HSPA4, ICAM1, IL1A, IL1B, IL4, IL10, IMPA1, KARS1, LSAMP, OXA1L, ABCB1, RAC1, RARG, H3P17